NURS 5334 Advanced Pharmacology Module 2 actual questions with 100% correct answers + detailed explanations
1/142
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
143 Terms
identification of teratogens
difficult to identify, 3 criteria must be met:
1. The agent must be present during the critical stage of development
2. The agent produces a particular pattern of birth defects in animal studies.
3. The agent crosses the placenta and there is a dose-response relationship.
3 stages of teratogenesis development
1. conception through week 2
2. embryonic period week 3-8 = gross malformations
3. fetal period week 9-delivery = functions disrupted w/ teratogen exposure
physiologic changes during pregnancy & drug impact
- 3rd trimester = renal blood doubles, renal excretion accelerated
- tone and mobility of bowel decreases -> prolongation of drug effects
placental drug transfer
all drugs can cross the placenta, some cross more easily than others
adverse reactions during pregnancy
can adversely affect both pregnant pt and fetus
- heparin -> osteoporosis
- prostaglandins -> stimulate uterine contraction
- some pain relievers can be used during delivery can cause respiratory depression in baby
teratogenesis birth defects
gross malformations = cleft palate, clubfoot, hydrocephalus
neurobehavioral & metabolic anomalies
responding to teratogen exposure
Determine when the drug was taken
Determine when the pregnancy began
-Weeks 3-8 (organogenesis) is most crucial time
Determine type of malformation expected
Conduct 2 US and consult FDA to determine severity
how to decrease risk of drug effects during breastfeeding
- take drugs immediately after breastfeeding
- avoid drugs w/ long half-lives
- choose drugs that tend to be excluded from milk, least likely to affect infant
- avoid hazardous drugs
pediatric response to drugs
- more sensitive to drugs
- greater individual variation
- sensitivity d/t organ system immaturity
- increased risk for adverse rxns
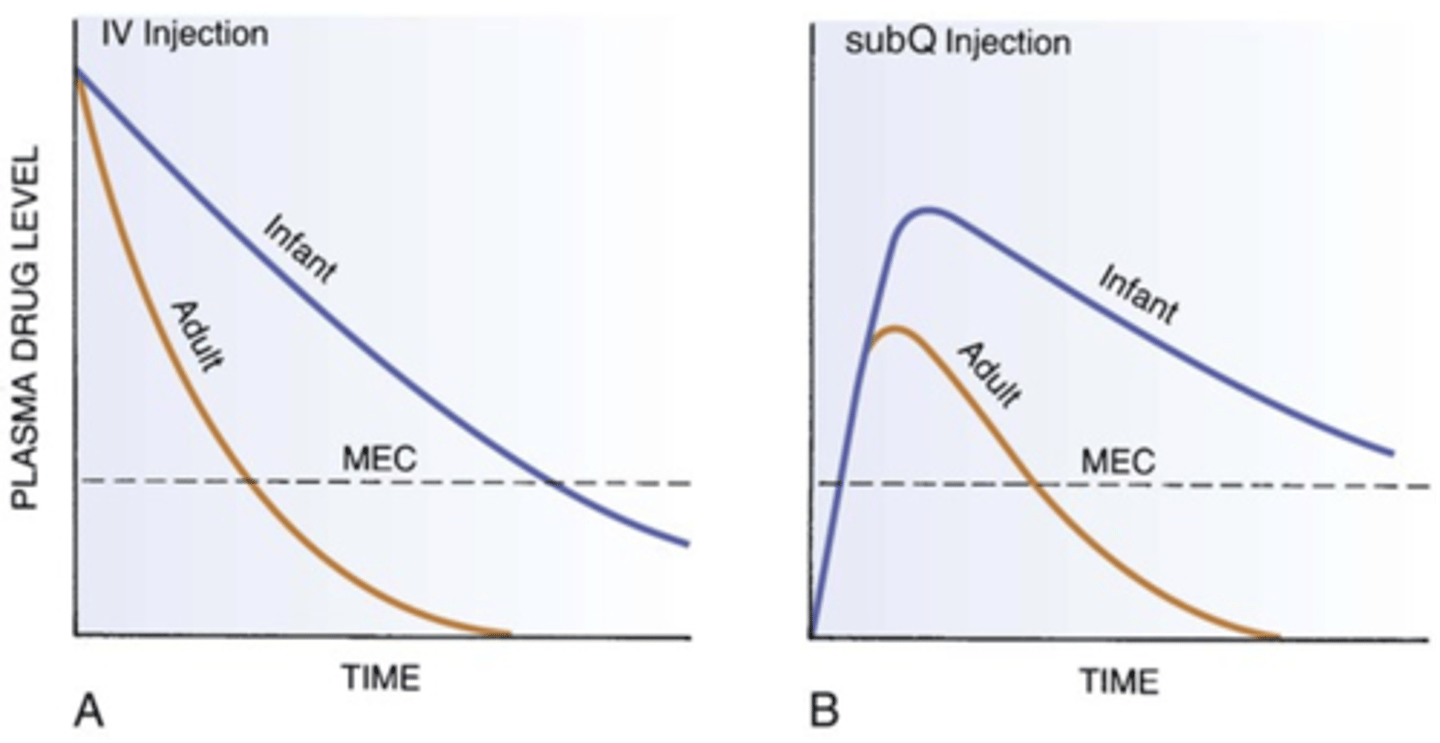
determining the intensity of duration of drug response in neonates & infants
- elevated drug levels = more intense response
- delayed elimination = prolonged response
- immaturity of organs = risk for both^
comparison of plasma drug levels in adults and infants
increased sensitivity in infants caused by immature state of...
