Newborn Eval -- first 28d of life
1/156
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
157 Terms
newborn phase
first 28d of life
newborn history
- review of current preg, L&D
- review of past pregnancy outcomes
- review of mothers and father's medical and genetic hx
- delivery of infant
most important review of moms hx
- maternal age, gravida, parity, blood type
- illnesses
- any pertinent positives (alcohol, substance abuse)
- moms GBS status
what happens to baby in delivery room
- placed on warmer, oropharynx and nose are suctioned, skin is dried
- brief exam (resp distress, cyanosis, cardiac exam, gestational age, med significant congenital abnorms)
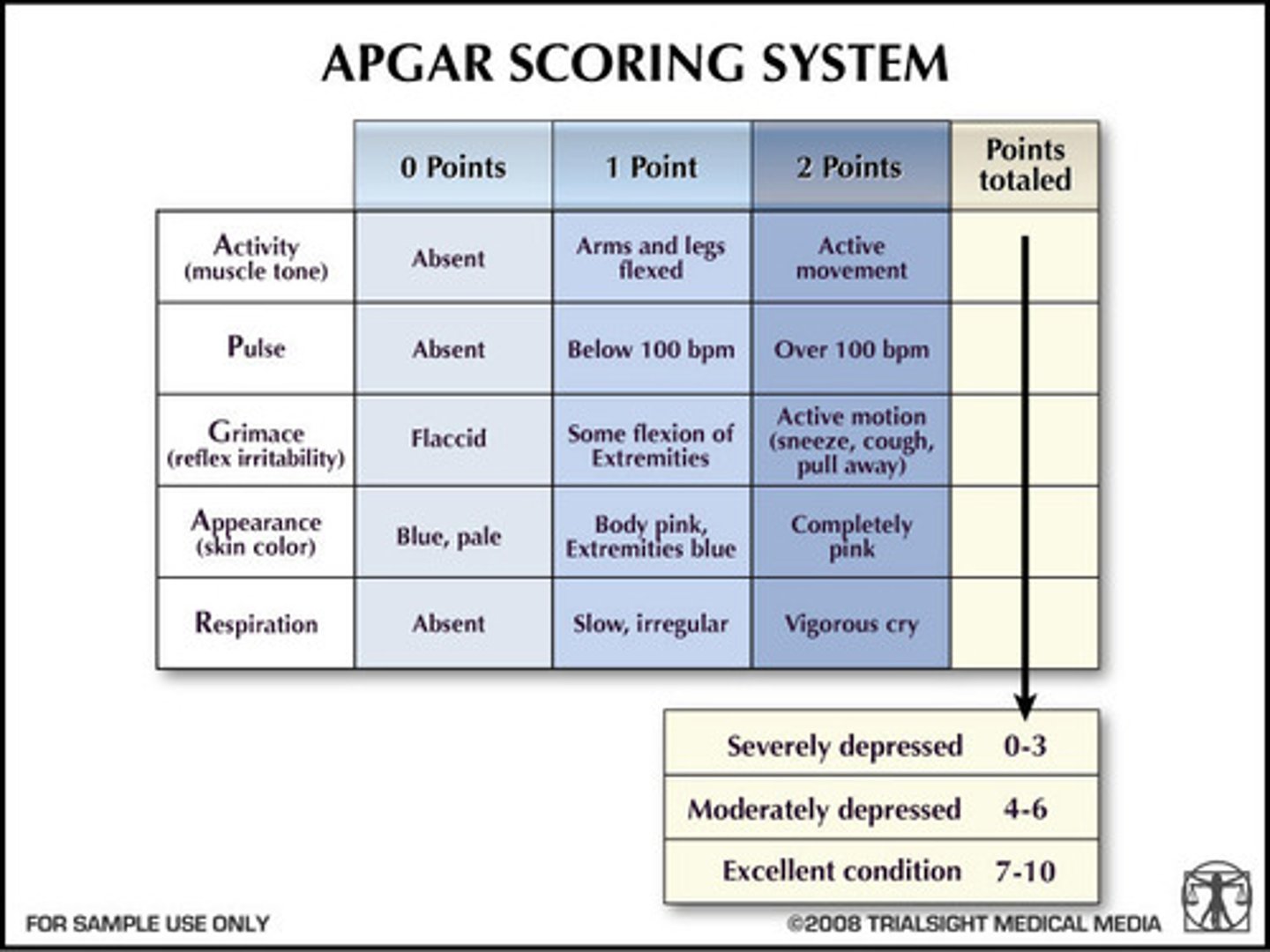
- APGAR score
apgar scoring
- at 1m and 5m
- if <7, continue scoring every 5m until >7
most reliable way to determine gestational age
knowing with certainty the LMP date
fetal u/s <22 wks also reliable
if neither u/s or LMP is reliable, how will you know gestational age
ballard score (postnatal)
physical indicators on the ballard score
Skin
Plantar creases
Breast appearance
Eyelids and Ear cartilage
Genitalia appearance
neuromuscular indicators on the ballard score
Posture
Active and Passive tone
Reflexes
___________ to eyes for prophylaxis to gonorrhea and chlamydia
erythromycin
___________to prevent hemorrhagic disease (due to deficiency of Vit K dependent factors: 2, 7, 9 and 10)
Vitamin K 1 mg IM
normal HR newborn
102 - 162 (50%ile is 120), HR may decrease in some infants to 85-90 during sleep
normal respirations in NB
35 - 60 (counted over 1 min)
avg temp of NB
97.7 to 99.5°F (axillary)
avg length of NB
average 20 inches (18 - 21.5) from top of head to bottom of feet with legs extended using a length board or measuring tape.
head circumference NB
ideal time to measure is 48 hrs after birth.
Measured from above the eyes and over the occipital bone prominence, may change in the first few days as molding and scalp edema resolve
avg weight NB
7.5 lbs (5.5 - 9.5, 5 - 95 %) without diaper or clothes
gestational age
# of weeks from 1st day of LMP
small for GA
- <10%ile for weight for their GA
cause of small baby
Can be caused by Congenital infection, maternal hypertension, maternal substance abuse, genetic syndrome
short term complication small baby
hypothermia and hypoglycemia
how long to most SGA infants catch up growth
by 2-4y
when are SGA infants more likely to remain small
when one or both parents are also small
large for GA (LGA)
>90th %ile for weight for their GA
associated maternal factors for LGA
-obesity, gestational diabetes, excessive gestational weight gain, certain genetic syndromes, AMA, post-term parity, multiparity
short term complications of LGA
hypoglycemia (should all be screened shortly after birth), birth injury (brachial plexus injury, clavicle fx), perinatal asphyxia, respiratory distress (TTN from C-section, meconium aspiration), polycythemia, , congenital anomalies
when does comprehensive exam of NB occur
on the day of delivery or the next morning.
what is reviewed at the NB comprehensive exam
baby's assigned sex, measurements (with percentiles) and VS should be reviewed .
general appearance of baby
Observation of the baby in the resting state should be observed before the exam.
acrocyanosis
blue hands and feet -- is common in first few days
indicates hypoxia and warrants immediate eval
Central cyanosis, bluish color to tongue, lips and mucous membranes
why might baby have facial bruise and pink lips
delivery
pallor in NB
anemia
ruddy color NB
polycythemia
jaundice
yellow baby
when is jaundice def abnormal
first 24 hr
respiratory disease in infant
rapid RR, nasal flaring, grunting or retractions suggest respiratory disease
how to note adequate intrauterine nutrition
subQ fat in NB
movement and position in NB baby
all extremities should move symmetrically. Abnormal movements and position may be from injury or deformation.
milia
white papules from retained keratin and sebum in follicles on nose and cheeks, may last 2 weeks
normal

