Sport Injury Prevention Midterm
0.0(0)
Studied by 0 peopleCard Sorting
1/107
Earn XP
Description and Tags
Last updated 10:11 PM on 2/16/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
1
New cards
why is sport injury prevention important?
\-severe long term effects
\-mental health effects
\-public healthcare costs
\-change in functions
\-sustainable long-term sport participation and physical activity
\-improved performance
\-forced retirement
\-mental health effects
\-public healthcare costs
\-change in functions
\-sustainable long-term sport participation and physical activity
\-improved performance
\-forced retirement
2
New cards
what sports have the highest burden of sports injury?
soccer, basketball, and hockey
3
New cards
what sports have the highest injury rates?
team sports: handball, soccer, hockey, rugby, american football, aussie rules football
4
New cards
what sports have the highest risk of head injury?
alpine skiing, snowboarding, soccer, hockey, rugby, football, and boxing
5
New cards
what sports have the highest risk of knee injuries?
pivoting sports: soccer, handball, basketball, football, and alpine skiing
6
New cards
what are the consequences of sport injuries?
\-time loss from school, sports, and work
\-lower physical activity
\-decreased mental health, social engagement
\-increased costs to healthcare systems
\-decreased overall well-being
\-increased risk of reinjury
\-increased risk of osteoarthritis, other long-term consequences
\-disability
\-obesity
\-post concussion syndrome
\-lower physical activity
\-decreased mental health, social engagement
\-increased costs to healthcare systems
\-decreased overall well-being
\-increased risk of reinjury
\-increased risk of osteoarthritis, other long-term consequences
\-disability
\-obesity
\-post concussion syndrome
7
New cards
what is primary prevention?
preventing injury in those who are uninjured
8
New cards
what is secondary prevention?
detecting injury in its earliest stages and early treatment to halt/slow its progression
9
New cards
what is tertiary prevention?
interventions to stop the progress of an established injury and prevent long-term consequences
10
New cards
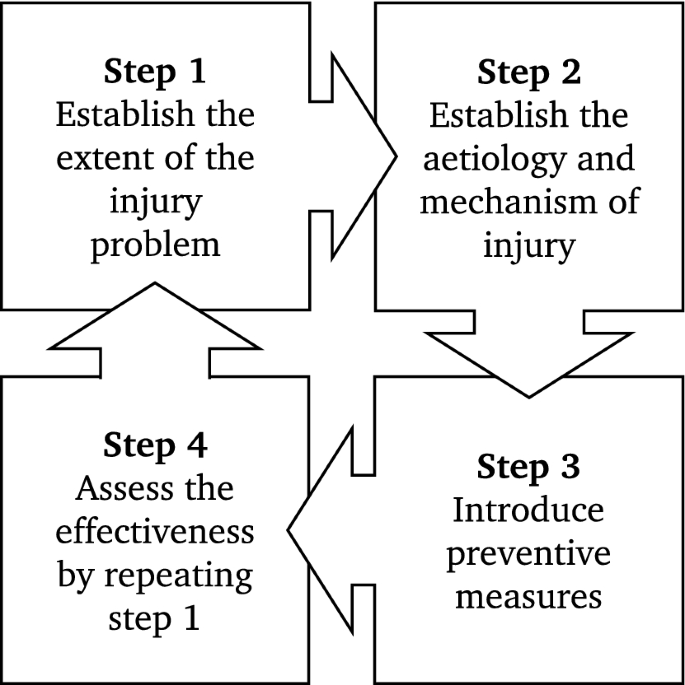
what is the 4-step sequence of sport injury prevention research?
