Portal Hypertension
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
portal hypertension is
the elevation of blood pressure within the portal venous system
the common cause of portal hypertension
cirrhosis
portal hypertension can also result from
portal vein thrombosis, hepatic vein thrombosis, IVC thrombosis, or compression of the portal veins by a tumor in an adjacent organ
what results in portal hypertension
the pressure within the portal veins increasing
because the liver becomes so scarred with cirrhosis,
the blood flowing to the liver meets greater vascular resistance, resulting in portal hypertension or high blood pressure within the portal veins
portosystemic collaterals and varicosities can consequently
develop within the abdomen as a result of the body’s attempt to repair itself by channeling blood away from the damaged liver
examples of portosystemic collaterals that may result from portal hypertension
coronary vein
short gastric vein
gastrorenal pathway
splenorenal pathway
umbilical vein
anterior abdominal wall vein
superior mesenteric vein
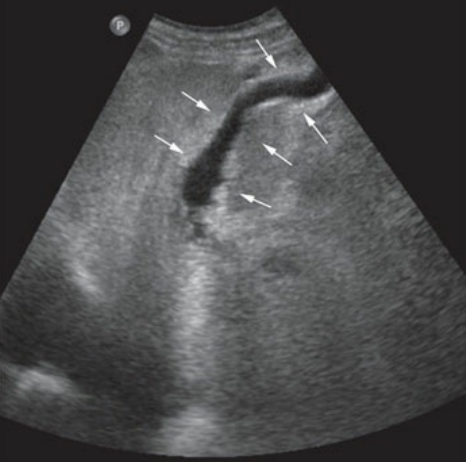
a patent or recanalized paraumbilical vein is noted extended from the left lobe of this patient who is suffering from cirrhosis and portal hypertension
one of the most common sonographically identifiable collaterals in portal hypertension is
the recanalization of the paraumbilical vein, also termed a patent paraumbilical vein
the umbilical vein is associated with
the left portal vein, ligamentum teres, and falciform ligament
cruveilhier-baumgarten syndrome
when the umbilical vein becomes open again and shunts blood away from the liver and into the inferior epigastric veins or superior epigastric vein
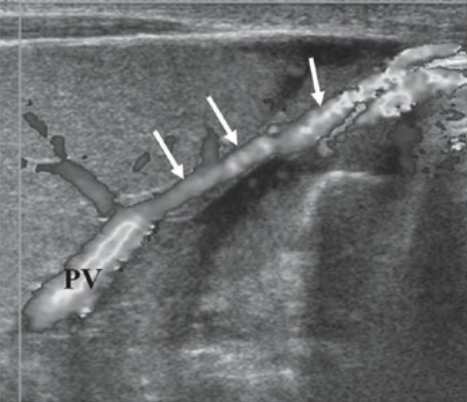
recanalized paraumbilical vein is demonstrated extended from left portal vein toward the anterior abdominal wall in a patient with portal hypertension
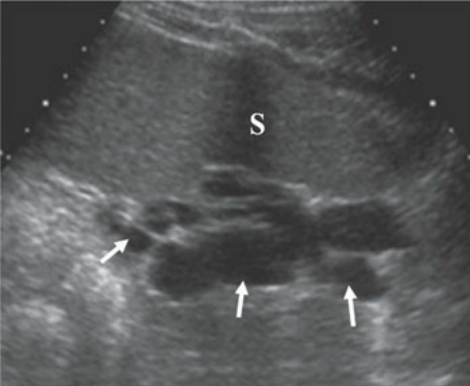
in a patient with portal hypertension, splenic varices are noted adjacent to the spleen in area of the splenic hilum
abdominal varicosities may be noted
by the splenic hilum, renal hilum, and gastroesophageal junction
enlargement and — may be seen with portal hypertension
reversed flow within the coronary vein, also referred to as the left gastric vein
normal coronary vein can be seen arising
from the splenic vein and extending superiorly toward the left
with portal hypertension, the coronary vein will demonstrate
abnormal flow toward the esophagus and will measure greater than 6 mm
shunting of blood toward the esophagus increases the risk for
esophageal hemorrhage and death
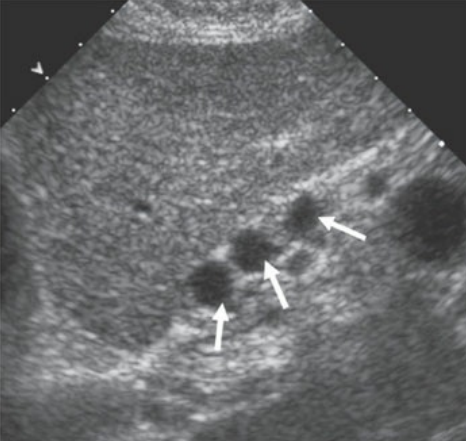
enlarged coronary vein can be seen posterior to the left lobe in a patient with portal hypertension
with portal hypertension, along with hepatofugal flow, the portal vein diameter — and —
will exceed 13mm in the AP dimension and the superior mesenteric vein will exceed 10mm
hematemesis, if present, is an ominous sign of
ruptured esophageal varices because it is markedly increases mortality and morbidity
caput medusa
recognizable dilation of the superficial veins of the abdomen
surgically placed shunts include
portocaval shunt, splenorenal shunt, and mesocaval shunt
a common, minimally invasive interventional treatment for portal hypertension
transjugular intrahepatic portosystemic shunt (TIPS)
TIPS
placement of a stent between the portal veins and hepatic veins to shunt blood and reduce portal systemic pressure
if you suspect cirrhosis, be sure to closely analyze the — for evidence of recanalization of the paraumbilical vein
left portal vein
the recanalized paraumbilical vein will extend from
the left portal vein, continues through the left lobe, and may travel inferiorly toward the umbilicus
clinical findings of portal hypertension
abnormal liver function tests
ascites
diarhhea
fatigue
hepatomegaly (initially)
hepatic encephalopathy
caput medusa
tremors
gastrointestinal bleeding
sonographic findings of portal hypertension
hepatomegaly (initially)
shrunken right lobe of the liver
enlarged caudate lobe of the liver
nodular surface irregularity
coarse echotexture
splenomegaly
ascites
monophasic flow within the hepatic veins
hepatofugal flow within the portal veins
enlargement of the portal vein (diameter will exceed 13 mm in the AP)
enlargement of the SMV'
enlargement and reversed flow within the coronary vein
enlarged hepatic arteries
abdominal varicosities at the splenic hilum, renal hilum, and gastroesophageal junction