absorption, protein binding of drugs, BBB, hepatic metabolism, renal drug excretion
infant absorption: oral administration
prolonged and irregular gastric
adult function at 6-8 months
infant absorption: gastric acidity
- very low 24 hours after birth
- does not reach adult values for 2 years
- low acidity = absorption of acid-labile drugs is increased
infant absorption: intramuscular admin
slow, erratic, delayed absorption as results of low blood flow in 1st few days of life
in early infancy, absorption of IM drugs more rapid than neonates & adults
infant absorption: transdermal
more rapid & complete for infants than older children & adults
- stratum corneum of infant's skin is thin
- blood flow to skin is greater in infants than older patients
- infants increased risk for toxicity from topical drugs
infant distribution: BBB
- not fully developed at birth
- drugs have easy access to CNS
- infants especially sensitive to drugs that affect CNS function
- dosage should be reduced for drug actions outside the CNS if those drugs are capable of producing toxicity as a side effect
infant hepatic metabolism
- drug-metabolizing capability of newborns is low
- liver's capability to metabolize drugs increases fast @ 1mo
- complete liver maturation occurs at 1yr
infant renal excretion
- low renal blood flow, glomerular filtration, & active tubular secretion
- drugs eliminated by renal excretion must have reduced dosing and/or longer dosing intervals
- adult level renal function occurs at 1yr
pharmacokinetics in children
metabolize drugs faster than adults till 2yrs, then gradual decline
sharp decline at puberty
may need to increase or decrease interval between doses
adverse drug reactions in children
- glucocorticoids -> growth suppression
- tetracyclines -> discoloring of teeth
- sulfonamides -> kernicterus
- fluoroquinolones -> musculoskeletal d/o's
- SSRIs - > black box increased SI
- OTC cough and cold meds not recommended in kids <2yrs
dosage determination in children
child's BSA x adult dosage/ 1.73m2 = child dose
older adults: altered pharmacokinetics
more sensitive to drugs than younger adults & w/ greater variation in pharmacokinetics
multiple & severity of illness, multiple pathologies
multiple-drug therapy (excessive prescribing)
poor adherence
older adults: absorption
- rate of absorption slows w/ age
- delayed gastric emptying & reduced splanchnic blood flow
older adults: distribution
- increased body fat % (storage depot for lipid-soluble drugs)
- decreased lean body mass %
- decreased total body water (distributed in smaller volume, concentration increased & effects more intense)
- reduced concentration of serum albumin -> decreased protein binding of drugs & increased levels of free drugs
older adults: metabolism
- hepatic metabolism declines
- reduced hepatic blood flow & liver mass
- decreased activity of hepatic enzymes
- half-life of some drugs may increase
- prolonged & enhanced drug responses
older adults: excretion
- decline in renal function, blood flow, GFR, active tubular secretion, # of nephrons
- drug accumulation d/t reduced renal excretion**
pharmacodynamic changes in older adult patients
- drugs w/ more intense effects
- beta blockers less effective, even in same concentrations
adverse drug reactions in older adults
7x more likely than adults
majority are dose related, not idiosyncratic
symptoms are often nonspecific
predisposing adverse reaction factors in older adults
- Drug accumulation secondary to reduced renal function
- Polypharmacy
- Greater severity of illness
- Multiple pathologies
- Greater use of drugs that have a low therapeutic index (e.g.,digoxin)
- Increased individual variations secondary to altered pharmacokinetics
- Inadequate supervision of long-term therapy
- Poor patient adherence
antimicrobials
used to treat infectious dx
significantly reduced morbidity and mortality from infection
classification of antibiotics
Drugs work on:
Cell wall synthesis
Cell membrane permeability
Protein synthesis (lethal)
Nonlethal inhibitors of protein synthesis
Synthesis of nucleic acids
Antimetabolites
Viral enzyme inhibitors
bactericidal
directly lethal to bacteria at achievable concentrations
