Resin-Based Composites
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
35 Terms
Composite
solid that contains two or more different component materials/phases that have physical properties (strength/elasticity) that are significantly changed then when in a homogenous material
Resin-base composite (RBC)
dental materials used for restorations, such as fillings, veneers, inlays, and crowns
Three historical classifications of development for composite
1)Bonding
2)Fillers
3)Curing
Bonding history
1)Unbound composite (shrink and pop out)
2)Acid etch and enamel bonding
3)Dentin-bonded composite
Filler history
1)Original development (large filler particles)
2)Smaller filler particles
3)Nanohybrid composite
Curing history
1)Self cured
2)UV cured
3)Visible light cured (LED)
Basic composition of composite (6)
1)Resin matrix
2)Filler particles
3)Coupling agent
4)Initiator/inhibitors
5)Pigment
6)Other (antibiotics/stain)
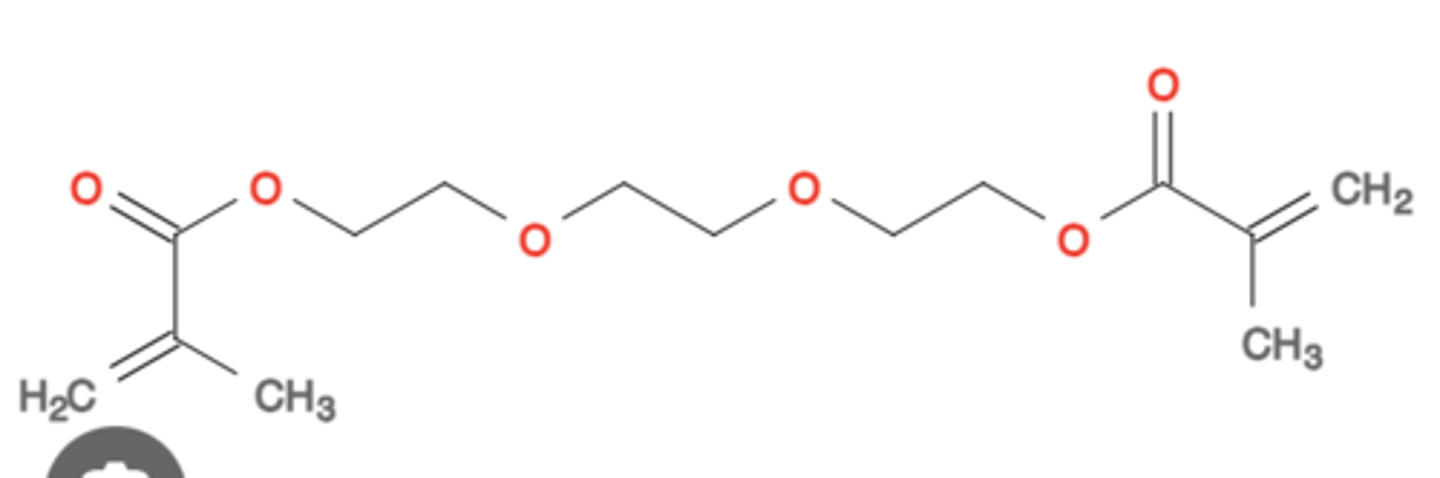
Resin matrix monomers
they are the scaffolding that provides shape and stiffness for composite
Ex/Bis-GMA and TEGMA
Bis-GMA
most common matrix monomer
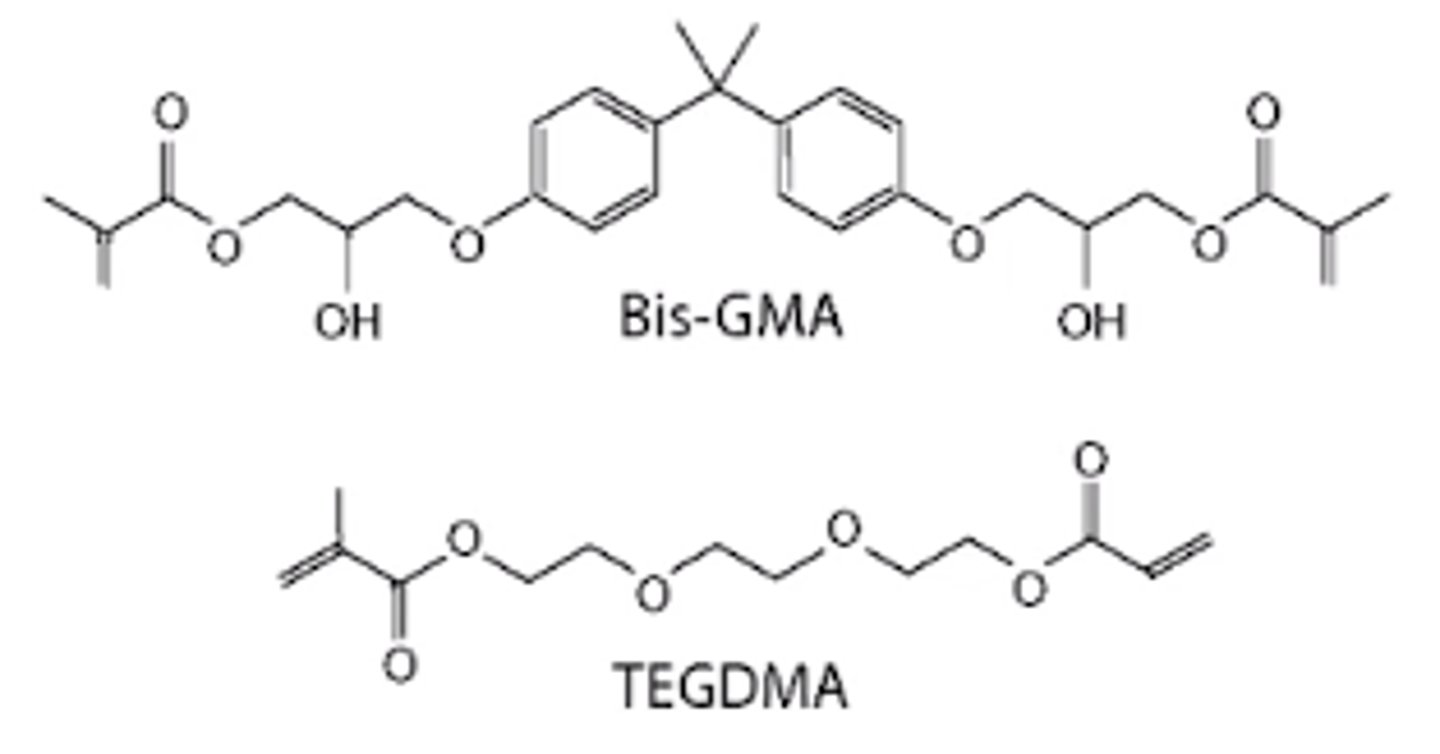
TEGMA
matrix monomer used to dilute Bis-GMA and allow for more particles/fillers
Filler particles
they reinforce the matrix, reduce shrinkage, reduce thermal expansion/contraction, decrease water sorption, radiopacity, and control workability/viscosity
Ex/quartz, glass Sol-gel ceramic, microfine silica, and silica nanoparticles
Coupling Agent (Silane)
provides bonding between inorganic filler particles and organic resin matrix to enhance mechanical properties and reduce clinical wear
Types of initiators (2)
1)Chemical initiators (redox)
2)Photo-initiators
Chemical initiator (redox)
polymerization begins when two components are mixed together, which releases a radical that breaks the double bond on the end of a monomer
Photo-initiator
Is a chemical/light that initiates the polymerization reaction. The key thing to remember here is that it takes the combination of the resin, photo-initiator, and the proper curing bulb to cause the gel to cure completely.
Inhibitors
prevent spontaneous polymerization to increase shelf-life and working time
Ex/Hydroquinone
Resin polymerization
causes shrinkage rate of 2-5.5%
Clinical implications of resin shrinkage (7)
1)Internal stress
2)Cusp deformities
3)Marginal gaps
4)Enamel cracks
5)Marginal leaks
6)Sensitivity
7)Secondary caries
