Lesson 118 - Butts, paws and others
1/90
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
91 Terms
What is systemic lupoid onychodystrophy (SLO)?
changes to the claws which occur secondary to inflammation of the claw bed and causes abnormal claw growth
What is the etiology of systemic lupoid onychodystrophy (SLO)?
poorly understood but likely includes immune-mediated and hereditary components
What is the signalment commonly affected by systemic lupoid onychodystrophy (SLO)?
1. large breed dogs like Rottweiler, Labrador, GSD, Boxer, Greyhound, Collies among others
2. Young to middle aged (2-6 years)
What is the clinical presentation of systemic lupoid onychodystrophy (SLO)?
might start with only one claw affected and progress to multiple claws on multiple paws within weeks to months and is often mistaken for claw trauma
What is onychomadesis?
sloughing of the claws
What is onychorrhexis?
splitting of the claws
What is onycholysis?
claw separation from the claw bed
What is trachyonychia?
roughened texture of the claws
How is systemic lupoid onychodystrophy (SLO) diagnosed?
1. Biopsy is required for definitive diagnosis
2. involves amputation of the third phalanx as well as the claw matrix
3. If required dew claw recommended to avoid weight bearing digits
What is seen on histopathology of systemic lupoid onychodystrophy (SLO)?
interface inflammation at the junction of the claw bed epithelium and the dermis, with or without a lichenoid band
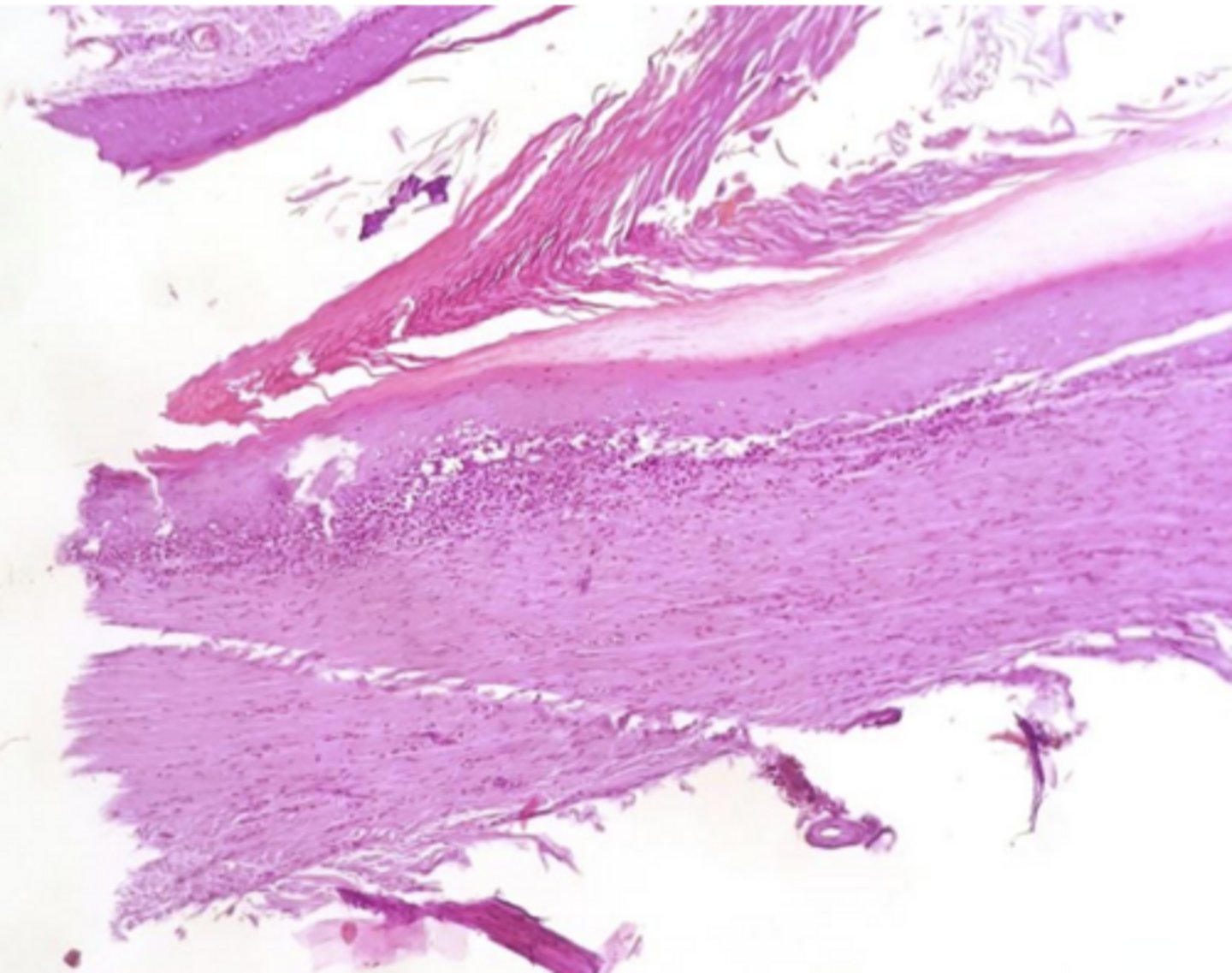
What is this?
histopathology of systemic lupoid onychodystrophy (SLO)
What is the treatment for systemic lupoid onychodystrophy (SLO)?
1. Pain control with gabapentin and corticosteroids for severe painful cases
2. Pentoxifylline, Cyclosporine, oral essential fatty acids for long-term control
When do bacterial infections of the claw occur most commonly?
secondary to some underlying local or systemic disease
What is the most common cause of bacterial infections of the claw?
trauma from fracture, excessively short nail clipping, etc.
What can occur in chronically infected claws?
osteomyelitis
What is the treatment for chronically infected claws with osteomyelitis?
P3 amputation
How are bacterial claw infections diagnosed?
What is the treatment for mild bacterial claw infections?
topical therapy
What is the treatment for severe bacterial claw infections?
treat as deep pyoderma
What is the most common fungal infection of the claw?
malassezia
What are the clinical signs of a malassezia infection of the claw?
some degree of paronychia and brown waxy debris at the claw fold (permanently red-brown)
What is a rare systemic fungal claw disease?
dermatophytosis
What are the clinical signs of claw dermatophytosis?
onychomalacia (commonly asymmetric) and commonly other clinical signs of generalized dermatophytosis
How is claw dermatophytosis diagnosed?
fungal culture of claw material
What is commonly cultured with claw dermatophytosis?
trichophyton mentagrophytes
What is the treatment for claw dermatophytosis?
same as for generalized dermatophytosis
What are the subungual (claw bed) tumors?
1. melanoma
2. squamous cell carcinoma
3. keratoacanthoma
Which subungual (claw bed) tumors are malignant?
1. melanoma
2. squamous cell carcinoma
Which subungual (claw bed) tumor is benign?
keratoacanthoma
What are the clinical signs of subungual melanoma?
swelling, pain, lameness, and brittle or missing claws
How do subungual melanomas behave?
1. locally invasive, often destroying bone
