Looks like no one added any tags here yet for you.
Acute Coronary Syndrome (ACS)
Classified by causative event → total of 5 diff types
Most common ~90% →
Arterial occlusion primarily driven by _____________ → MI
VTE driven by ________
Post MI pathophysiology → activates ____ and ______
^ can create ________ leading to HF
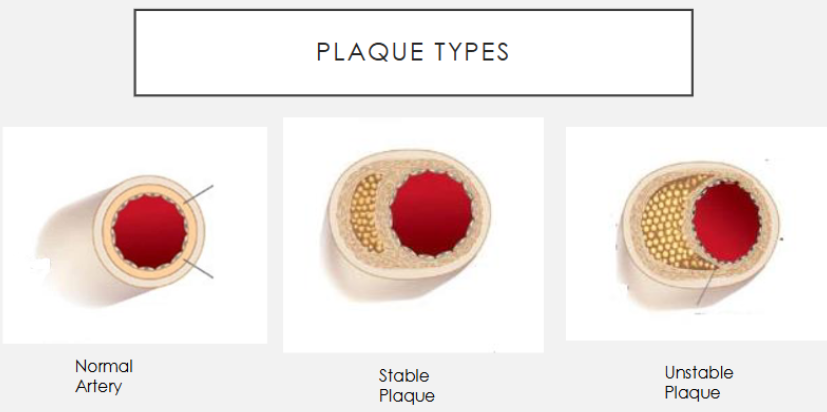
type 1 → acute plaque rupture
platelet aggregation
clotting cascade
+SNS, RAAS
ventricular hypertrophy
COMPLICATIONS FROM MI
construction issues → 3
cardiac function → 3
structural issues → 3
bradycardia, heart block, vent arrhythmia
cardiogenic shock, HF, TE (thromboembolism)
papillary muscle rupture, free wall rupture, pericarditis
Patient presentation MI (diff from angina)
________ chest pain
Squeezing, heaviness, or tightness of chest lasting ______
Pain may radiate to …
-
-
-
ATYPICAL PRESENTATION IN … (5)
crushing
>10 min
arms, shoulder, back, abdomen, jaw
NV
diaphoresis (sweating)
SOB
>75, women, diabetes, impaired renal, dementia
SIGNS
ADHF with _______ distention
___________
_____ on auscultation
New ________ or mitral regurgitation
New _________
Hemodynamic abnormalities ranging from …
jugular venous
pulm edema
S3
murmur
arrhythmias
HTN to hypotension w/shock
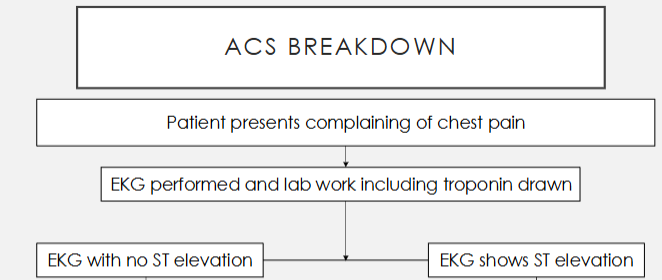