establishing the extent of the injury problem (incidence and severity) → establishing injury etiology and mechanism → introduce a preventative measure → assess its effectiveness→ repeat cycle again
11
New cards
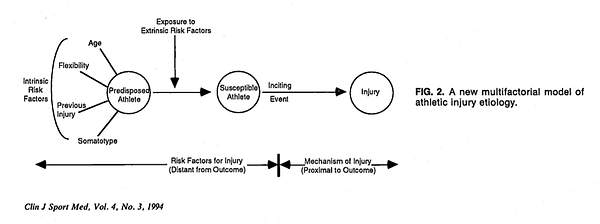
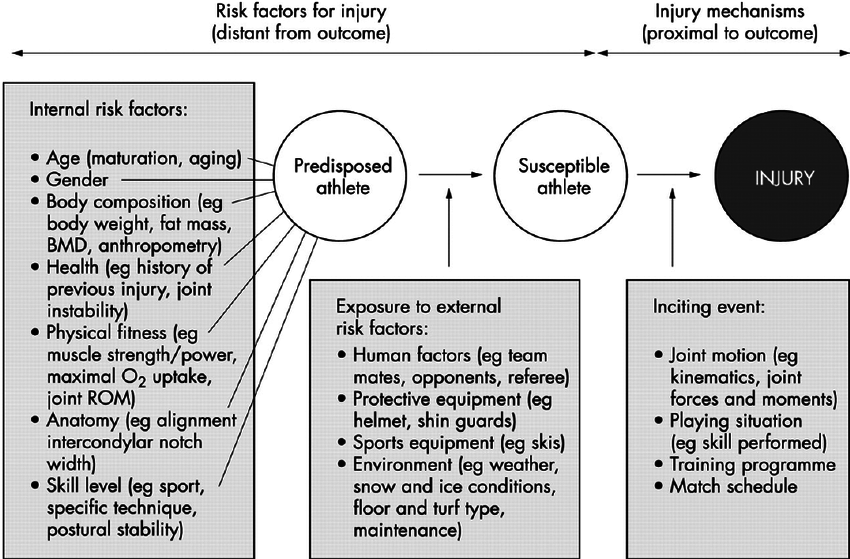
what is the multifactorial model of athletic injury etiology?
assessment of intrinsic risk factors creating a predisposed athlete, who is then exposed to extrinsic risk factors creating a susceptible athlete. an inciting incident then must occur for an injury to happen
12
New cards
what is the comprehensive model for injury causation?
similar to the multifactorial model with assessment of risk factors however this model focuses on the inciting event as being the most important. Factors contributing to the inciting event include: playing situation, player/opponent behaviour, whole body biomechanical descriptions, and detailed, single joint biomechanical descriptions of injury mechanism
13
New cards
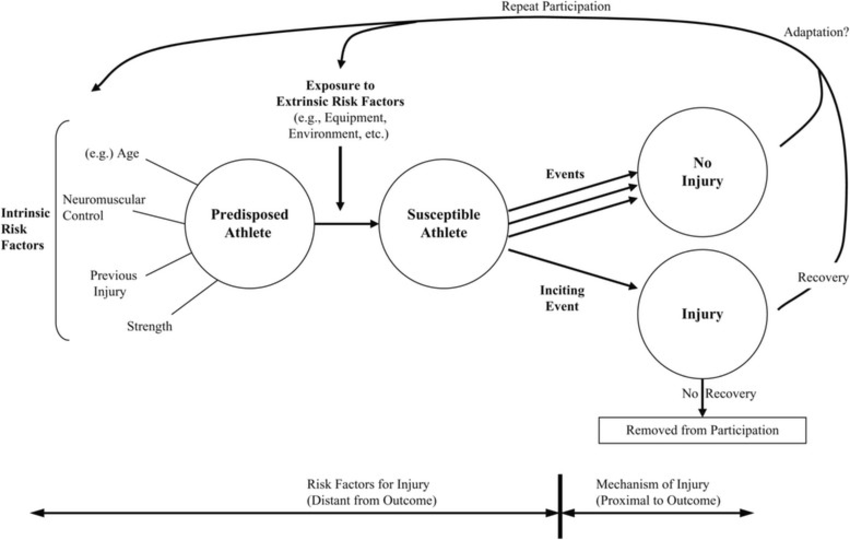
what is the dynamic model of etiology in sport injury?