Transient Pustular Melanosis
-superficial pustules overlying darker macules, usually in dark skinned babies

Erythema Toxicum
1-2mm white papules on erythematous base, filled with eosinophils, on body

Congenital Dermal Melanosis (Mongolian spots)
blue-grey or brown macules, usually over spine and buttocks. More typical in babies of African or Asian decent

Nevus Simplex (Salmon patches or Stork bite)
pink-red macule on upper eyelids, upper eyelid, forehead or nape of neck

Nevus Flammeus (Port Wine Stain)
low flow capillary malformation that can occur anywhere on the body

lanugo
a fine, soft hair that covers a fetus while developing in the womb, often appearing on newborns, especially premature babies

general inspection head and scalp
inspection for head shape and size, protuberances, lacerations and abrasions, swelling, lesions.
avg head size
Average is 35cm, Range 33-37cm
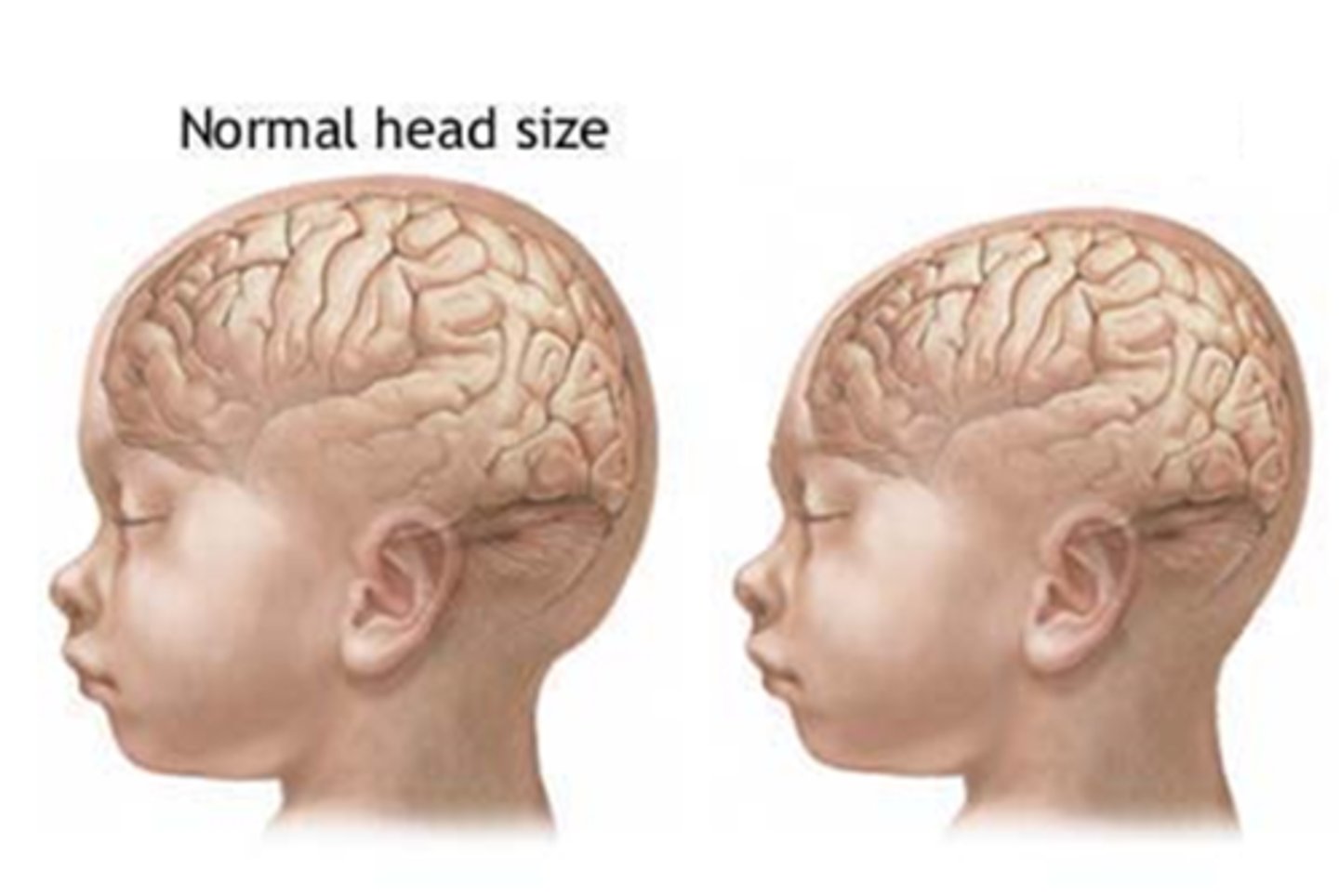
macrocephaly