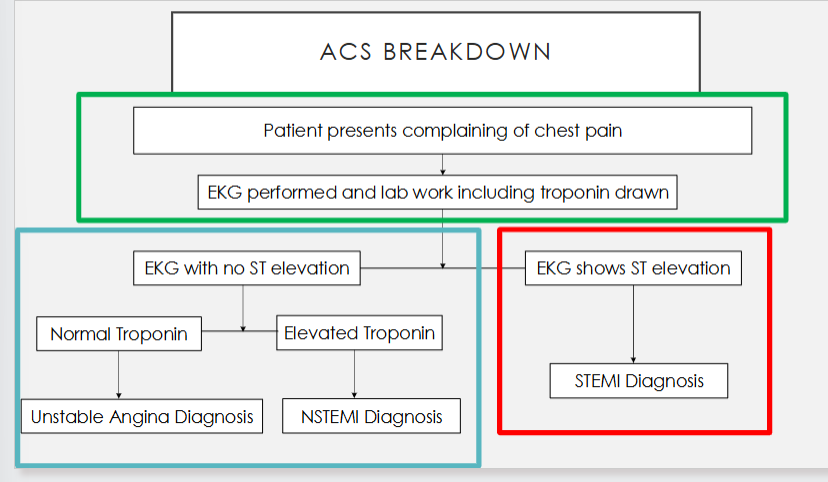
ACS WORK UP (in order)
________ + goal time
-
-
-
-
-
EKG <10 min
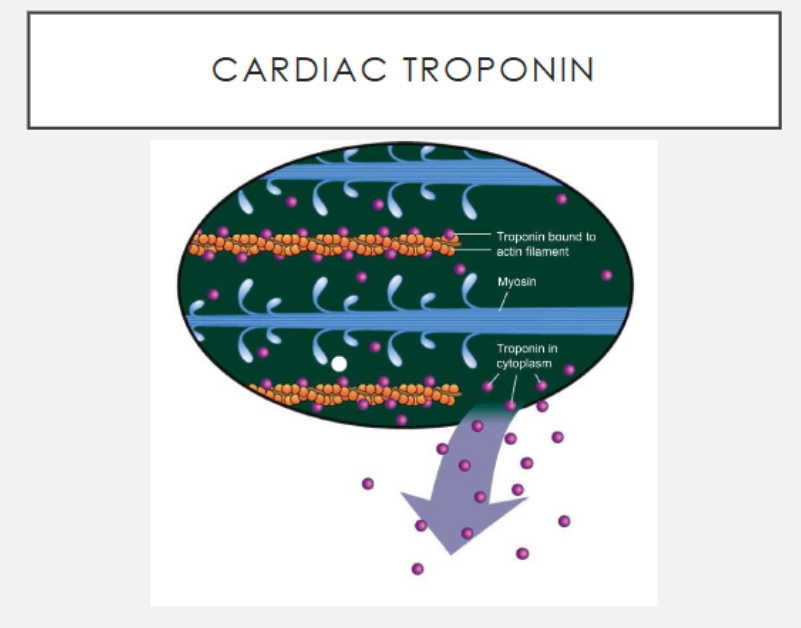
cardiac troponin (cytoplasm troponin is BAD)
chem panel K, Mg, SCr
CBC
coagulation tests → aPTT, anti Xa
lipid panel
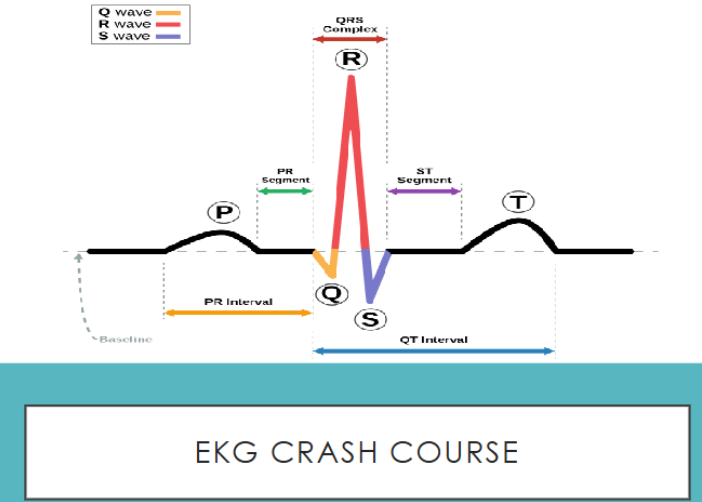
P =
QRS =
T =
____ tells us whether the patient is having an MI
atria
vent contracting
vent resetting
ST
ST elevation →
no ST elevation →
STEMI
normal troponin → unstable angina; +troponin → NSTEMI
GREEN BOX → placed on every patient
*MONA-B =
Morphine (analgesia/anxiolytic) → place in therapy → CI?
^ alternative?
O2 indicated in patients with O2 saturation _____
NTG → initially given … → CI?
Aspirin → place in therapy → initial dose → when to use?
Beta blocker → when to use?
^ alternative? (CI to BB)
morphine, O2, NTG, ASA, BB
2nd line pain after NTG → CI hypersens, hypotens, brady/lethargy
fentanyl
<90%
SL then IV if anginal symptoms persist → CI SBP<90 or >30 below baseline, PDE5i
all → 162-324 mg CHEWED → IMMEDIATELY
for all → use any EXCEPT ISA → within 24h
CCB
Do NOT use beta blockers in patients with ACS due to ___________ use → potential of unopposed alpha stimulation & coronary vasospasm
cocaine → use CCB
WHAT TESTS OR LABWORK WOULD BE THE MOST APPROPRIATE TO OBTAIN ON OUR PATIENTS?