builds more onto the multifactorial model. Describes how risk factors are transient and constantly changing. A susceptible athlete can go through many risky situations without injury occuring leading to adaption/maladaption. however once an injury occurs after an inciting event they can either recover, adapt, and then continually modify their risk factors, or there is no recovery and they are removed from participation
14
New cards
what is the haddon matrix?
a logical framework for categorizing highway safety phenomena and activity
15
New cards
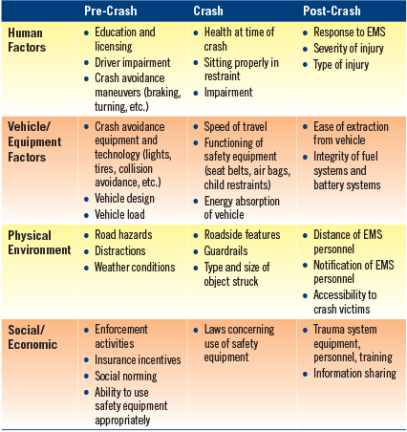
what is the modified haddon matrix?
model used for sport injury, used to assess athlete, environment, and equipment factors at pre-event, event, and post-event time points
16
New cards
what is the TRIPP framework?
Translating Research into Injury Prevention Practice: extends the van mechelen model after the fourth stage to knowledge translation. 5: describe intervention context to inform implementation strategies, 6: evaluate effectiveness of preventative measures in implementation context
17
New cards
what are the four overarching types of study designs in injury prevention?
descriptive: qualitative, case study, and cross-sectional studies (assess who, what, where)
analytic exploratory: qualitative, cross-sectional, case-control, cohort studies
analytic experimental: RCT, quasi-experimental study
synthesis of primary studies: scoping and systematic reviews, meta-analysis
analytic exploratory: qualitative, cross-sectional, case-control, cohort studies
analytic experimental: RCT, quasi-experimental study
synthesis of primary studies: scoping and systematic reviews, meta-analysis
18
New cards
what is the purpose of qualitative studies?
\-provide deeper insights into real-world problems
\-complete and detailed descriptions of the research topic
\-deals with understanding the individuals attitudes, beliefs, behaviour, motivation, values, and perceptions
\-help develop ideas or hypotheses for quantitative studies
\-complete and detailed descriptions of the research topic
\-deals with understanding the individuals attitudes, beliefs, behaviour, motivation, values, and perceptions
\-help develop ideas or hypotheses for quantitative studies
19
New cards
what are the disadvantages of qualitative studies?
\-can be largely affected by the researchers biases
\-lack replicability
\-can be prone to selection bias
\-lack replicability
\-can be prone to selection bias
20
New cards
where can qualitative studies be used?
in stage 1 of van mechelen → establishing injury problem
21
New cards
what are case studies used for?
to give descriptive characteristics of a specific injury and its associated variables. generates an in-depth understanding of a complex issue in its real world environment, generally used to describe rare events
22
New cards
what are the disadvantages of case studies?
\-cannot establish causation or temporality
\-cannot be generalized
\-cannot be generalized
23
New cards
where can case studies be used in the van mechelen model?
stage 2 → establishing etiology and mechanisms of injury
(potentially in stage 3→ intervention intro)
(potentially in stage 3→ intervention intro)
24
New cards
what are the advantages of cross-sectional studies?
\-describes outcomes, characteristics, and exposures in the population, at a specific time
\-gives ideas for future studies
\-inexpensive
\-easy data acquisition
\-gives ideas for future studies
\-inexpensive
\-easy data acquisition
25
New cards
what are the disadvantages of cross-sectional studies?
