Personality Disorders
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
19 Terms
personality disorders
Enduring pattern of inner experience and behaviour that deviates markedly from expectations. Changes in two or more of: cognition, affectivity, interpersonal functioning, impulse control
When certain traits are highly maladaptive, we might say that an individual has a personality disorder
Inflexibility is a significant aspect of personality
disordersMost of us can alter our behaviour when the context demands it
Compared to most people, individuals with
personality disorders have a small number of
traits that are particularly prominent and
inflexible
Inflexible and pervasive across a broad range of personal and social situations
Clinically significant distress or impairment
Stable and of long duration, with onset traced back to at least adolescence or early adulthood
Distress over personality traits is generally not a defining feature of personality disorders (they are usually egosyntonic), unlike virtually all other conditions (which are usually egodystonic)
Prevalence of all personality disorders combined is about 9% of the population
Quite a bit of comorbidity across personality disorders
Prevalence in clinical populations is very high (30-45%)
Prevalence and/or diagnosis of personality disorders varies by gender
Histrionic and borderline PD in women
Antisocial and narcissistic PD in men
Some temporary or short-term states can look like enduring personality disorders
personality disorders - etiology
Parent-child attachment is thought to affect an individual's later relationships and their way of approaching the world
Borderline personality disorder in particular has been associated with maltreatment, abuse, and extremely insecure attachment
Cognitive-behavioural explanations emphasize the role of early learning and maladaptive schemas
Some moderate evidence of genetic contributions
Personality is fairly highly heritable, but personality disorders appear to be much less so
clusters of personality disorders
Cluster A (Odd-Eccentric): Low Extroversion, Low Agreeableness
Paranoid personality disorder (0.4%)
Schizoid personality disorder (0.7%)
Schizotypal personality disorder (3%)
Cluster B (Dramatic-Emotional-Erratic): High Extroversion, Low Agreeableness, Low Conscientiousness, High Neuroticism
Anti-social personality disorder (2-3%)
Borderline personality disorder (1.7%)
Histrionic personality disorder (3%)
Narcissistic personality disorder (<1%?)
Cluster C (Anxious-Fearful): High Agreeableness, High Conscientiousness, High Neuroticism
Obsessive-compulsive personality disorder (1.7%)
Dependent personality disorder (1.7%)
Avoidant personality disorder (1.3%)
A - paranoid personality disorder
Pattern of suspiciousness and distrust, interprets other's motives as malevolent
Suspects that others are exploiting, harming, or deceiving
Preoccupied with unjustified doubts about loyalty or trustworthiness
Reluctant to confide in others, fears it will be used against him or her
Reads hidden demeaning or threatening meanings into benign comments or events
Persistently bears grudges
More readily perceives attacks upon character or reputation
Recurrent suspicions without justification about fidelity
Absence of frank delusions distinguishes paranoid PD from delusional disorder
Negative beliefs about others are more plausible (even if not supported by evidence)
A - Schizoid Personality Disorder
A pervasive pattern of detachment from social relationships and a restricted range of expression of emotions in interpersonal settings, as indicated by four or more of the following:
Neither desires nor enjoys close relationships, including
being part of a familyAlmost always chooses solitary activities
Has little, if any, interest in having s*xual experiences with
another personTakes pleasure in few, if any, activities
Lacks close friends or confidants other than first-degree
relativesAppears indifferent to the praise or criticism of others
Shows emotional coldness, detachment, or flattened
affectivity
Important differential diagnoses include psychosis, autism spectrum disorder, and social phobia
Often associated with significant educational/vocational under-achieving compared to intellectual ability, but very little emotional distress
A - Schizotypal Personality Disorder
