Equine Repro ICVA Diseases
1/132
Earn XP
Description and Tags
Break this card into multiple cards titled Pathophysiology, Clinical signs, Diagnostics, Treatment,Prevention
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
133 Terms
Pathophysiology of Abortion in Horses
in mares is defined as the loss of pregnancy before the fetus is viable (before 300 days of gestation). This involves complex interactions between the fetus, placenta, and uterus; disruptions due to infection, placental insufficiency, or systemic illness can lead to abortion.
Clinical Signs of Abortion in Horses
Common clinical signs include premonitory signs such as
vaginal discharge
or colic-like symptoms,
sudden abortion with the expulsion of the fetus, and
examination of expelled fetal membranes may reveal abnormalities.
Diagnostics for Abortion in Horses
clinical examination,
ultrasonography for fetal viability and placental thickness,
laboratory tests for serum progesterone and pathogen detection, and
vaginal cytology and culture to identify infectious agents.
Treatment for Abortion in Horses
± antibiotics for placentitis,
anti-inflammatory agents,
progesterone supplementation, and
supportive care in a stress-free environment.
Prevention of Abortion in Horses
vaccination against EHV-1 and EVA to reduce the risk of infectious abortions etc
Pathophysiology of Agalactia in Horses
is the absence or significant reduction of milk production in a lactating mare. Disruptions in the hypothalamic-pituitary-ovarian axis can impair prolactin secretion due to factors like
stress,
poor nutrition,
systemic illness, and
certain pharmacological agents.
Inadequate mammary development (mammary hypoplasia) may occur from hormonal imbalances, impacting future milk production.
Clinical Signs of Agalactia in Horses
Common clinical signs include:
Reduced or absent milk production
Poor udder development, sometimes evident during late pregnancy
Foal distress: frequent nursing attempts, vocalization, restlessness; risk of failure of passive transfer (FPT)
Signs of underlying causes:
Mastitis: fever, depression, anorexia
Fescue toxicosis: prolonged gestation, dystocia, retained placenta, thickened placental membranes.
Diagnostics for Agalactia in Horses
Diagnostics may include:
Clinical examination for udder size, milk quality, and signs of mastitis
Blood tests to measure serum prolactin and progesterone levels
Evaluation of mammary secretions through cytology and culture for infection
Dietary assessment including history of fescue exposure
Ultrasonography to evaluate mammary gland abnormalities or abscesses.
Treatment of Agalactia in Horses
Treatment aims to address underlying causes:
Nutritional support: high-quality forage and balanced concentrates.
For Endophyte-Infected Fescue Toxicosis: Remove mare from fescue pasture or hay, provide non-fescue forage, and administer dopamine antagonists (domperidone 1.1 mg/kg orally once daily) to block dopamine-mediated suppression of prolactin.
For Mastitis: systemic antibiotics, anti-inflammatories, udder drainage.
Hormonal therapy: dopamine antagonists effective in endocrine-related agalactia.
Foal management: colostrum supplementation, plasma transfusion, milk replacers, or fostering with a nurse mare if lactation is inadequate.
Prevention of Agalactia in Horses
Prevention strategies include:
Assessing the mare’s diet for fescue exposure
Early intervention with dopamine antagonists to restore milk production
Adequate nutritional and stress management
Comprehensive diagnostics to rule out infection or systemic illness.
Pathophysiology of Cervical Disorders in Horses
These conditions can compromise the cervix’s ability to maintain an appropriate environment for conception, gestation, and parturition:
Cervical Tears: Resulting from difficult foalings or manual interventions, leading to damage and increased risk of infertility.
Cervical Adhesions: Form through inflammation or trauma, obstructing the cervical canal and interfering with reproductive processes.
Cervical Cysts: Glandular cysts that may alter cervical function, potentially causing fertility issues.
Congenital Abnormalities: Rare anomalies like cervical hypoplasia affecting reproductive functions, often resulting in early infertility.
Clinical Signs of Cervical Disorders in Horses
Common clinical signs include:
Infertility: Decreased fertility or failure to conceive despite repeated breeding.