HC>97%ile for GA , hydrocephalus or any enlargement of brain structure st

microcephaly
HC < 3%ile for GA, genetic, metabolic, toxic or infectious causes
fontanelles
usually flat
In an infant at rest, a bulging fontanelle can indicate hydrocephalus or meningitis
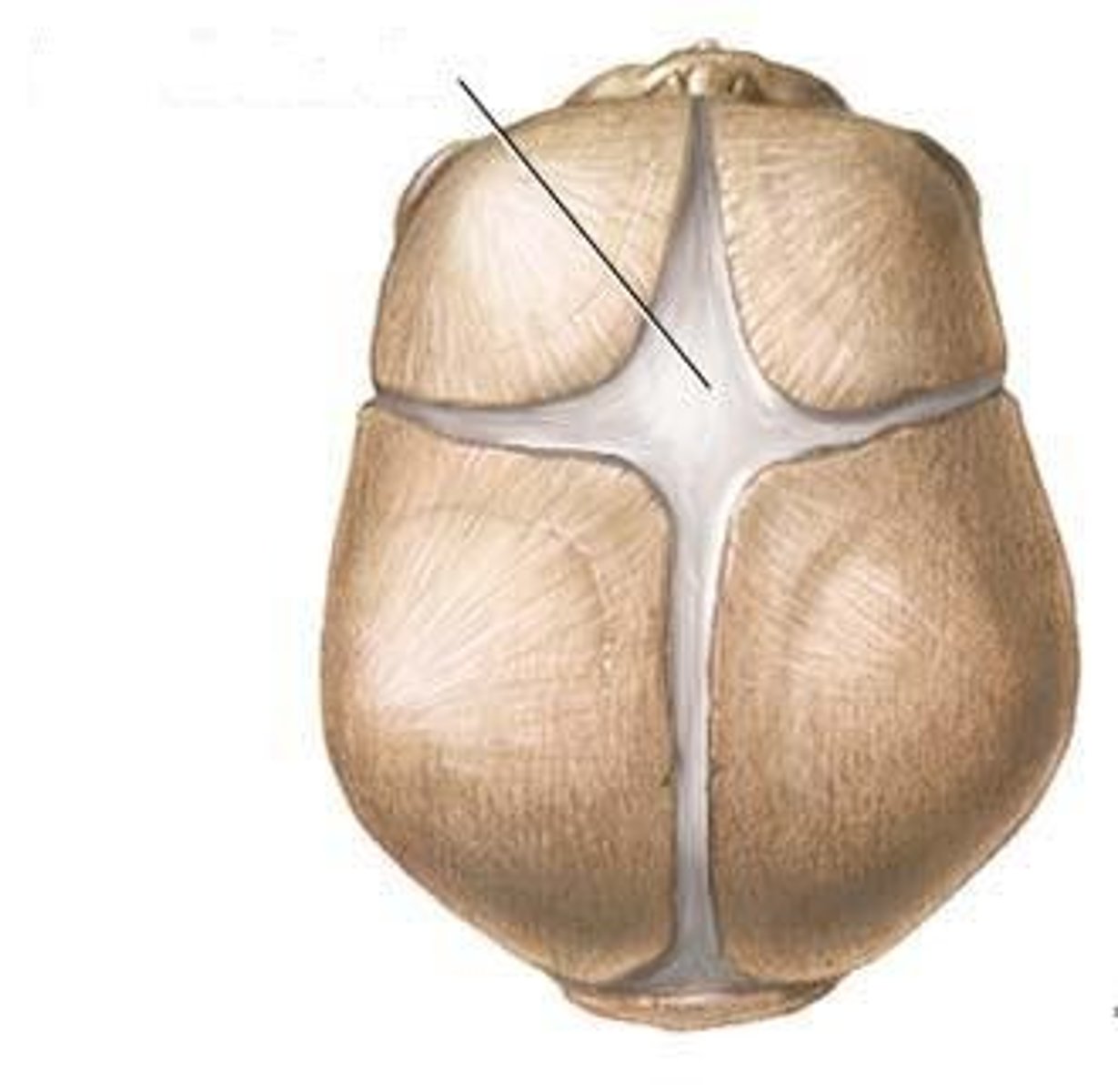
anterior vs posterior fontanelle
Anterior- variable size, usually closes by 9-18m
Posterior usually < 1 cm, usually closes by 2-4m
suture lines and molding/overlapping -- what happens?
Molding or overlapping skull bones from passage through the birth canal, a temporary asymmetry of the head.
If the asymmetry persists >2-3w, may be craniosynostosis --> refer
craniotabes
-soft area of the skull (usu parietal) that feels like a ping-pong ball when depressed.
benign: May be intrauterine position.
If doesn’t resolve, it may be pathologic --> refer
caput succedaneum
area of edema of the scalp which crosses the suture lines, occurs at presenting part of skull.