2. 30-58% chance of metastasis by the time of diagnosis
What is the treatment for subungual melanomas?
amputation of the affected digit at the metacarpophalangeal or metatarsophalangeal joint, and tributary lymph node
What is the prognosis for subungual melanomas?
median survival of about one year with surgical treament
What is a subungual squamous cell carcinoma?
tumor of the claw bed epithelium
What is the most common signalment for subungual squamous cell carcinoma?
dogs 7-11 years
How do subungual squamous cell carcinomas behave?
1. Slow growing
2. Can aggressively spread to the lymph nodes and beyond
3. ~1/3 of tumors in this site will metastasize even after amputation of the digit
What is the curative treatment for subungual squamous cell carcinoma?
amputation
What is a keratoacanthoma?
rare benign tumor that typically emerges as a single, enlarged, and twisted claw
What is the common signalment for keratoacanthoma?
adult dogs of any age (3-14 yrs)
How can keratoacanthomas cause loss of P3?
tumor-induced lysis and pressure necrosis of the claw bed
What is the curative treatment for keratoacanthomas?
amputation
What do hyperkeratotic disorders usually affect?
nose and footpad
What can cause hyperkeratotic disorders?
1. Age related change
2. Secondary to certain conditions like autoimmune diseases, distemper virus, zinc-responsive dermatosis
How are hyperkeratotic disorders diagnosed?
1. clinical appearance
2. biopsy and histopathology
What is the treatment for hyperkeratotic disorders?
none, management only
How are hyperkeratotic disorders managed?
1. Regular gentle trimming of the buildup, reshaping footpads to avoid gait changes
2. Emollients: petroleum jelly, nose/paw balms
3. Keratolytics: urea, salicylic acid, lactic acid
4. Antiseptic soaks: avoid fissuring and secondary infections
Where are anal sacs located?
in the subcutaneous tissue between the external and internal anal sphincter muscle
What is the structure of anal sacs?
invaginations of the skin lined with apocrine and sebaceous glands produce a secretion rich in bacteria and sebaceous material
What are the characteristics of the ducts of the anal sacs?
small, narrow duct that opens into the anal canal, usually near the junction of the skin and the anal mucosa
What is the function of the anal sacs?
sphincter muscles compress the sacs as feces passes, releasing the fluid onto the stool for territory marking and identification
What is anal saccultis?
inflammation and/or infection of one or both anal sacs that can lead to failure of emptying and ultimately rupture
What is the etiology of anal saccultis?
1. Allergy is the most common comorbidity
2. Causality not confirmed but suspected to be related to dysbiosis
What is the common signalment of anal saccultis?
1. Breed (spaniels and brachycephalics), stool quality, diet type, and changes, osteoarthritis
2. Any age
What are the clinical signs of anal saccultis?
1. Scooting, licking/chewing the perianal region
2. Blood in the stool, and/or leaking anal sacs
What are the different clinical presentations of anal sac disease?
1. Anal sac impaction
2. Anal sacculitis
3. Anal sac abscess
What is anal sac impaction?
anal sac overfilling
What is anal sac abscess?
rupture of the anal sac, leading to cellulitis and deep infection of surrounding tissue
How is anal saccultis diagnosed?
1. Clinical presentation
2. Thorough rectal exam to empty sacs and reveal thickened tissue
What is the treatment for anal saccultis?