A. CBC, BMP, Coagulation tests
B. EKG, Troponin, BMP
C. Troponin, BMP, CBC
D. EKG, Coagulation tests, CBC
B
What is a situation that a beta blocker would be CI in but a CCB would not?
A. Hypotension
B. Acute decompensated heart failure
C. Cocaine use
D. Third degree heart block
C
What would be the most appropriate treatment to initiate in FC?
A. Morphine, Oxygen, Metoprolol
B. Metoprolol, Diltiazem, Nitro
C. Aspirin, Morphine, Carvedilol
D. Aspirin, Oxygen, Nitro
D
(always give ASA immediately, O2 89% so give, can give some more nitro too)
Would you give him?
M
O
N
A
B
no (NTG not given yet + substance use disorder)
no (97%)
yes
yes
no → CCB
NSTEMI: Used in LOWER risk patients that do not require urgent PCI → ___________ approach
Risk assessment by _______ or _______ score
selective invasive
TIMI, GRACE
NSTEMI: Used in INTERMEDIATE - HIGH risk patients → ____________ approach
Also beneficial for (6)
routine invasive
70+, prev MI, ST changes, HF, +troponin, diabetes
What treatment path is best for Alex?
A. selective invasive
B. routine invasive
C. STEMI
B
(age 70, +troponin, symptoms → routine invasive)
What treatment path is best for Antonio?
A. selective invasive
B. routine invasive
C. STEMI
A
NSTEMI TREATMENT
Initial treatment during workup (both)→
Additional tx aimed at keeping vasculature patent (both) → 2
final step: Selective invasive →
final step: Routine invasive →
ASA, O2 if <90%, BB in first 24h, NTG/morphine
antiplatelets (P2Y12), anticoagulants (heparin)
continued workup
angiography
P2Y12 INHIBITORS:
antiplatelet through ____ pathway
*4 agents, can NOT use them interchangeably for all ACS tx regimens!!!
Irreversible binding →
Reversible binding →
Prodrugs →
Clopidogrel (______) → metab by multiple CYPs but mainly 50% _____ → may be used in … → Platelets require ____ to recover after stopping → monitor …
Prasugrel (______) → metab by .. → _________ platelet inhibitor compared to clopidogrel → CI? → Platelets require ____ to recover after stopping → monitor …
Ticagrelor (_______) → metab by … → CI? → monitor …
Cangrelor (_______) → the only inhibitor admin ____
ADP
clopidogrel, prasugrel
ticagrelor, cangrelor
clopidogrel, prasugrel
Plavix → CYP2C19 → ALL → ~5d → s/s bleeding
Effient → 1 CYP → more potent → CI hx stroke/TIA → ~7d → s/s bleeding
Brilinta → CYP3A4 → CI in ASA>100 mg/day → s/s bleeding, dyspnea
Kengreal → IV
P2Y12 Overview
Planned PCI → use …
NO planned PCI → use …
ticagrelor or prasugrel, clopidogrel
ticagrelor, clopidogrel
ANTICOAGULATION:
Tx is __________ and NOT continued after discharge
Unfractionated Heparin UFH → Large interpatient variability require monitoring every _______ (aPTT, AXA) → place in therapy? → monitoring?
Enoxaparin (Lovenox, LMWH) → smaller fragments which create a more _____ effect than UFH, anticoagulation monitoring NOT required → place in therapy? → CI?
Agent can be used in HIT + lower risk patients? → risk?
Agent can be used in HIT + PCI ONLY (not fibrinolysis)? + monitoring
short term
6h → ALL → s/s bleeding, HIT
predictive → ALL → CI hx HIT
fondaparinux/Arixtra → catheter thrombosis
Bivalirudin/Angiomax → s/s bleeding, ACT (activated clotting time)
What medications should be AVOIDED in Alex due to his history?
A. NTG infusion
B. Aspirin
C. Bivalirudin infusion
D. Prasugrel
D
What presenting factor immediately decides Saul’s treatment arm?