cephalohematoma
Subperiosteal bleeding which forms a fluctuant mass that does not crosses the midline. Takes weeks-months to resolve.
what might cause facial palsies in NB
from forceps deliveries or prolonged labor
what might cause facial dysmorphology in the NB
genetic syndromes or Fetal Alcohol
Syndrome, unusual shape of the nose or ears, wide spaced
eyes, long philtrum
why might exam of baby's eyes be hard after birth
edema of eyes
eyes & genetic syndromes or Fetal Alcohol Syndrome
wide spaced eyes

why might baby have asymmetry of eyes
due to prominent epicanthal folds (Down's), size of globes or ptosis.

palpebral fissures in baby eyes
when slanted indicate a genetic syndrome. Up (Downs) or Down (Treacher's Collins)
eye movement test in baby -- what is important to note
eye movement can be tested by holding infant upright and moving them from side to side. Asymmetrical eye movement is common in first month of life
sclera of NB
normally white/clear
conjunctiva in baby
examine for inflammation or drainage. Hemorrhage may occur spontaneously during birth or from a traumatic delivery.
pupils and baby -- what is abnormal
shape and constriction reflex to light,
Leukocoria, a white pupil may be retinoblastoma

red reflex in baby -- what is abnormal and what does that indicate
elicited with an ophthalmoscope light from 18" away, in darkened room. A diminished or white reflex can be congenital cataracts
position of baby ears
Low set if top of ear is lower than an imaginary line drawn posteriorly from the outer canthus of the eye. Posterior position. Genetic syndromes
malformed ears associated w...
dysplasia, associated hearing loss
preauricular pits and tags are associated w...
when found in isolation (no facial dysmorphology or ear dysplasia) are unlikely to be associated with hearing loss
ear canal in NB
examined for patency. Small size and occlusion with vernix prohibits an otoscopic ear exam
nose shape in baby
- what might thin/wide nose suggest
appearance may be flattened or asymmetrical from intrauterine positioning.
A very thin nose or extra wide nose may be consistent with a genetic syndrome.
nares in baby
- what might cause obstruction
patency is very important as neonates are primarily nose breathers.
Obstruction may be from suctioning at birth or Choanal atresia (tested by attempting to pass a feeding tube through the nose.
a recessed jaw (micrognathia)
part of Pierre Robin Syndrome which also includes glossoptosis (falling backwards of the tongue) and a Cleft palate.