A pervasive pattern of social and interpersonal deficits
marked by acute discomfort with, and reduced capacity for,
close relationships, as well as by cognitive or perceptual distortions and eccentricities of behavior, beginning by early
adulthood and present in a variety of contexts, as indicated
by five (or more) of the following:Ideas of reference (excluding delusions of reference)
Odd beliefs or magical thinking that influences behavior and is inconsistent with subcultural norms (e.g., superstitiousness,
belief in clairvoyance, telepathy, or "sixth sense"; in children and adolescents, bizarre fantasies or preoccupations)Unusual perceptual experiences, including bodily illusions
Odd thinking and speech (e.g., vague, circumstantial,
metaphorical, overelaborate, or stereotyped)Suspiciousness or paranoid ideation
Inappropriate or constricted affect
Behavior or appearance that is odd, eccentric, or peculiar
Lack of close friends or confidants other than first-degree
relativesExcessive social anxiety that does not diminish with
familiarity and tends to be associated with paranoid fears
rather than negative judgments about self
Schizotypal PD is listed in both the personality
disorders section and the psychosis section of
the DSM5
Cluster A vs Schizophrenia
Cluster A disorders can be prodromal (occur prior to the onset) to schizophrenia
A diagnosis of a Cluster A PD in an adolescent would be considered a risk factor for later conversion to psychosis
Distinguish between unusual thoughts and beliefs and delusions (bizarre or held with implausible conviction)
Duration and intensity
Cognitive impairment and grossly disorganized behaviour are not part of Cluster A PD’s
B - Antisocial Personality Disorder
There is a pervasive pattern of disregard for and violation of the rights of others occurring since age 15 years, as indicated by three or more of the following:
Failure to conform to social norms with respect to lawful
behaviors as indicated by repeatedly performing acts
that are grounds for arrestDeceitfulness, as indicated by repeated lying, use of
aliases, or conning others for personal profit or pleasureImpulsivity or failure to plan ahead
Irritability and aggressiveness, as indicated by repeated physical fights or assaults
Reckless disregard for safety of self or others
Consistent irresponsibility, as indicated by repeated failure to
sustain consistent work behavior or honor financial obligationsLack of remorse, as indicated by being indifferent to or
rationalizing having hurt, mistreated, or stolen from another
The individual is at least age 18 years
There is evidence of Conduct Disorder with onset before age
15 yearsAbout 3% in the general population (three times as common in men than women)
About 40% of the prison population
Higher fear threshold, low ability to learn from negative experiences
Antisocial behaviour can be an adaptive reaction to life circumstances
psychopathy
Avoidant Personality Disorder (APD) criteria includes observable
behaviours, but little about inner experience (emotions, thoughts, etc)Most psychopaths qualify for a diagnosis of APD, but most individuals with APD do not qualify as psychopaths
Psychopathy is not a DSM-5 diagnosis, but the term is widely used clinically and in research
Psychopathy Checklist - Revised (PCL-R): Glibness/superficial charm, grandiose sense of self-worth, pathological lying, cunning/manipulative, lack of remorse or guilt, shallow affect (genuine emotion is short-lived and egocentric), callous/lack of empathy, failure to accept responsibility for own actions, need for
stimulation/proneness to boredom, parasitic lifestyle, poor behavioral control, lack of realistic long-term goals, impulsivity, irresponsibility, juvenile delinquency, early behavior problems, revocation of conditional release, promiscuous s*xual
behavior, many short-term marital relationships, criminal versatility1% of the population
New research is suggesting that many or even most psychopaths
are not violent (although that is not to say they are harmless)There is no truth to the myth of the “brilliant” psychopath, IQ is completely independent of antisocial personality
treating APD and Psychopathy
Little motivation to make changes
Some evidence suggests that treatment succeeds in creating
better (less likely to be caught) psychopaths!