Abnormal Estrous Cycles: Prolonged estrus or signs of endometritis.
Dystocia History: Previous incidents indicating potential cervical trauma.
Visible or Palpable Lesions: Abnormalities observed during reproductive examinations, such as tears or cysts.
Diagnostics for Cervical Disorders in Horses
Diagnostics include:
Clinical History: Thorough reproductive history, including previous foalings and fertility issues.
Speculum Examination: Visual inspection for tears and structural abnormalities.
Palpation: Assessment of cervical tone and structure via rectal palpation.
Ultrasound: Detection of internal abnormalities not visible through speculum examination.
Hysteroscopy: Direct visualization for suspected adhesions or internal abnormalities.
Treatment for Cervical Disorders in Horses
Treatment options vary depending on the condition:
Cervical Tears:
Mild Tears: Often heal without intervention; conservative management may be sufficient.
Severe Tears: Require surgical repair and post-operative care.
Cervical Adhesions:
Surgical Dissection: Removal of adhesions using hysteroscopic techniques.
Post-Surgical Management: Use of anti-adhesion agents to reduce recurrence risk.
Cervical Cysts:
Drainage and Removal: Glandular cysts can be drained and treated to prevent recurrence.
Congenital Abnormalities:
Breeding Management: AI techniques or corrective surgery for anatomical defects.
Prevention of Cervical Disorders in Horses
Preventative strategies include:
Breeding Management: Careful handling to minimize trauma during breeding.
Monitoring: Regular reproductive evaluations, especially in mares with a history of dystocia.
Biosecurity Measures: Implementing measures to reduce the risk of uterine infections.
Pathophysiology of Dystocia in Horses
in horses arises from complications during parturition, commonly due to abnormal fetal positioning, maternal pelvic abnormalities, or uterine inertia. The primary causes of dystocia include fetal malposition, fetal oversize, maternal pelvic abnormalities, and uterine inertia.
Clinical Signs of Dystocia
Clinical signs typically identified during stage two of labor include prolonged labor (exceeding 30 minutes), excessive straining without progression, observation of abnormal fetal parts protruding from the vulva, and signs of restlessness such as anxiety and sweating.
Diagnostics for Dystocia in Horses
Diagnosis includes a physical examination to assess the mare's condition, vaginal examination to evaluate fetal presentation and position, ultrasound for additional information on fetal viability, and radiography in rare cases to assess fetal size and position.
Treatment for Dystocia in Horses
Treatment involves correction of malposition, controlled vaginal delivery (CVD), potential fetotomy for cases of fetal death, emergency cesarean section if needed, and post-delivery care including antibiotics and assessments for both mare and foal.
Prevention of Dystocia in Horses
Prevention strategies include proper breeding management by selecting compatible mare and stallion sizes, monitoring mare health, ensuring proper nutrition during pregnancy, and regular veterinary check-ups to identify potential complications.
Cryptorchidism in Stallions: Pathophysiology
commonly referred to as 'retained testicle' or 'rig,' is a congenital condition characterized by the failure of one or both testes to descend into the scrotum. The condition can be unilateral (one testis retained) or bilateral (both testes retained), and may result from genetic factors, hormonal imbalances, or anatomical defects during fetal development.
Cryptorchidism in Stallions: Clinical Signs
Cryptorchid stallions often exhibit reduced fertility and may present with behavioral issues typically associated with intact males, such as aggression and heightened libido. Physical examination may reveal the absence of one or both testes in the scrotum.
Cryptorchidism in Stallions: Diagnostics
Diagnosis involves a thorough physical examination, ultrasonography, and hormonal assays. The Anti-Müllerian Hormone (AMH) test is particularly useful as elevated levels indicate the presence of testicular tissue. Laparoscopy can also be employed for definitive diagnosis.
Cryptorchidism in Stallions: Treatment
The treatment of choice is surgical removal of the retained testicle(s) via cryptorchidectomy. This procedure can be performed through various approaches, and early surgical intervention is recommended to prevent complications.