complications of recessed jaw
There can be feeding and breathing issues.
treatment of severe recessed jaw
surgery
epstein pearls
benign inclusion cysts in the midline between the hard and soft palate
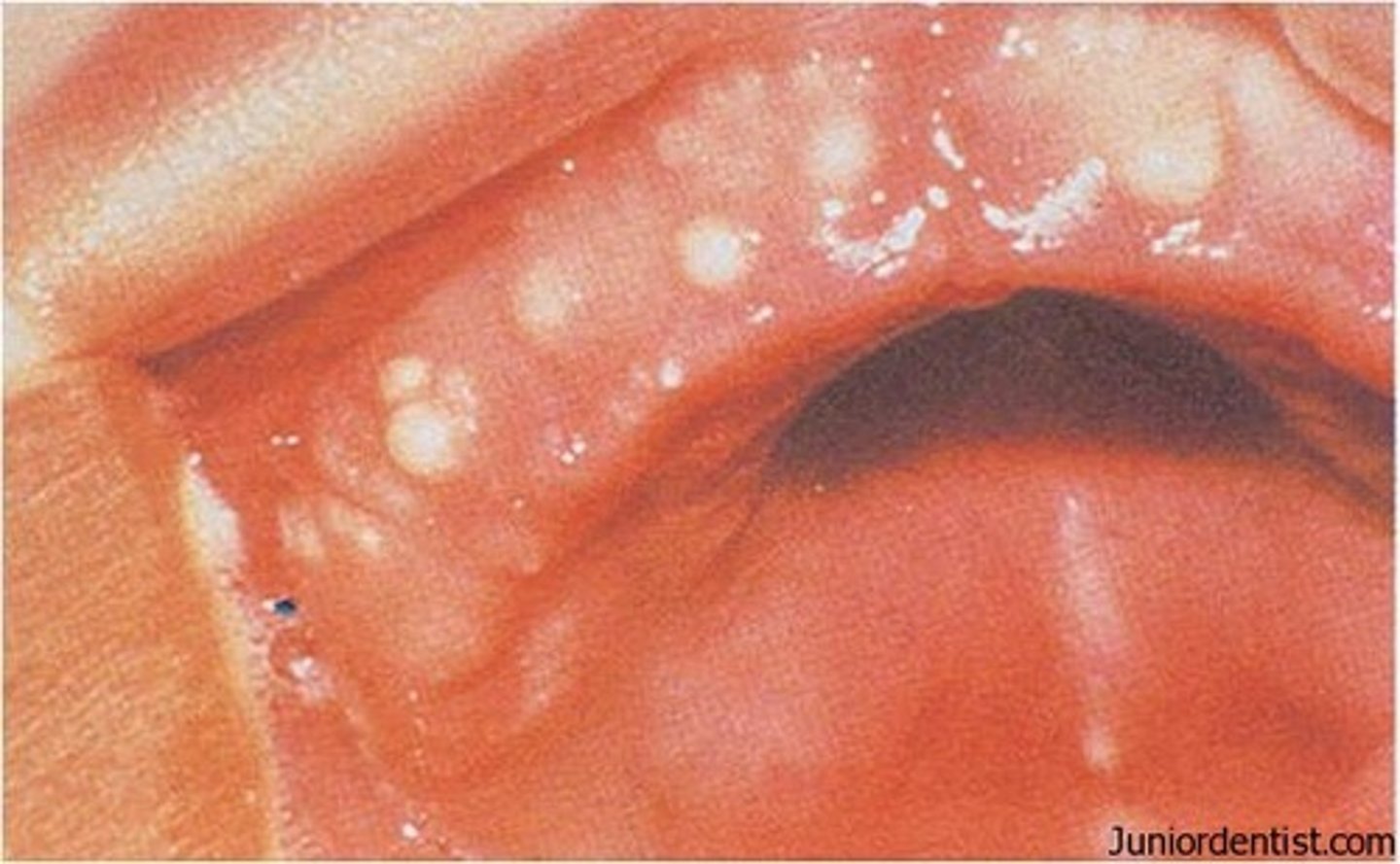
mucous retention cysts
benign cysts on gums, inside of lips or floor of the mouth
frenulum lingae / complication of this
unusually short band of tissue from the floor of the mouth to the tongue.
May extend to the time of the tongue and interfere with latching during breastfeeding
natal teeth
- how to manage?
- what is this associated w/?
Primary mandibular incisors often just a single tooth.
Consider extraction, if not well secured and may result in aspiration. Can be associated with Genetic syndromes.

cleft of hard or soft palate
Require surgical correction. A bifid uvula may be associated with a submucosal cleft palate

cystic hygromas
microcystic malformation of the lymphatic system, usually a painless, transilluminated cyst located about the clavicles