\-no follow-up period
\-is difficult to determine whether the injury followed the exposure of the exposure resulted from the outcome
\-recall bias and missing information
\-is difficult to determine whether the injury followed the exposure of the exposure resulted from the outcome
\-recall bias and missing information
26
New cards
when should cross-sectional studies be used in the van mechelen model?
stage 1 → establishing injury problem
27
New cards
what are the advantages of case-control studies?
\-can establish relationship between exposures and specific outcomes
\-are efficient for studying rare outcomes
\-relatively inexpensive
\-usually quick to complete
\-are efficient for studying rare outcomes
\-relatively inexpensive
\-usually quick to complete
28
New cards
what are the disadvantages of case-control studies?
\-usually retrospective so recall bias
\-inefficient for rare exposures
\-prone to selection bias
\-inefficient for rare exposures
\-prone to selection bias
29
New cards
when should case control studies be used in the van mechelen model?
stage 2 → establishing injury etiology and mechanism
30
New cards
what are the advantages of cohort studies?
\-can compare injury occurence in groups that have different exposures over time
\-demonstrates temporal relationship between exposures and outcome
\-provides good descriptive information about exposures
\-efficient for studying rare exposures, common outcomes and multiple outcomes
\-demonstrates temporal relationship between exposures and outcome
\-provides good descriptive information about exposures
\-efficient for studying rare exposures, common outcomes and multiple outcomes
31
New cards
what are the disadvantages of cohort studies?
\-expensive
\-requires large numbers
\-takes a long time
\-requires large numbers
\-takes a long time
32
New cards
where should cohort studies be used in the van mechelen model?
stage 2→ establishing injury etiology and mechanism
(potentially stage 4→ assessing effectiveness but not as good as RCT)
(potentially stage 4→ assessing effectiveness but not as good as RCT)
33
New cards
what are the advantages of RCTs?
\-most reliable form of scientific evidence
\-controls confounding and allows generalization of results
\-high internal validity
\-controls confounding and allows generalization of results
\-high internal validity
34
New cards
what are the disadvantages of RCTs?
\-expensive and time-consuming
\-rare outcomes necessitate large numbers
\-difficulties with participant compliance
\-low external validity
\-rare outcomes necessitate large numbers
\-difficulties with participant compliance
\-low external validity
35
New cards
when should RCTs be used in the van mechelen model?
stage 4→ establishing the effectiveness of an intervention
36
New cards
what is injury surveillance?
the collection of data describing the occurrence, characteristics, and factors associated with an injury
addresses: rate, severity, and types of injuries, the athlete factors associated with the injury and the typical injury patterns
addresses: rate, severity, and types of injuries, the athlete factors associated with the injury and the typical injury patterns
37
New cards
what features is successful injury surveillance dependent on?
\-valid and reliable definitions
\-accurate data collection and careful analysis
\-accurate data collection and careful analysis
38
New cards
why are consensus statements important?
consensus statements on injury definitions and data collection allows for standardization and comparisons to be made in injury surveillance
39
New cards
what is the definition of a sport injury?
tissue damage or other derangement of normal physical function due to participation in sports, resulting from rapid or repetitive transfer of kinetic energy
40
New cards
what are the broad types of sport injuries?
all complaints → medical attention → time loss → match time loss
41
New cards
how is sport injury severity determined?
generally by the number of days from injury to date of full RTP
slight = 0 days
minor = 1-7 days
minimal = 1-3 days
mild = 4-7 days
moderate = 8-28 days
severe = more than 28 days
career-ending injury
slight = 0 days
minor = 1-7 days
minimal = 1-3 days
mild = 4-7 days
moderate = 8-28 days
severe = more than 28 days
career-ending injury
42
New cards
what is prevalence of sport injury?
total 3 of injuries at a specific time in a specific population. n exisiting injuries/total population
43
New cards
what is the difference between point and period prevalence?
point prevalence = amount of injuries right now, at a specific point in time
period prevalence = amount of injuries over a period of time (i.e. year, season, etc)
period prevalence = amount of injuries over a period of time (i.e. year, season, etc)
44
New cards
what is incidence?
number of new occurences of an injury over a specific period, can be described as a rate of new injuries/unit of person-time (athlete years, exposure hours, etc.)