B - Borderline Personality disorder
"People with BPD are like people with third degree burns over 90% of their bodies. Lacking emotional skin, they feel agony at the slightest touch or movement." - Marsha Linehan
Instability reflects dysregulation of emotions, cognitions, sense of self, etc
Anxious-ambivalent or disorganized attachment style
Children desire safety, but inconsistent parenting results in beliefs that security is impossible
As adults, want intimacy but experience intense fear of abandonment
Idealization and devaluation often occurs with professionals involved in their care
Staff splitting
Dialectical behaviour therapy
An integrative approach involving aspects of CBT, mindfulness, and experiential therapy, often/mostly in group setting
Goal is emotional regulation and tolerance
Dialectics involve choices between opposing needs or desires, and recognition of dialectic aspect of emotions
Borderline Personality Disorder criteria
A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity as indicated by five or more of the following:
Frantic efforts to avoid real or imagined abandonment
Pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation
Markedly and persistently unstable self-image or sense of
selfImpulsivity in at least two areas that are potentially self-
damaging (e.g., spending, s*x, Substance Abuse, reckless
driving, binge eating)Recurrent suicidal behavior, gestures, or threats, or self-
mutilating behaviorAffective instability due to a marked reactivity of mood
(e.g., intense episodic dysphoria, irritability, or anxiety
usually lasting a few hours and only rarely more than a few
days)Chronic feelings of emptiness
Inappropriate, intense anger or difficulty controlling anger
(e.g., frequent displays of temper, constant anger, recurrent
physical fights)Transient, stress-related paranoid ideation or severe
dissociative symptoms
B - Histrionic Personality Disorder
A pervasive pattern of excessive emotionality and attention seeking, as indicated by five (or more) of the following:
Is uncomfortable in situations in which he or she is not the center of attention
Interaction with others is often characterized by inappropriate s*xually seductive or provocative behavior
Displays rapidly shifting and shallow expression of emotions
Consistently uses physical appearance to draw attention to self
Has a style of speech that is excessively impressionistic and lacking in detail
Shows self-dramatization, theatricality, and exaggerated expression of emotion
Is suggestible, i.e., easily influenced by others or circumstances
Considers relationships to be more intimate than they actually are
Often described as being the “life of the party”
Will do anything for attention, even things that reflect badly on themselves (unlike NPD)
Many people with borderline personality disorder also meet criteria for histrionic personality disorder
B - Narcissistic Personality Disorder criteria
A pervasive pattern of grandiosity (in fantasy or behavior), need for admiration, and lack of empathy, as indicated by five or more of the
following:Has a grandiose sense of self-importance (e.g., exaggerates achievements and talents, expects to be recognized as superior without commensurate achievements)
Is preoccupied with fantasies of unlimited success, power,
brilliance, beauty, or ideal loveBelieves that he or she is "special" and unique and can
only be understood by, or should associate with, other
special or high-status people (or institutions)requires excessive admiration
Has a sense of entitlement, i.e., unreasonable expectations of especially favorable treatment or automatic compliance with his or her expectations
Is interpersonally exploitative, i.e., takes advantage of
others to achieve his or her own endsLacks empathy: is unwilling to recognize or identify with the feelings and needs of others
Is often envious of others or believes that others are envious of him or her
Shows arrogant, haughty behaviors or attitudes
B - Narcissistic Personality Disorder
Characterized by an inflated sense of self-importance, a constant need for admiration, and a lack of empathy for others
Individuals often have a fragile self-esteem and may react negatively to criticism or perceived failures
Two psychoanalytic theories:
Kohut: Fixation on an earlier, normal stage of development, where other people are an extension of the self (selfobject)
Kernburg: Abnormal quality to early relationships makes individual relentlessly seek approval
There is some very early evidence of altered brain functioning in people with NPD
That could reflect a genetic or a learning etiology
Has a high overlap with borderline personality disorder and ASPD
C - Avoidant Personality Disorder
A pervasive pattern of social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation, beginning by early adulthood and present in a variety of contexts, as indicated by