bacteriostatic
slows bacterial growth but doesn't cause cell death
penicillin and cephalosporin MOA
inhibit cell wall synthesis-> bacterial lysis and death
___ MOA
increase cell membrane permeability -> leaking of ICF
aminoglycosides MOA
lethal inhibition of bacterial protein synthesis -> cell death
tetracyclines MOA
nonlethal inhibition of protein synthesis -> slow microbial growth (they do NOT kill bacteria)
rifampin, metronidazole, & fluroroquinolones MOA
binds to nucleic acids or interacts w/ enzymes required for nucleic acid synthesis -> inhibit bacterial synthesis of DNA and RNA or disrupt DNA function
antimetabolites (trimethoprim & sulfonamides) MOA
disrupt specific biochemical reactions -> decrease in synthesis of essential cell constituents or synthesis of nonfunctional analogs of metabolites
antiviral MOA
inhibit specific enzymes required for viral replication and infectivity
organisms w/ microbial drug resistance
Enterococcus faecium Staphylococcus aureus
Enterobacter species Klebsiella species
Pseudomonas aeruginosa
Acinetobacter baumannii
Clostridium difficile
4 basic microbial mechanisms of drug resistance
1. decrease concentration of drug @ site of action
2. inactivate drug
3. alter structure of drug target molecules
4. produce drug antagonist
NDM1 gene
can inactivate most all beta lactam abx
mechanisms for acquired resistance
-Spontaneous mutation (Random changes in a microbes DNA, resistance to one drug)
-Conjugation (extrachromosomal DNA is transferred from one bacterium to another, gram negative bacteria, multiple drug resistance)
which abx promote resistance?
broad-spectrum
more abx used, faster drug resistant organisms emerge
nosocomial infections
health care associated infections
superinfections
new infection appears during course of treatment for primary infection w/ drug resistant microbes
public health action plan to combat antimicrobial resistance
focus area 1 = surveillance
focus area 2 = prevention and control
focus area 3 = research
focus area 4 = product development
empiric therapy
abx therapy before causative organism is identified
prophylactic use of antimicrobials
surgery, bacterial endocarditis, neutropenia
penicllin structure
includes beta lactam ring
beta lactam family = cephalosporins, aztreonam, imipenem, meropenem, ertapenem
low toxicity
pencillins MOA
weaken cell wall -> cell rupture
bactericidal
3 mechanisms of bacterial resistance in penicillins
inability of penicillins to reach target
inactivation of penicillins by bacterial enzymes
production of penicillin binding proteins that have low affinity for penicillins
2 types of MRSA
health care associated MRSA
community associated MRSA
Penicillin G
bacterial to many gram positive & some gram negative prganisms
allergic reactions
Penicillin V
stable in stomach acid
replaced penicillin g for oral therapy
penicillinase resistant penicillins
Oxacillin, nafcillin, dicloxacillin
broad spectrum pencillins
ampicillin, amoxicillin
AE: rash, diarrhea
extended spectrum/antipseudomonal penicillins
Piperacillin
- broad spectrum, but penicillinase sensitive
- effective against organisms susceptible to aminopenicillins plus bacterial resistant antimicrobials
Beta-lactamase inhibitors
clavulanic acid, sulbactam, tazobactam
penicillin combinations
Extends antimicrobial spectrum when combined with penicillinase-sensitive antibiotics
- ampicillin/sulbactam (Unasyn)
- amoxicillin/clavulanic acid (Augmentin)
- piperacillin/taxobactam (Zosyn)
cephalosporins
most widely used abx group
beta lactam abx
bactericidal
low toxicity
cephalosporins MOA
B-lactam drugs that inhibit cell wall synthesis but less suspectible to penicillins -> cell lysis
1st generation cephalosporins
Cefazolin, cephalexin, Cefadroxil
2nd generation cephalosporins
Cefoxitin, cefaclor, cefuroxime, cefotetan, cefprozil, cefmetazole, cefonicid, loracarbef
3rd generation cephalosporins
cefotaxime, cefdinir, cefditoren, cefixime, cefpodoxime, cerazidime, cefibuten, ceftriaxone, cefoperazone, cefitzoxime
4th generation cephalosporins
Cefepime
5th generation cephalosporins
Ceftaroline
Ceftolozane
cefiderocol
new cephalosporin for MDR gram negative infections