brachial cleft cyst
located anterior margin of SCM

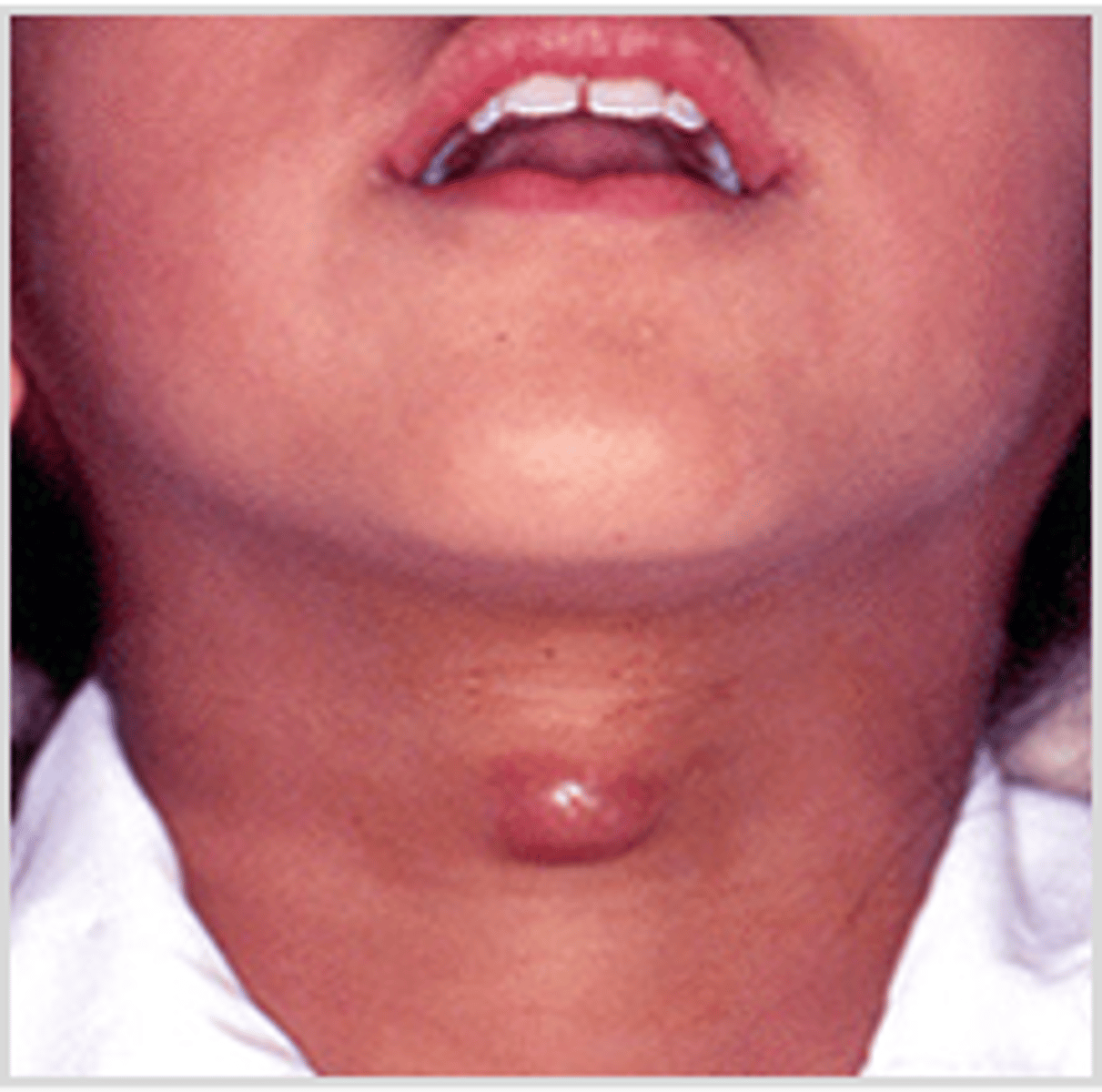
thyroglossal duct cyst/enlarged thyroid
midline
cervical lymph nodes
may be normal or be from congenital infections
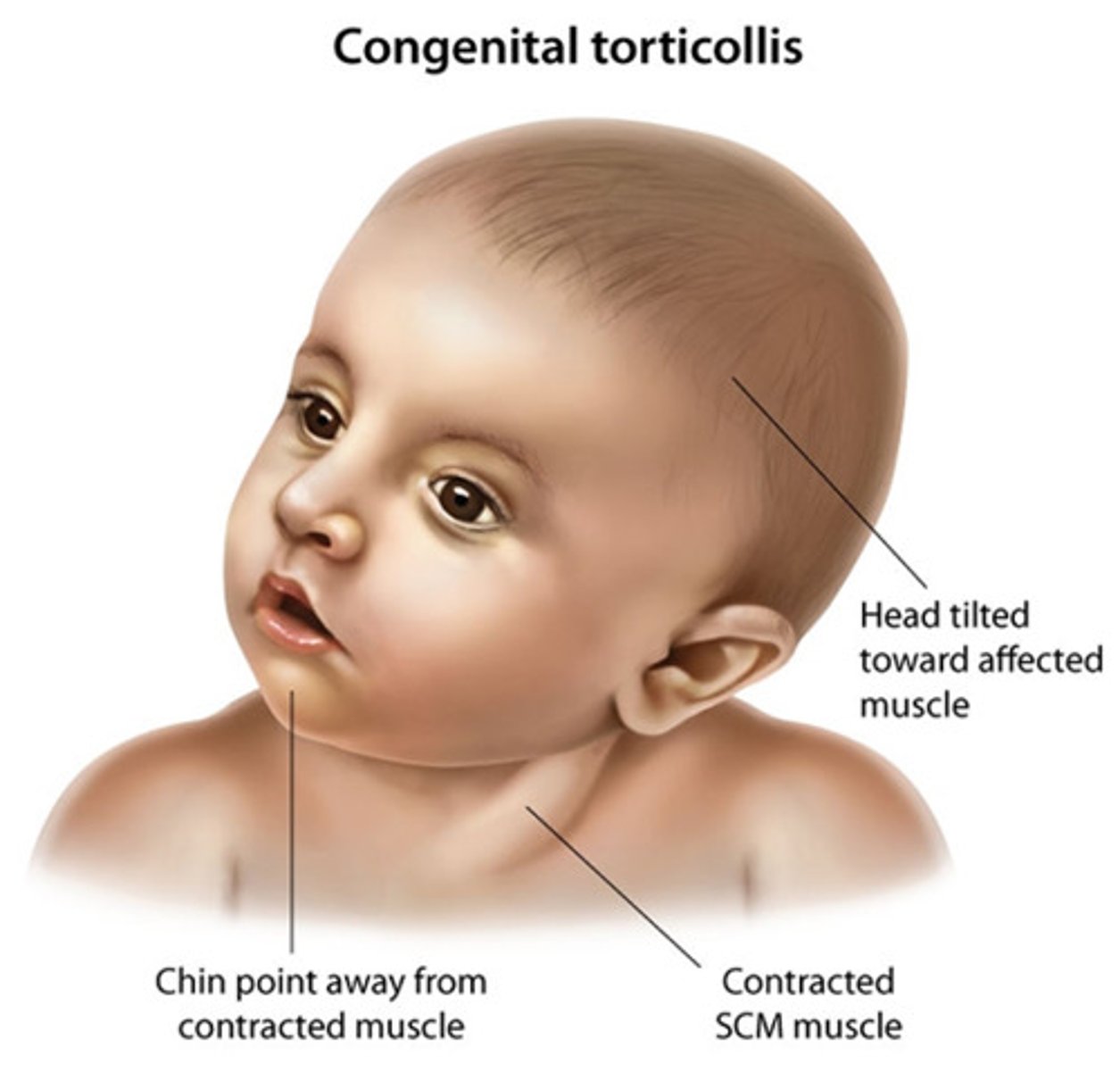
torticollis
head tipped to one side, chin points to the other side.
Usually caused by injury to SCM during delivery or from intrauterine positioning/
excess skin in NB
webbing in Turners syndrome and redundant folds in Downs
clavicle fx in NB / presentation
caused from birth trauma. Presents with irritability and decreased mobility of arm
Exam shows tenderness, swelling and crepitus of the clavicle and asymmetrical Moro reflex.