Cryptorchidism in Stallions: Prevention
Preventative strategies include genetic counseling to identify at-risk animals and minimizing factors that may contribute to the condition during fetal development.
Testicular Hypoplasia: Pathophysiology
refers to the underdevelopment of one or both testes, resulting in smaller-than-normal testicles with impaired spermatogenesis. This condition can arise from chromosomal abnormalities, hormonal deficiencies, or environmental factors.
Testicular Hypoplasia: Clinical Signs
Common clinical signs include unilaterally or bilaterally small, firm testicles, reduced or absent sperm production (azoospermia), decreased libido, and in advanced cases, asymmetrical testicles.
Testicular Hypoplasia: Diagnostics
Diagnostics include physical examination, ultrasonography, hormonal assays (LH, FSH, and testosterone), and testicular biopsy to confirm histological abnormalities.
Testicular Hypoplasia: Treatment
No curative treatment is available; management focuses on optimizing fertility where possible, such as through artificial insemination with limited viable sperm.
Testicular Hypoplasia: Prevention
Genetic counseling may be recommended to prevent the transmission of the condition.
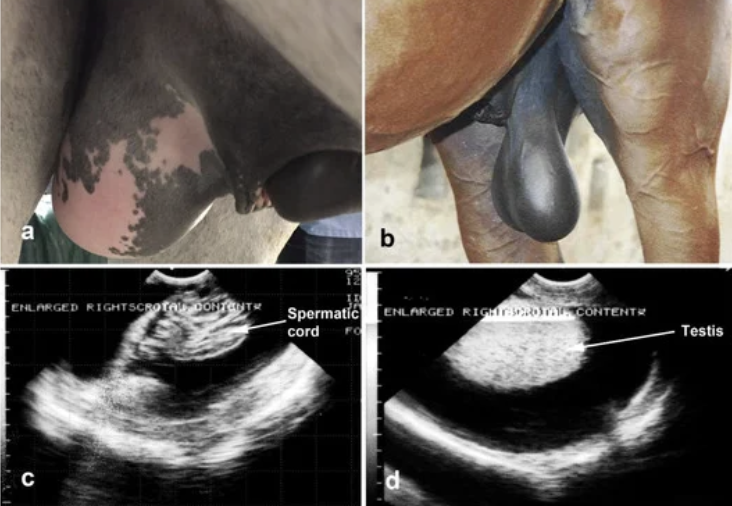
Hydrocele: Pathophysiology
is the accumulation of serous fluid between the parietal and visceral layers of the vaginal tunic surrounding the testicle. It may result from trauma, inflammation, or idiopathic causes.
Hydrocele: Clinical Signs
Clinical signs include a fluctuant, non-painful swelling of the scrotum, no significant change in testicular consistency, and possible discomfort interfering with breeding in severe cases.
Hydrocele: Diagnostics
Diagnostics involve physical examination, ultrasonography, and possibly aspiration for fluid analysis.
Hydrocele: Treatment
Conservative management for mild cases; surgical drainage or castration may be necessary for severe or persistent cases.
Hydrocele: Prevention
Preventative strategies involve addressing underlying causes such as trauma or infection.

Testicular Torsion: Pathophysiology
refers to the twisting of the spermatic cord, compromising blood flow to the testicle, leading to ischemia and potential necrosis.
Testicular Torsion: Clinical Signs
Acute onset of severe testicular pain, swollen and painful testicle, asymmetry in testicular position, and possible signs of colic.
Testicular Torsion: Diagnostics
Physical examination revealing abnormal testicular positioning, ultrasonography to assess blood flow, and scintigraphy to confirm ischemia.
Testicular Torsion: Treatment
Surgical detorsion and fixation if performed early; castration recommended if ischemic damage is severe.
Testicular Torsion: Prevention
Preventive measures include careful handling to avoid trauma and monitoring of stallions with long spermatic cords.