45
New cards
what is the difference between training and game exposure?
training = team based and individual physical activities under the control/guidance of coaching/fitness staff, includes pre and post-game warmups and cooldown, does not include rehabilitation or personal training
game = play between teams from different clubs (i.e. not scrimmages
game = play between teams from different clubs (i.e. not scrimmages
46
New cards
How are sport injuries classified?
location of injury and body side, type of injury, first time vs. subsequent injury, training or game injury, and mechanism of injury
47
New cards
what is an index injury?
the first recorded injury
48
New cards
what is an exacerbated injury?
injury to the same location and tissue as the original injury when the original injury was not fully healed yet
49
New cards
what is an injury recurrence?
an injury to the same location and tissue as the original injury if the first injury was fully healed
50
New cards
what is a subsequent local injury?
an injury to the same location but a different tissue than the original injury
51
New cards
what is a subsequent new injury?
an injury to a new location, different than the original injury
52
New cards
what are the types of acute injuries?
direct contact, indirect contact, or non-contact injuries
53
New cards
what are the types of overuse injuries?
repetitive (gradual onset) or repetitive (sudden onset)
54
New cards
what are the categories of injury mechanism descriptions?
sport situation (team action, court position, player position, skill performed), athletes behaviour, whole body biomechanics, joint tissue biomechanics
55
New cards
how is data collected on injury mechanism?
interviews, clinical studies (imaging and surgery), analysis of video recordings of actual injuries, lab motion analysis, injuries during biomechanical experiments, cadaver and dummy studies, mathematical modeling and simulation of injury situation
56
New cards
what is the most common ACL injury situation in soccer?
non-contact or indirect contact situations: pressing in defensive play, regaining balance during landings after heading and kicking
57
New cards
what is the most common ACL mechanism in soccer?
dynamic valgus movement of the knee, full body weight on 1 leg, relatively straight knee
58
New cards
what are the recommendations for preventing ACL injuries?
teach proper single leg landing techniques, change of direction technique, proper limb alignment, movement control of core and lower extremities before ground contact, no tackling from behind
59
New cards
what is the most common head injury situation in skiing and snowboarding?
when landing or turning from a jump, pitching backwards or sideways falls, impacts to the back or side of the head
60
New cards
what is the common head injury mechanism in downhill sports?
common landing sequence: skis/board → upper or lower extremity → butt/pelvis → back → head
61
New cards
what is the mechanism for ankle injuries?
sudden inversion and internal rotation, slightly inverted ankle orientation, centre of pressure shifts laterally
62
New cards
what are the two axes of the ankle joint and what movements do they allow for?
ankle joint axis → plantar and dorsiflexion
subtalar axis → supination, pronation (abduction and addution)
subtalar axis → supination, pronation (abduction and addution)
63
New cards
what is the function of tibialis anterior and triceps surae?
tib ant = good dorsiflexor, poor adductor
triceps surae = good plantarfexor, medial terrible adductor, lateral terrible abductor
triceps surae = good plantarfexor, medial terrible adductor, lateral terrible abductor
64
New cards
why are tib ant and triceps surae terrible pronators and supinators?
very small moment arm, have to asymetrical
65
New cards
why do we need small muscles crossing the ankle joint?
if only had tib ant and triceps surae, would have to asymetrically load the achilles tendon
would have huge local forces making it very easy to injure (in order to stabilize the ankle need a lot of co-contraction)
many small muscles allow for better control and decreased forces
would have huge local forces making it very easy to injure (in order to stabilize the ankle need a lot of co-contraction)
many small muscles allow for better control and decreased forces
66
New cards
how do we train ankle muscles?
must be trained in all 6 directions, at maximal force, for at least ten seconds
67
New cards
what is a risk factor?