used in adults w/ complicated UTIs and pyelo
cephalosporin drug interactions
Probenecid
Alcohol
Drugs that promote bleeding
Calcium and ceftriaxone
cephalosporin adverse effects
allergy, bleeding, thrombophlebitis
1st gen cephalosporin uses
prophylactically for surgery patients
2nd gen cephalosporin use
rarely used for active infections
3rd gen cephalosporin use
preferred therapy for several infections
highly active against gram-negative organisms
able to penetrate CSF
4th gen cephalosporin uses
HCA pneumonia including cause by pseudomonas aeruginosa
5th gen cephalosporin use
MRSA infection
carbapenems
Imipenem, Meropenem, Ertapenem, Doripenem
beta lactam abx
extremely broad spectrum
low toxicity
not active against MRSA
Imipenem
active against more bacterial pathogens & many resistant to other abx
highly effective against gram + cocci & omst gram - occi and bacilli
Vancomycin MOA, use
MOA = inhibit cell wall synthesis
use = serve infections, MRSA< staph, C diff
Vancomycin AE
ototoxicity, nephrotoxicity, red man syndrome, thrombophlebitis, thrombocytopenia
Telavancin
new class, lipoglycoproteins synthetic derivatives of vancomycin
effect only against gram +
AE: taste disturbance, NV, foamy urine, red man syndrome prolonged QT
BB warning! = HCA pneumonia w/ cr clearance <50
Monobactam
Aztrenonam
narrow spectrum
gram - aerobic only
Fosfomycin
singe dose therapy for uncomplicated UTI caused by e coli or enterococcus faecalis
AE = diarrhea, HA, vaginitis, nasuea
tetracyclines
tetracycline, doxycycline, minoocycline
MOA = inhibit protein synthesis, broad spectrum
use = infectious dx, acne, PUD, RA, mycoplasma pneumonia, lyme dx, anthrax, h pyylori
cant take w/ ca, iron, mg containing laxatives, antacids
AE = GI upset, bones & teeth, superinfection, hepatoxicity, renal toxicicty, photosensitivity
Macrolides
erythromycin, clarithromycin, azithromycin
MOA = inhibits protein synthesis, bacteriostatic can be bactericidal
active againt gram + and some gram -
use = whooping cough, chlamdia, m pneumonia, group A strep, if allgeric to penicillin
AE = GI upset, prolonged QT, cardiac death, superinfections, thrombophlebitits, transient hearring los
Clindamycin
MOA = inhibit protein synthesis, active against anaerobic bacteria (only certain ones outside CNS indicated)
can promote severe cdiff
AE = CDAD, hepatic toxicity, blood dyscrasias
Linezolid (Zyvox)
use = multi drug resistant gram + pathogens (VRE, MRSA)
MOA = inhibits protein synthesis, bacteriostatic
interacts w/ MAOIs
AE = NVD, HA
Telithromycin
use: Strep pneumonia
AE = severe liver injury, GI, visual changes, prlonged QT
Dalfopristin/Quinupristin
MOA = inhibits protein synthesis
use = VRE
AE = hepatotoxicity
CYP3A4 interaction
Chloramphenicol
MOA = inhibits protein synthesis
use = only life threatenning infection f nothing worked
AE = bone marrow depression, fatal aplastic anemia, gray syndrome, GI, peripheral neuropathy
aminoglycosides
Gemtamicin, tobramycin, amikacin, Neomycin, Kanamycin, Streptomycin, Paromomycin
narrow spectrum abx
bactericidal aerobic gram - bacilli
AE =nephrotoxicity, ototoxicity, neuromuscular blockade
Gemtamicin
used to treat infections caused by aeoribic gram - bacilli
pseudomonas aeruginosa
e coli
klebsiella
serratia
proteus mirabillis
AE = nephro & ototoxicity
sulfonamides
MOA = inhibit synthesis of folic acid
uses = UTI**, nocardiosis, chlamydia, UC, malaria
AE = stevens johnson syndrome, hematologic effects, kernicterus, renal damage from crystalluria
trimethoprim
MOA = inhibits dihydrofolate reductase -> supress DNA, RNA, protein synthesis
uses = acute and uncomplicated UTIs
AE = hematologic effects, hyperK, use in pregnancy and lactation
Trimethoprim/Sulfamethoxazole
MOA = inhibits bacterial folic acid synthesis powerfullly
use = UTI, OM, bronchitis, pneumonia, GI infection
AE = NV, rash, hyperK, stevens johnson, birth defects in first trimester
upper UTI
kidneys
acute pyelo
acute bacterial prostatitis
lower UTI
bladder & urethra
acute cystitis
acute urethral syndrome
organism that causes 80% uncomplicated community acquired UTIs
E coli
organism that causes most hosptial aquired UTIs
klebsiella
proteus
enterbacter
pseudomonas
staph
enterococci
e coli