small chest / malformed thorax indicates...
pulmonary hypoplasia or a neuromuscular disorder
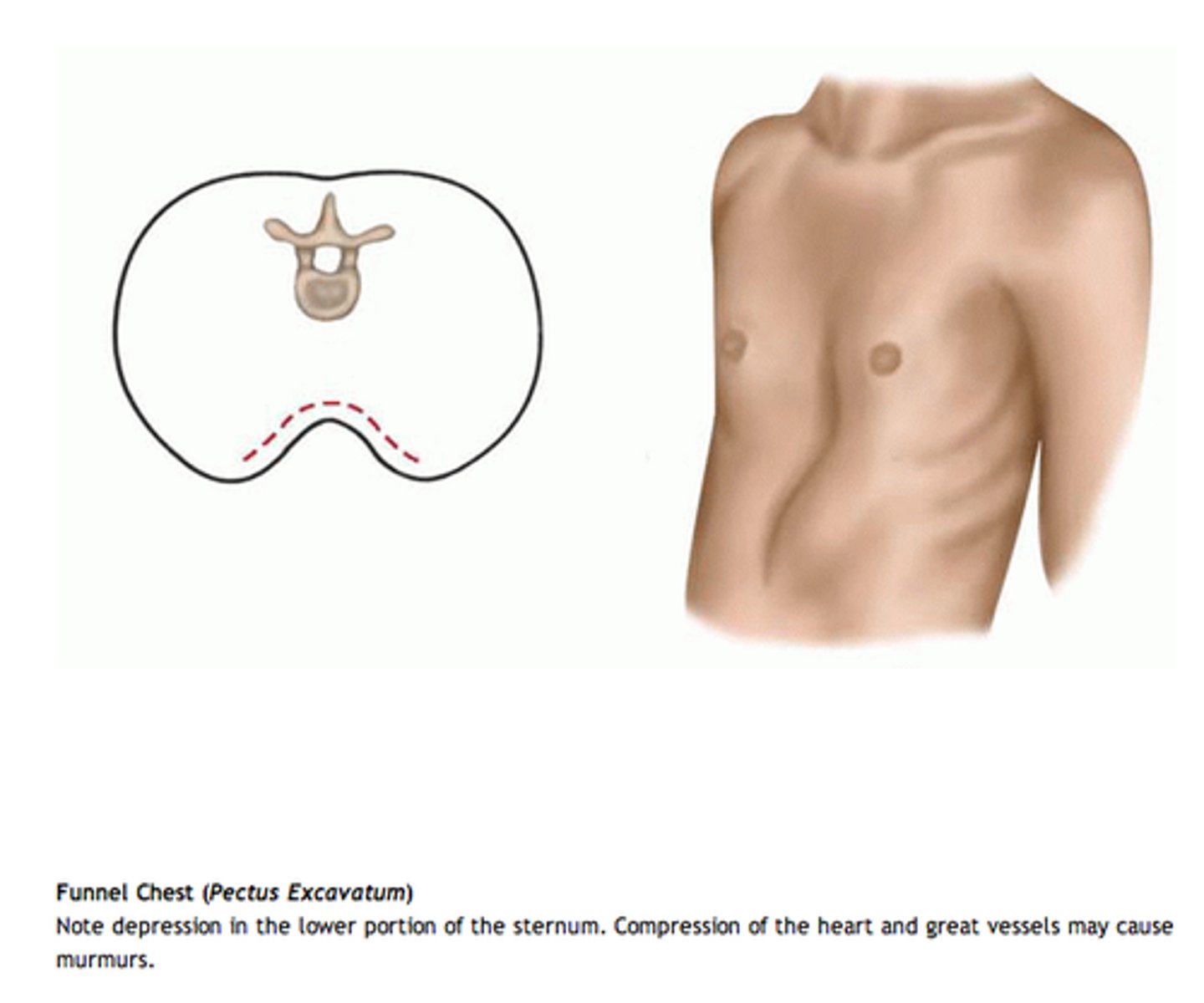
pectus excavatum (funnel chest)
Depression of the sternum
pectus carinatum