Hematocele: Pathophysiology
occurs when blood accumulates between the layers of the vaginal tunic surrounding the testicle, usually following trauma.
Hematocele: Clinical Signs
Acute, painful swelling of the scrotum, possible discoloration, testicular pain, and reluctance to move.
Hematocele: Diagnostics
Physical examination for swelling and discoloration, ultrasonography to identify echogenic fluid, and aspiration to confirm diagnosis.
Hematocele: Treatment
Immediate supportive care; surgical intervention may be necessary for severe cases.
Hematocele: Prevention
Preventive strategies involve managing risk factors such as trauma and monitoring for signs of underlying coagulopathies.

Paraphimosis: Pathophysiology
occurs when the penis becomes prolapsed and cannot retract into the prepuce, potentially leading to edema and necrosis.
Paraphimosis: Clinical Signs
Prolapsed, swollen penis that cannot retract, possible edema and ulceration, and difficulty urinating or breeding.
Paraphimosis: Diagnostics
Physical examination observing the prolapsed penis and evaluating for underlying trauma or neurological conditions.
Paraphimosis: Treatment
Immediate manual reduction, use of bandaging or suture to keep the penis retracted, and anti-inflammatory medications.
Paraphimosis: Prevention
Preventive measures involve careful handling during breeding and monitoring for signs of trauma.
Priapism: Pathophysiology
is a persistent erection unrelated to sexual arousal, often caused by vascular dysfunction resulting in impaired venous outflow.
Priapism: Clinical Signs
Prolonged, painful erection, swollen and engorged penis, and inability to retract the penis into the prepuce.
Priapism: Diagnostics
Physical examination indicating persistent erection and history of drug administration or trauma.
Priapism: Treatment
Immediate medical management with penile massage, intracavernosal injections of vasoconstrictors, and potential surgical intervention.
Priapism: Prevention
Preventative strategies include careful monitoring of drug use and management of underlying neurological conditions.
Pathophysiology of Infertility in Horses
The pathophysiology of infertility in horses varies depending on the underlying cause and can be broadly categorized into congenital, acquired, and functional types:
Congenital Abnormalities: These include anatomical defects such as incomplete development of reproductive organs (e.g., segmental aplasia of the uterus, intersex conditions).
Infectious Causes: Infections of the reproductive tract, particularly in mares, such as endometritis.
Hormonal Imbalances: Endocrine dysfunctions affecting estrous cycles and reproductive health.
Mechanical and Functional Issues: Conditions affecting sperm transport and embryo development.
Systemic Diseases: Conditions like laminitis or metabolic syndrome that disrupt hormonal balance or overall health.
Clinical Signs of Infertility in Horses
The clinical presentation varies depending on the cause:
Mares:
Irregular estrous cycles or anestrus.
Failure to conceive despite repeated breeding.
Early embryonic loss or abortion.
Abnormal uterine discharge.
Stallions:
Decreased libido or failure to achieve erection.
Reduced sperm output or quality.
Azoospermia or oligospermia (absence or low sperm concentration).
Pain or discomfort during breeding.
Diagnostics for Infertility in Horses
A comprehensive diagnostic approach is essential:
History and Physical Examination: Detailed breeding and reproductive history.
Reproductive Examination in Mares:
Transrectal ultrasonography.
Uterine cytology and culture.
Endometrial biopsy.
Hormonal assays.
Reproductive Examination in Stallions:
Semen analysis.
Testicular ultrasonography.
Hormonal testing.
Breeding soundness exam (BSE).
Treatment for Infertility in Horses
Treatment strategies depend on the identified cause:
Mares:
Intrauterine antibiotic therapy for bacterial endometritis.
Hormonal therapies to regulate the estrous cycle.
Surgical correction of anatomical abnormalities.
Use of advanced reproductive techniques.
Stallions:
Hormonal supplementation for endocrine disorders.
Semen extenders or cryopreservation to enhance fertility potential.
Systemic antibiotics for bacterial infections.
Prevention of Infertility in Horses
Prevention strategies include:
Maintaining optimal health and nutrition for mares and stallions.
