composites, polymerization, bonding
1/77
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
78 Terms
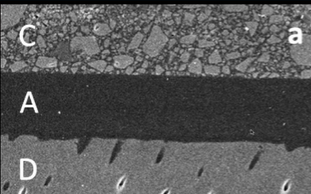
layer D
dentin
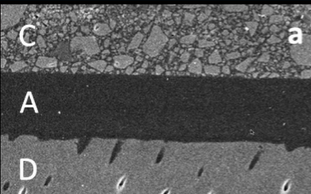
layer A
bonding agent
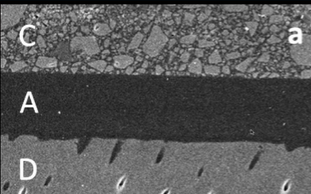
layer C
enamel
what is a composite
a material made up from two or more constituent materials w different physical or chemical properties than the ingredients
what is a dental composite generally made up of
essentially a complex combination of glass or ceramic filler in a resin polymer matrix
dental composite are increasingly popular materials for what type of restorations
direct restoration
what materials can you find in fillers
glass
non-glass base- like zirconia
what is the matrix primarily composed of
resin
is the filler or resin matrix more important
resin matrix
what is the family of the main dental monomers that are used in dental composites
di-methacrylate
what is the coupling agent that couples the glass to the resin (filler to the matrix)
silane coupling agent
what are the major components of composite
matrix- polymer
fillers- glass, ceramics
coupling agent- organo-metallic compound
what are the minor components of composite
initiator
accelerator
diluent
surfactants
pigments
radio opaquer
how did older composites look radiographically
radiolucent → why there are radiopaquers that are put into composites
what is responsible for the radiopacity of the composite
fillers
what properties make a composite desirable
good esthetics
handling properties
physical properties
what esthetic properties make a composite desirable
shade matching
durable gloss
resistant to discoloration
what handling properties make a composite desirable
adequate working time
easy to manipulate
good polymerization performance
quick and easy polishing
what physical properties make a composite desirable
matching mechanical properties of dental tissue
durable under occlusal loads
wear resistant, minimal abrasive wear effect on opposing teeth
minimal shrinkage during and after light curing
dental composites are designed to have what relationship w water
designed to dislike water → hydroPHOBIC
cons to hydrophobicity of composite
less bonding to water-based tissues
cellular toxicity
pros to hydrophobicity of composite
lower water sorption
less water-driven expansion
less staining
less biofilm adhesion
is dentin or enamel more hydrophilic
dentin
what is the process of polymerization
the process of chemically linking many small monomers together to form a large polymer
degree of conversion
percentage of monomers that are incorporated into the polymer → WANT TO BE HIGH
residual monomer
unconverted monomers → we DO NOT LIKE
a ____ (low/high) degree of conversion and _____ (high/low) residual monomer is undesirable
a low degree of conversion and high residual monomer is undesirable
what type of polymerization rxn happens
free radical polymerization
what is the C-C double bond that will undergo polymerization from monomer to polymer
vinyl bond → will be broken and turn into polymer w some sort of radical, usually oxygen based
what does methyl methacrylate become after free radical vinyl polymerization
poly methyl methacrylate- PMMA
what is the bulky monomer that is the basis of most dental composites
BIS-GMA
size of these from smallest to largest:
BIS-GMA
HEMA
TEGMA
HEMA < TEGDMA < BISGMA
what is the single methacrylate called
HEMA
what are the di-methacrylates called
BIS-GMA
UDMA
TEGMA
bulky monomers increase the viscosity or flowability
inc viscosity
less bulky monomers increase the viscosity of flowability
flowability
what is the linking in dental composites between di-methacrylate monomers
cross-linked
what is addition polymerization→ curing
when di-methacrylate monomers’ double bonds open up to allow the monomer to bond to neighboring monomers which results in the formation of cross-linked polymer network
what effect does the cross-linking network have on the composite
improves wear, lowers solubility, increases modulus, and increases strength
what is happening during polymerization shrinkage
C=C (vinyl) conversion results in smaller intermolecular distances, which in turn results in smaller composite volume
on average, composites shrink ___% linearly or __% by volume
0.5-1.5% linearly or 3% by volume
what can polymerization shrinkage lead to
debonding, leakage, caries, stress, hypersensitivity, fx, staining
what is the phase that does NOT react as part of the polymerization rxn
fillers → it is usually glass of ceramic in dental composites
how do fillers improve the physical properties of polymerized composites
improve translucency, radiopacity, strength, wear resistance
reduce volumetric shrinkage
what is the range of filler sizes used today
40 nm to 50 microns
how are composites names after
filler size:
macrofill
microfill
nano-fill
microhybrid fill
what are the two ways the degree of fill is measured
volume %
weight %
does volume % or weight % matter more to us, why
volume % → volume of the filler, the lower amount of shrinkage
what kind of strategies are used by manufactures to create a higher volume %
pre-polymerized particles
surfactants
surface treatments
what happens if you have too much filler in a composite
results in unworkable viscous composite (high filler → high viscosity)
why are coupling agents important
critical to wear resistance, stain resistance, reduce crack propagation, surface integrity, and prevent particle dislodgment
what is dental curing
addition polymerization by free-radical initiation, an accelerator that facilitates free-radical formation
what are the three types of curing, put an asterisk by the one that is most common today
heat cure
chemical cure
light cure*
when is heat cure typically used
denture
indirect restorations
NOT IN PTS MOUTH
what are the main 2 types of LCU
QTH light
LED light
range of power density for QTH light
older: 400-600
newer: 800-1000
pros to QTH light
broad spectrum
high intensity- newer one
cons to QTH light
lots of heat- even w filtering
noisy
fan
cord
longer curing time required
power density for LED light
1200
pros for LED light
high output
little heat
battery driven
no cord
cons for LED light
the head or guide design may affect performance
LED spectra may be too narrow for certain composites
what should you take into consideration for a light curing unit
power density
spectral output
heat generation
homogeneity of output
intensity w distance
tip design
eye protection
why is power density a consideration factor for a light curing unit
must be sufficient to penetrate into the composite and cure the composite in a clinically reasonable time
why is spectral output a consideration factor for a light curing unit
must match the absorption of the photo-activator
why is heat generation a consideration factor for a light curing unit
show be low, or risk pulpal damage; should be <1 C rise for <1 min
why is homogeneity of output a consideration factor for a light curing unit
should be even across a cross-section of the output
why is intensity w distance a consideration factor for a light curing unit
degree of decay w distance
why is tip design a consideration factor for a light curing unit
should be convenient use
why is eye protection a consideration factor for a light curing unit
it is not UV but do NOT stare
what is etch made up of
phosphoric acid, 35% gel
etch is thixotropic, what does this mean
stays where you put it
why is it important to get a rough surface prior to bonding and placing composite
good micro-mechanical possibilities for bonding
anything you want to bond to, do you want to have a high or low surface energy
high
what is the purpose of etching
to increase surface energy → will rough surface, don’t want to do too much tho!
what is the main challenge to bond to dentin
dentin is wet, collagen mineral while composites are hydrophobic, the bonding agent will need to link the two
why is dentin etching not the same as enamel
it may be etched too deep, be too wet, or be too dry