chest wall movement with breathing
On inspiration rib cage moves inward while abdomen moves outward
breasts in NB baby
In both males and females, breast may be hypertrophied and asymmetrical, due to maternal hormones,
wide nipples in baby indicates what
possible turners
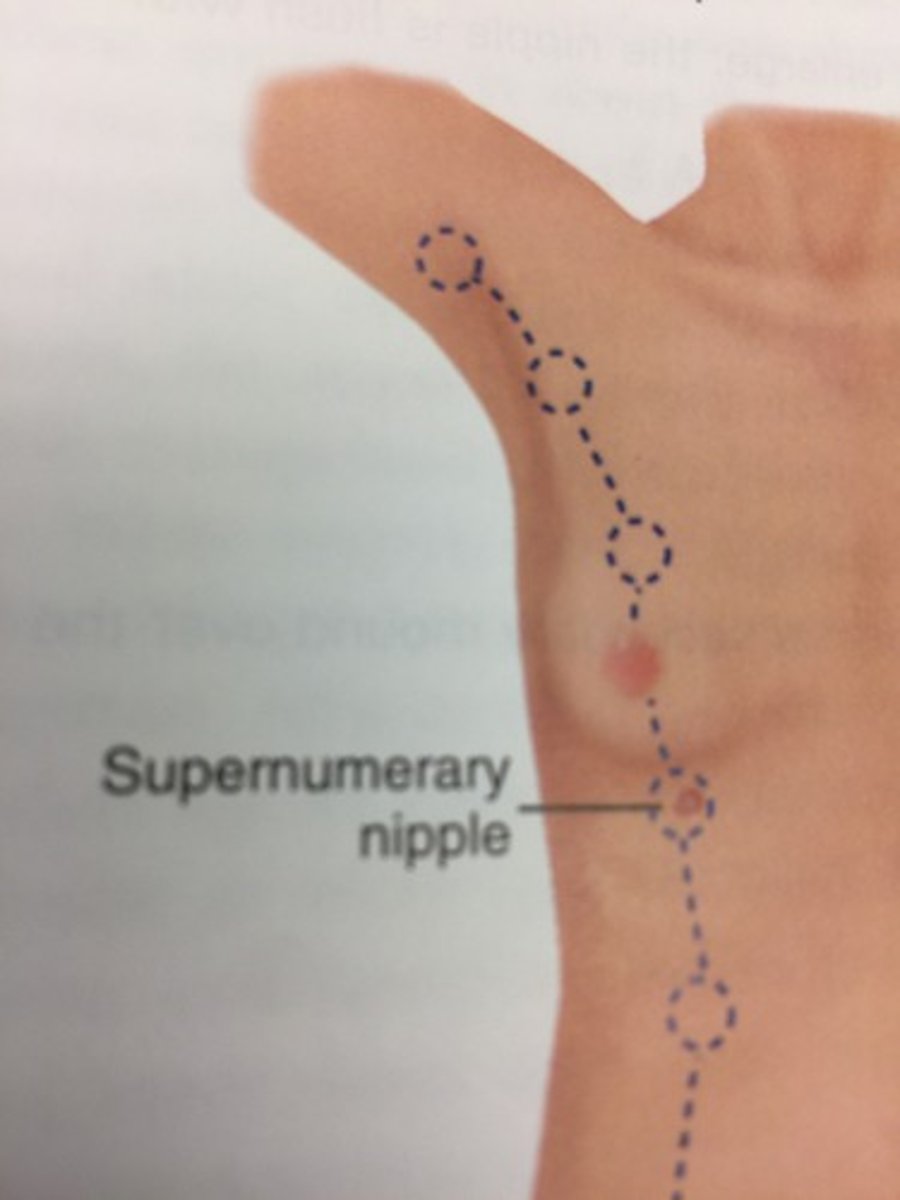
supernumerary nipples, where are they normal
along milk line
respiratory distress in baby
nasal flaring, grunting, tachypnea and accessory muscle use, stridor
normal breath sounds in baby
equal on both sides. Rales can be normal for a few hours after birth
normal RR baby
40-60 w/ variations in rate/rhythm
PMI of baby
PMI is felt best a left lower sternal border. RV is dominant.
pulses in baby -- which are best
femoral pulses are the most easily detected when the infant is quiet.