Regular veterinary care to monitor reproductive health.
Good breeding management practices to reduce risk factors.
Implementing biosecurity measures to limit exposure to infectious agents.
Pathophysiology of Metritis
is an inflammation of the uterus, commonly following parturition. It can be caused by retained fetal membranes, bacterial infections, and systemic illness. The inflammation can lead to the breakdown of uterine tissue and a decrease in fertility due to disruption in the reproductive environment.
Clinical Signs of Metritis
:
Foul-smelling vaginal discharge
Fever
Depression and lethargy
Anorexia
Decreased milk production
Abdominal distension or discomfort
Diagnostics for Metritis
Diagnosis may involve:
Clinical examination (history and physical assessment)
Ultrasonography to evaluate uterine condition
Vaginal cytology to identify infectious agents
Culture and sensitivity testing of uterine discharge
Diagnostics for Metritis
Diagnosis may involve:
Clinical examination (history and physical assessment)
Ultrasonography to evaluate uterine condition
Vaginal cytology to identify infectious agents
Culture and sensitivity testing of uterine discharge
Prevention of Metritis
Preventative strategies include:
Maintaining good hygiene during parturition
Monitoring for retained fetal membranes and addressing them promptly
Ensuring proper nutrition and management of pregnant mares
Implementing biosecurity measures to prevent infection.
Granulosa-Theca Cell Tumors (GTCTs): Pathophysiology
are the most common ovarian tumors in horses and typically arise from the granulosa and theca cells of the ovary. They are usually unilateral, with the affected ovary becoming enlarged and the contralateral ovary undergoing atrophy due to hormonal feedback mechanisms. These tumors produce varying amounts of hormones, including testosterone, inhibin, and estrogen, leading to reproductive abnormalities.
Granulosa-Theca Cell Tumors (GTCTs): Clinical Signs
Clinical signs include persistent estrus or anestrus behavior, stallion-like behavior due to elevated testosterone levels, infertility or irregular estrous cycles, and an enlarged ovary detectable via rectal palpation and ultrasonography.
Granulosa-Theca Cell Tumors (GTCTs): Diagnostics
Diagnostics involve rectal palpation revealing enlarged and asymmetrical ovaries, ultrasonography showing a honeycomb or multilocular appearance, hormonal assays indicating elevated inhibin and testosterone levels, and histopathological examination for definitive diagnosis.
Granulosa-Theca Cell Tumors (GTCTs): Treatment
The treatment of choice is surgical removal (ovariectomy), which can be performed laparoscopically or via open surgery. This removal often resolves clinical signs and normalizes the reproductive cycle.
Granulosa-Theca Cell Tumors (GTCTs): Prevention
Currently, specific prevention strategies for GTCTs are not well established due to their complex etiology, but monitoring older mares for signs of reproductive issues may be beneficial.
Ovarian Hematomas: Pathophysiology
occur due to hemorrhage into a large, developing follicle or following ovulation, leading to an enlarged ovary that may disrupt normal reproductive cycles.
Ovarian Hematomas: Clinical Signs
Signs include unilateral ovarian enlargement, possible discomfort or colic-like symptoms, and disruption of the estrous cycle.
Ovarian Hematomas: Diagnostics
Diagnostics include rectal palpation showing enlarged ovaries, ultrasonography revealing large, dense, fluid-filled structures, and hormonal assays to assess reproductive hormone levels.
Ovarian Hematomas: Treatment
Treatment may include pain management with NSAIDs and monitoring via ultrasonography, as small hematomas often resolve spontaneously.
Ovarian Hematomas: Prevention
Prevention strategies include proper management of breeding practices to minimize trauma and monitoring for signs of discomfort in mares.
Ovarian Dysgenesis: Pathophysiology
is a congenital abnormality characterized by incomplete or abnormal development of the ovaries, often resulting in non-functional ovaries.
Ovarian Dysgenesis: Clinical Signs
Clinical signs include small, underdeveloped ovaries, anestrus or absent estrous cycles, and failure to conceive.