a condition, behaviour, or other factor that increases the risk of injury, can be either intrinsic or extrinsic
68
New cards
what is the complex system approach for sport injuries?
model that describes risk factors as an interconnected web that are all interacting and constantly changing
69
New cards
what are the two types of hamstring strains?
sprint-related: occurs during late swing or early stance phase with huge eccentric biecps femoris contraction
stretch-related: occurs during extensive hip flexion with exttended knee, rapid overstretching of semimembranosus
stretch-related: occurs during extensive hip flexion with exttended knee, rapid overstretching of semimembranosus
70
New cards
what are the risk factors for hamstring strains?
previous hamstring strain, older age, reduced hip ROM, poor hamstring strength, superior running speed, low back pain, muscle fatigue, insufficient warm-up, level of play, changes in training program
71
New cards
what are the risk factors for ankle sprain?
previous ankle sprain, limited dorsiflexion, reduced proprioception, deficiencies in balance, female, lower BMI, decreased peroneal reaction time, pivoting sport
72
New cards
what are the risk factors for knee ligament injuries?
previous knee joint injury, female, high knee adbduction moments during landing and cutting, stiff landings, landing with a heel strike, weak hip abductor strength, poor core stability, high friction surfaces
73
New cards
what is the relationship between training load and injury risk?
some studies shown that spikes in training load increase injury risk, and high absolute loads increase injury risk
74
New cards
What elements are necessary in a risk management system for a team?
injury surveillance, season analysis, preseason screening, athlete monitoring, return to sport, education, equipment and facilities, emergency action plan
75
New cards
what are the effects of helmets on the risk of head and neck injuries in downhill sports?
protective, no evidence suggesting increased neck injury risk
76
New cards
what are the effects of wrist guards in wrist and arm injuries in snowboarders?
protective for wrists, some evidence that might result in elbow/shoulder injuries instead but still overall reduction
77
New cards
what is risk compensation theory?
each person has a target level of risk that they are willing to accept, and if they perceive an intervention has lowered their level of risk, then they will change their behaviour to bring it back to their target level of risk
78
New cards
what affects an individuals target level of risk?
\-expected advantages from the risky behaviours
\-expected costs from the risky behaviour
\-expected benefits from safe behaviour
\-expected costs of safe behaviour
\*trying to maximize net benefits
\-expected costs from the risky behaviour
\-expected benefits from safe behaviour
\-expected costs of safe behaviour
\*trying to maximize net benefits
79
New cards
what are hedlund’s rules for risk compensation?
1: If I don’t know its there, I won’t compensate for a safety measure
2: If it doesn’t affect me, I won’t compensate for a safety measure
3: If I have no reason to change my behaviour, I won’t compensate for a safety measure
4: if my behaviour is tightly controlled, I won’t compensate for a safety measure
2: If it doesn’t affect me, I won’t compensate for a safety measure
3: If I have no reason to change my behaviour, I won’t compensate for a safety measure
4: if my behaviour is tightly controlled, I won’t compensate for a safety measure
80
New cards
What sex differences exist for injuries in team differences?
males have higher rate of overall, upper extremity, hip/groin, thigh, and foot injuries
females have 2-times higher rate of ACL injuries
no differences in concussions, ankle sprains, or achilles tendon
females have 2-times higher rate of ACL injuries
no differences in concussions, ankle sprains, or achilles tendon
81
New cards
what sex differences exist for injuries in runners?
no difference between sexes for overall injuries
female runners are twice as likely to have stress fractures, and 2-10 times more likely to have patellofemoral pain
male runners have higher risk of achilles tendinopathy and hamstring strain
female runners are twice as likely to have stress fractures, and 2-10 times more likely to have patellofemoral pain
male runners have higher risk of achilles tendinopathy and hamstring strain
82
New cards
what sex differences exist for injuries in elite alpine skiiers?