1. Address any identifiable underlying issues
2. Localized treatment of anal sacculitis with flushing and infusion
3. Anal sacculectomy as a salvage procedure for refractory cases or when masses are present
What underlying issues can cause anal saccultis?
allergy, obesity, fiber content of diet, GI issues, osteoarthritis pain
What is the local treatment protocol for anal sacculitits?
1. Digital expression of anal sac(s)
2. Carefully insert lubricated IV catheter (no needle), tom cat catheter or curved tip syringe into anal sac duct
3. Flush the sac with saline until all material is removed
4. Infusion of polyvalent ointment like Animax® or Mometamax® (off-label use)
5. May need to be repeated at 2-4 week intervals
6. Sedation usually required and recommended
What is the etiology of perianal fistulas (PAF)?
immune mediated disease likely a consequence of local T-cell-mediated inflammation
What is the common signalment of perianal fistulas (PAF)?
80% are middle-aged german shepherds but can occur in any breed
What are the clinical signs of perianal fistulas (PAF)?
1. Single or multiple painful sinus tracts or ulcers that spontaneously occur in the skin around the anus that do not communicate with the rectum
2. Licking around the anus
3. Tenesmus, hematochezia, or mucopurulent discharge
How are perianal fistulas (PAF) diagnosed?
clinical signs (usually with sedation because of pain)
What is the treatment for perianal fistulas (PAF)?
1. Systemic antimicrobials are not helpful in disease but might be needed for secondary infection
2. Topical not practical in painful or severe cases until partial resolution with systemic therapy
3. Prednisone 1-2 mg/kg day
4. Cyclosporine 5 mg/kg q24h
5. Tacrolimus 0.1%- SID- tapering
6. Steroid - mometasone 0.1% SID- tapering
7. Adjunct gabapentin (pain), stool softeners, photobiomodulation, and hydrolyzed or novel protein diet
What are the ischemic dermatopathies?
1. Post-rabies vaccine panniculitis
2. Generalized vaccine-associated ischaemic dermatopathy
3. Canine familial dermatomyositis (FDM)
4. Generalized idiopathic ischaemic dermatopathy
5. Juvenile-onset dermatomyositis-like disease in atypical breeds
What is the etiology of post-rabies vaccine panniculitis?
unknown, but thought to be a type III hypersensitivity reaction
When can post-rabies vaccine panniculitis occur?
1. Typically occurs 2 to 4 months post injection
2. Can have repeated reactions at site of re-vaccination or progress to generalized vaccine-associated ischaemic dermatopathy
What is the common signalment of post-rabies vaccine panniculitis?
toy poodle, shih tzu and bichon frise may be predisposed, but can happen in any breed
What are the clinical signs of post-rabies vaccine panniculitis?
localized and well-demarcated alopecia, hyper- or hypopigmentation, scaling, crusts and ulcers.
How is post-rabies vaccine panniculitis diagnosed?
clinical presentation +/- histopathology
What is the treatment for post-rabies vaccine panniculitis?
1. Not always required since disease is not typically found until late in the course, but can be tried to limit cosmetic effects
2. Pentoxifylline, corticosteroids(oral or topical), vitamin E, cyclosporine (typically reserved for severe/generalized cases)
3. Spontaneous hair regrowth possible, surgical excision is an option when cosmetically important
What needs to be discussed with owners about post-rabies vaccine panniculitis?
risk of recurrence of local disease and progressing to generalized disease with future vaccination