Ovarian Dysgenesis: Diagnostics
Diagnostics often involve ultrasonography revealing underdeveloped ovaries and hormonal assays showing abnormal reproductive hormone levels.
Ovarian Dysgenesis: Treatment
Treatment focuses on supportive care for managing infertility; there is no cure due to the congenital nature of the condition.
Ovarian Dysgenesis: Prevention
Prevention strategies include genetic counseling and breeding management to avoid known hereditary issues.
Anovulatory Follicles: Pathophysiology
occur when a follicle fails to rupture during ovulation, leading to hemorrhage within the follicle and mimicking cystic structures.
Anovulatory Follicles: Clinical Signs
Clinical signs include prolonged estrous cycles, irregular hormone levels, and large, persistent follicles observed on ultrasound that do not rupture.
Anovulatory Follicles: Diagnostics
Diagnosis involves rectal palpation, ultrasonography showing large fluid-filled follicles, and hormonal assays confirming dysregulation.
Anovulatory Follicles: Treatment
Treatment may include hormonal therapies such as human chorionic gonadotropin (hCG) or GnRH analogs to induce ovulation; success may vary.
Anovulatory Follicles: Prevention
Preventive measures involve monitoring hormonal levels and reproductive cycles in susceptible mares to identify issues early.
Pathophysiology of Patent Urachus
is a condition in which the urachus, a tube that connects the fetal bladder to the allantoic sac during gestation, fails to close after birth. This leads to a persistent state where urine continues to leak from the umbilicus. It can be congenital or acquired, with congenital cases often linked to abnormal development of the umbilical structures or fetal urinary system, while acquired cases may result from trauma, infections, or excessive abdominal pressure.
Clinical Signs of Patent Urachus
typically present with:
Urine dribbling from the umbilicus: Noticeable soon after birth or within the first few days.
Moist umbilicus: Constant leakage may lead to a malodorous area around the umbilicus.
Umbilical swelling: Inflammation or abscess formation around the umbilicus.
Signs of systemic illness: Possible lethargy, fever, anorexia, and signs of sepsis.
Diagnostics for Patent Urachus
A thorough diagnostic workup includes:
Physical Examination: Observation of urine leaking and palpation for swelling or signs of infection.
Ultrasonography: Assessment of umbilical structures and detection of abnormalities.
Blood Work: Complete blood count (CBC) and serum biochemistry to identify systemic infection or inflammation.
Urine Culture: Bacterial culture from the umbilicus or urachus to identify infectious agents.
Treatment for Patent Urachus
The treatment strategy depends on severity and infection:
Conservative Management:
Topical Antiseptics: Cleaning with antiseptics for mild cases without systemic signs.
Systemic Antibiotics: Broad-spectrum antibiotics for foals with signs of infection.
Surgical Intervention:
Umbilical Resection: Surgical removal of the patent urachus and infected structures when conservative management fails.
Laparoscopic Surgery: Minimally invasive option for some cases.
Prevention of Patent Urachus
Preventive measures include:
Proper Handling: Avoid excessive manipulation of the umbilical stump.
Monitoring: Early identification of signs in premature or dystocia-affected foals.
Infection Control: Ensuring good hygiene to lower risks of umbilical infections.
Prematurity: Pathophysiology
is characterized by an early termination of gestation, resulting in the delivery of a foal that has not completed the final stages of fetal development. Critical development occurs during the last month of gestation, particularly in the lungs, musculoskeletal system, and thermoregulatory mechanisms. Premature foals, therefore, have immature lungs, which often lack adequate surfactant production, leading to respiratory distress syndrome (RDS). Additionally, underdeveloped musculoskeletal tissues result in weak bones, tendons, and muscles, impacting mobility.
Dysmaturity: Pathophysiology
refers to foals born at term or post-term but showing signs of immaturity due to intrauterine growth restriction. This condition often stems from placental insufficiency, which may be associated with placentitis, twins, or maternal illness. Placental abnormalities restrict the delivery of oxygen and nutrients to the fetus, disrupting normal fetal growth and development.