Optical characteristics
multiple shades and translucency to appear like dentin/enamel
Classifications of resin-based composites
1)Filler particle (size/distribution)
2)Clinical usage (flowable/universal)
3)Polymerization reaction (light-cured, self-cured, dual-cured)
Filler particle classification (3)
1)Microfill
2)Mini/Midfill/Microhybrid
3)Nanofilled/Nanohybrid
Microfill
40-50 nm sized fillers, pre-polymerized with mixed monomers, polished, highest luster, smoothest surface, low stress bearing, and esthetic areas
Mini/Midfill or Microhybrid
<1μm sized filler, high strength, good wear, and used for anterior/posterior restorations
Nanofilled or Nanohybrid
<100 nm sized filler, high strength, esthetics, and polished
Clinical application classification (4)
1)Packable (high viscosity)
2)Flowable (low viscosity)
3)Conventional (regular viscosity)
4)Bulk-fill (conventional/low viscosity)
Packable composite
high viscosity, posterior teeth, difficult to adapt, rarely used, and similar to amalgam
Flowable composite
low viscosity, easy to adapt, inferior mechanical properties, and not load bearing
Convention composite
regular viscosity, universal composite, nanofiller/nanohybrid/microhybrid, higher resistance, low wear, load bearing, and increased polymerization shrinkage (stress)
Bulk-fill composite
conventional (high resistance and low wear) or low viscosity (low resistance and high wear), posterior restorations, reduced stress from polymerization shrinkage, and deeper curing depth
Type I polymerization restorative material
suitable for restorations of occlusal surfaces
Type II polymerization restorative material
suitable for restoration of all other surfaces besides occlusal surfaces
Class I restorative material
materials whose setting is initiated by mixing and initiator and activator (self-curing)
Class II restorative material
materials whose setting is initiated by application of external source (blue light/heat)
Group I: energy applied intra-orally
Group II: energy applied extra-orally
Class III restorative material
materials whose setting is initiated by an external energy source and also have self-curing mechanism (dual cure)
Desirable physical properties for composite (5)
1)Linear coefficient of thermal expansion (similar to teeth)
2)Water sorption (increase filler decrease water sorption)
3)Wear
4)Modulus of elasticity (increase filler increase stiffness)
5)Color stability (maintain color)