males have higher risk of overall injuries, low back, and pelvis injuries
no sex difference in risk of knee and ACL injuries
no sex difference in risk of knee and ACL injuries
83
New cards
what anatomical differences may predispose female athletes to knee injuries?
females have greater pelvic width, greater hip internal rotation, greater knee external rotation, greater knee valgus, greater quadriceps angle
84
New cards
what is the relationship between knee valgus, q angle, and knee injuries?
q angle is the angle between the quad muscle and patellar tendon and increases with greater knee valgus.
q angle is not related to ACL injuries, more related to patellar injuries
Knee valgus is related to ACL injuries
q angle is not related to ACL injuries, more related to patellar injuries
Knee valgus is related to ACL injuries
85
New cards
What is the relationship between the intercondylar notch and ACL injuries?
proposed that females have narrower intercondylar notch, potentially leading to smaller or weaker ACLs
86
New cards
what neuromuscular factors may predispose females to knee injuries?
\-ligament dominance: greater reliance on passive subsystem to absorb ground reaction forces
\-quadriceps dominance: use of quads rather than hamstrings for knee stabilization
\-leg dominance: more likely to have imbalance between right and left leg
\-trunk dominance: impaired trunk muscular control
\-quadriceps dominance: use of quads rather than hamstrings for knee stabilization
\-leg dominance: more likely to have imbalance between right and left leg
\-trunk dominance: impaired trunk muscular control
87
New cards
what biomechanical factors may predispose females to knee injuries?
\-different running mechanics
\-different cutting mechanics
\-different landing mechanics
\-different cutting mechanics
\-different landing mechanics
88
New cards
what gendered envrionmental factors may predispose women to ACL injuries?
pre-sport environment: gendered parenting, expectations, and stereotyping
sport participation: starting age, quality of coaching, quality of facilities, quality of training, support systems
sport participation: starting age, quality of coaching, quality of facilities, quality of training, support systems
89
New cards
what are the primary targets for prevention of sport injuries?
training strategies, rule modifications, equipment recommendations
90
New cards
what are the most common strategies used in sport injury prevention studies?
training programs to improve fitness/movement quality,
new/modifiedsport equipment
new/modified rules
coach or referee education
policy change
training programms to improve psychological or cognitive skills
new/modifiedsport equipment
new/modified rules
coach or referee education
policy change
training programms to improve psychological or cognitive skills
91
New cards
what areas do we need more intervention studies in?
specific injury types (hamstring strains, shoulder, low back, and overuse injuries)
individual sports
female athletes
rehabilitation
individual sports
female athletes
rehabilitation
92
New cards
what effective interventions exist for reducing injury risk?
NMT programs
Insoles
external joint supports
Insoles
external joint supports
93
New cards
how can we prevent hamstring injuries?
eccentric strength training → nordic hamstring curls
94
New cards
how can we prevent ankle sprains?
NMT and proprioceptive training, bracing
95
New cards
how can we prevent knee injuries?
NMT programs to increase core and lower limb strength and stability, awareness of knee position, and quality of movement
96
New cards
what is the neuromuscular system?
the nervous system and muscles working together to control, direct, and allow movement of the body
97
New cards
what is neuromuscular control?
the ability to produce controlled movement through coordinated muscle activity and dynamic joint stability and postural control
98
New cards
what are the aims of neuromuscular training?
\-to improve the nervous system’s ability to generate a fast and optimal muscle firing pattern
\-to increase dynamic joint stability
\-to decrease joint forces
\-to learn movement patterns and skills
\-to increase dynamic joint stability
\-to decrease joint forces
\-to learn movement patterns and skills
99
New cards
what are the critical teaching points for skipping in NMT warmup?
keep elbows at 90 degrees, keep upright posture, and proper arm swing
100
New cards
what are the critical teaching points for hip-hinge exercise in NMT warmup?
\-keep hands on hips
\-slow and controlled movements
\-look straight to maintain balance
\-slow and controlled movements
\-look straight to maintain balance