What is this?
symmetric lupoid onychodystrophy (SLO)

What is this?
malassezia claw infection

What is this?
dermatophytosis claw infection

What is this?
footpad hyperkeratosis

What is this?
anal sacculitis

What is this?
perianal fistula

What is this?
post-rabies vaccine induced panniculitis
A 4-year-old Labrador Retriever presents with a 2-month history of progressive lameness. Initially, one claw was fractured and assumed traumatic. Over time, multiple claws on multiple paws have become brittle, sloughing, and misshapen. On exam, several claws show splitting and separation from the claw bed.
What is the most appropriate next step to definitively confirm the diagnosis?
biopsy including P3 and claw matrix
A dog is diagnosed presumptively with SLO based on history and clinical findings. The owner wants a long-term treatment plan.
Which of the following is the most appropriate long-term therapy?
cyclosporine or pentoxifylline ± fatty acids
A dog presents with a single painful, swollen claw after a recent nail trim. There is purulent discharge at the claw fold. Radiographs reveal lysis of the distal phalanx.
What is the best treatment?
amputation of P3
A dog with chronic paw licking presents with brown, waxy debris at the claw folds and red-brown discoloration of claws.
What is the most appropriate first-line therapy?
topical therapy with medicated wipes
A cat presents with asymmetric claw deformities and generalized dermatologic lesions. Onychomalacia is noted.
Which diagnostic test is most appropriate?
fungal culture of claw material
A dog presents with swelling of a digit, lameness, and a missing claw. Radiographs show bone destruction.
What is the most appropriate treatment plan?
digit amputation with lymph node evaluation
A dog presents with a ruptured, draining tract near the anus with surrounding cellulitis.
What is the most likely diagnosis?
anal sac abscess
A middle-aged German Shepherd presents with severe pain, tenesmus, and draining tracts around the anus that do not communicate with the rectum.
What is the most likely underlying pathogenesis?
immune-mediated T-cell inflammation
A dog presents with localized alopecia and hyperpigmentation at a previous rabies vaccine site 3 months after injection.
What is the most likely mechanism?
type III hypersensitivity reaction
How are bacterial claw infections diagnosed?
cytology (+/- culture and susceptibility) with a sample from under the claw