A. Initial troponin of 1.0 ng/ml
B. His current cocaine use and chest pain
C. His EKG reading
D. The severity of his chest pain symptoms
C (ST elevation → treat on STEMI pathway)
STEMI TREATMENT: (+ST)
All STEMI patients should have _________ rapidly pursed → _________
PCI compared to fibrinolysis (3)
2 types of PCI →
CABG (harvested vein) may be necessary in patients w ___________
reperfusion therapy → PCI, fibrinolytic
+survival, -risk stroke/IC hemorrhage, -reinfarction/ischemia
DES (drug eluting stent), BMS (bare metal stent)
severe/multivessel CAD
FIBRINOLYSIS
Primarily favored in patients with DELAY to cath lab ________
fibrinolytic initiated than patient transferred to PCI capable hospital
ABSOLUTE CONTRAINDICATIONS → 2
3 agents →
>120 min
hx stroke, severe HTN
alteplase, reteplase, tenecteplase
STEMI TREATMENT step wise
Initial during workup
Revascularization
additional concurrent tx
POST STENTING →
MONAB
PCI, fibrinolysis
antiplatelets, anticoagulants
DAPT for 12 months → shorten for +risk bleeding
UNDER WHICH SITUATION SHOULD SAUL RECEIVE FIBRINOLYTICS?
A. He is two and a half hours from a cath lab
B. The doctor anticipates he will need a CABG
C. If he is being taken immediately to the cath lab
D. He experiences cardiac arrest
A
HIGH BLEED RISK MANAGEMENT:
Patients stable on _________ and ______ from event can stop ASA
Patients can de-escalate from higher bleed risk P2Y12s (prasugrel and ticagrelor) to _______
Patients w GI bleeding as concern can be safely initiated on ______
Patients who require therapeutic anticoagulation with their DAPT (apixaban, etc) should ___________________
ticagrelor >1 month → stop ASA
clopidogrel
GI bleed → start omeprazole
DC ASA 1-4 weeks post event
Important STEMI METRICS
Door to EKG!!!
<10 min
When to pick ticagrelor over clopidogrel?
ACS or MI
ACS DISCHARGE → THROMBINS2
When are each used?
Thienopyridine (clopidogrel, prasugrel)
Heparin
RAAS
Oxygen
Morphine
Beta blocker
Intervention (PCI)
NTG
Statin
Salicylate
during + discharge
during
started during admiss/discharge
during if O2 sat <90%
2nd line pain
during first 24h + prn discharge
during
during + prn discharge
start at discharge
during + discharge
SECONDARY PREVENTION: CHOLESTEROL MANAGEMENT
Patient not on statin or on low/moderate → initiate ________
Consider _______ add on
Reassess lipid profile in ______
Patient on max tolerated statin →
→
→
high-intensity statin
ezetimibe
4-8 weeks
LDL<55 continue+reassess
LDL 55-69 consider add nonstatin+reassess
LDL>70 add nonstatin+reassess
ACS SECONDARY PREVENTION
all patients without CI →
all patients without CI →
DAPT
Beta blockers → all without CI →
ACEi → all without CI →
MRA →
SL NTG prn (CI PDE5i)
daily baby ASA (75-162mg) → watch for ticagrelor (<100mg daily)
PDY12 for 12 months
use HF BBs (metoprolol succ, bisoprolol, carvedilol) for CHF
ARNI if CHF or intolerant to ACEi cough
all w HFrEF + diabetes/CHF
SH IS BEING DISCHARGED. WHEN REVIEWING HIS MEDICATION LIST, WHICH MEDICATION HAS A CONTRAINDICATION PRESENT?
PTA Med List:
Aspirin 81mg daily
Citalopram 10mg daily
Pantoprazole 20mg daily
Tadalafil 5mg daily
Metformin 500mg twice daily
Medications added at discharge:
Lisinopril 10mg daily
Metoprolol succinate 50mg daily
Ticagrelor 90mg BID
Nitro 0.4mg prn
A. Aspirin
B. Ticagrelor
C. Nitro
D. Lisinopril
C
(CI w tadalafil)
What medication class to use for stenting?
GIIb/IIIa
What medications to add/adjustments for ACS discharge?
+atorvastatin (to high intensity)
BB
-ASA to 81 mg daily
(no NTG bc he is on tadalafil)
What changes should be made based on his current therapy regimen? What other medication issues should be investigated at this appointment?
DC ASA for 1-4 weeks (since he is on ticagrelor + apixaban)