Premature Foals: Clinical Signs
Underdeveloped Physical Features: Small size, silky coat, domed forehead, and floppy ears.
General Weakness: Poor suckling reflex, difficulty standing, and lethargy.
Musculoskeletal Abnormalities: Flexor tendon laxity leading to fetlock hyperextension and incomplete ossification of the carpal and tarsal bones, increasing the risk of fractures and angular limb deformities.
Respiratory Distress: Rapid, shallow breathing with nasal flaring, resulting from immature lungs and insufficient surfactant.
Gastrointestinal Immaturity: Poor gut motility, predisposing foals to colic, ileus, and reduced absorption of colostrum.
Dysmature Foals: Clinical Signs
Physical Signs: While they may be normal in size, they present with an abnormally long and silky coat, domed forehead, floppy ears, and a small, frail appearance.
Weakness and Poor Suckling: Similar to premature foals, dysmature foals may struggle to stand, nurse, and maintain body temperature.
Respiratory Compromise: Mild to moderate respiratory distress due to underdeveloped lungs.
Angular Limb Deformities: Incomplete ossification of bones due to restricted fetal growth.
Metabolic Instability: Dysregulated glucose levels, electrolyte imbalances, and failure to thrive.
Prematurity and Dysmaturity: Diagnostics
Physical Examination: Initial examination should focus on identifying hallmark physical signs such as size, coat characteristics, ear cartilage pliability, and limb strength.
Radiography: Essential for evaluating the degree of ossification in the carpal and tarsal bones.
Bloodwork: Arterial blood gas analysis, CBC and biochemistry, serum immunoglobulin G (IgG) concentration.
Ultrasound: Evaluation of fetal size, placental thickness, and presence of placentitis in utero.
Pulmonary Function Testing: To confirm lung maturity, although this is not always feasible in the field setting.
Treatment for Prematurity and Dysmaturity
Supportive Care:
Thermoregulation: Controlled environment to maintain body temperature.
Nutrition: Enteral feeding with high-quality colostrum; intubation for weak suckling reflex cases.
Intravenous Fluids: To correct dehydration and electrolyte imbalances.
Antibiotic Therapy: Broad-spectrum antibiotics due to high risk of sepsis.
Oxygen Therapy: Supplemental oxygen for respiratory distress.
Joint and Limb Support: Bandaging and splinting as necessary.
Medications: Glucocorticoids to enhance surfactant production.
Prevention of Prematurity and Dysmaturity
Maternal Health Management: Monitor for illnesses such as equine metabolic syndrome, placentitis, or inadequate nutrition.
Avoid Twin Pregnancies: Minimize the risks associated with multiple gestations.
Induction Protocols: Ensure labor is not induced without confirming fetal maturity.
Monitoring for Prematurity and Dysmaturity
Continuous monitoring of blood glucose, electrolyte levels, and arterial blood gases to detect metabolic disturbances early.
Frequent assessment of bone development through radiographs to prevent orthopedic issues.
Prognosis for Prematurity and Dysmaturity
The prognosis depends on the severity of clinical presentation, the degree of organ system immaturity, and the level of care provided. Early intervention with aggressive supportive care can improve survival rates, though some foals may develop long-term complications.
Pathophysiology of Retained Placenta
is a common postpartum complication in mares, defined as the failure to expel the fetal membranes within 3 hours after foaling. The placenta consists of a microcotyledonary structure, where fetal membranes are intimately associated with the endometrium. Retained placenta occurs due to several underlying mechanisms, including:
Uterine Atony: Insufficient uterine contractions postpartum, often seen in dystocia, uterine inertia, or systemic illness.
Inadequate Separation: Failure of the connection between microcotyledons and endometrium to release, potentially due to premature placental detachment or inflammation.
Hormonal Imbalances: Anomalies in the production of prostaglandin and oxytocin impair uterine contractions.
Vascular Compromise: Damage to the endometrial blood supply can affect normal placental detachment.