four (or more) of the following:Avoids occupational activities that involve significant interpersonal contact, because of fears of criticism, disapproval, or rejection
Is unwilling to get involved with people unless certain of being liked
Shows restraint within intimate relationships because of the fear of being shamed or ridiculed
Is preoccupied with being criticized or rejected in social situations
Is inhibited in new interpersonal situations because of feelings of inadequacy
Views self as socially inept, personally unappealing, or inferior to others
Is unusually reluctant to take personal risks or to engage in any new activities because they may prove embarrassing
The DSM acknowledges the APD is essentially the same thing as social phobia
Anxious-avoidant childhood attachment style
C - Dependent Personality Disorder
A pervasive and excessive need to be taken care of that leads to submissive and clinging behavior and fears of separation, as indicated by five or more of the following:
Has difficulty making everyday decisions without an excessive amount of advice and reassurance from others
Needs others to assume responsibility for most major areas of his or her life
Has difficulty expressing disagreement with others because of fear of loss of support or approval
Has difficulty initiating projects or doing things on his or her own (because of a lack of self-confidence in judgment or
abilities rather than a lack of motivation or energy)Goes to excessive lengths to obtain nurturance and support
from others, to the point of volunteering to do things that are
unpleasantFeels uncomfortable or helpless when alone because of
exaggerated fears of being unable to care for himself or herselfUrgently seeks another relationship as a source of care and
support when a close relationship endsIs unrealistically preoccupied with fears of being left to take
care of himself or herself
Some similarities with depressive disorders (worthlessness, pessimism, self-dislike), and anxiety disorders
Panic disorder is common in DPD
Afraid of blame and/or rejection, and have learnt that deferring to others absolves them of responsibility
“Co-dependence” is not a DSM term, but captures a fairly similar construct
C - Obsessive-Compulsive Personality Disorder
A pervasive pattern of preoccupation with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency, as indicated by four or more of the following:
Is preoccupied with details, rules, lists, order, organization, or
schedules to the extent that the major point of the activity is lostShows perfectionism that interferes with task completion
Is excessively devoted to work and productivity to the exclusion of leisure activities and friendships (not accounted for by obvious economic necessity)
Is overconscientious, scrupulous, and inflexible about matters of morality, ethics, or values (not accounted for by cultural or religious identification)
Is unable to discard worn-out or worthless objects even when they have no sentimental value
Is reluctant to delegate tasks or to work with others unless they submit to exactly his or her way of doing things
Adopts a miserly spending style toward both self and others; money is viewed as something to be hoarded for future catastrophes
Shows rigidity and stubbornness
Often excessively deferential to authorities, and relationships seem
formal and seriousDistinguished from OCD by the absence of true obsessions and
compulsions, and presence of rigidity in most areas of life
personality disorders - treatment
Treatment prognosis is generally poor
Apart from BPD, there are no recognized empirically validated psychological treatments for any personality disorder
Acute distress is usually much less intense compared to other disorders, so motivation for treatment is low
Psychological treatment can take a very long time, and often focuses on learning new ways to respond (emotionally or behaviourally) in a close relationship
Some evidence that personality disorders are more manageable following pharmacological treatment to lessen anxiety, stress, depression, etc
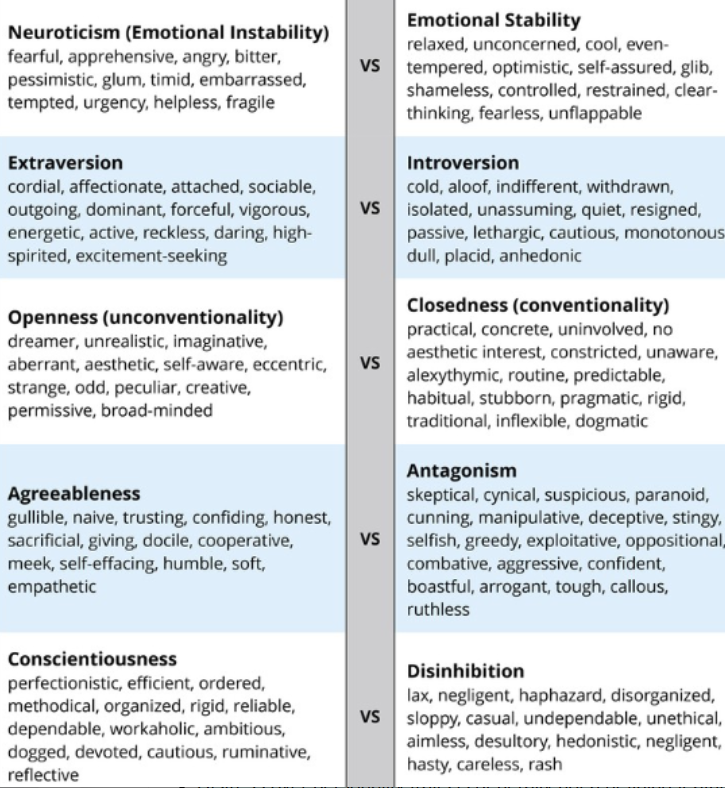
five traits (personality disorders)
Neuroticism (emotional instability) vs emotional stability
Extraversion vs introversion
Openness (unconventionality) vs closedness (conventionality)
Transparency and honesty in relationships vs privacy and personal boundaries
Agreeableness vs antagonism
Agreeableness – altruism, cooperation, and compassion, sensitive to the needs of others, helpful and cooperative
Antagonism – disagreeableness, skepticism, and competition, not cooperative, perceived as suspicious, manipulative and uncooperative
Conscientiousness vs disinhibition
Conscientiousness – responsible, organized, hard-working, goal-directed, and adhering to norms and rules
Disinhibition – the tendency to act impulsively, take risks, and fail to follow through with plans and goals; associated with a lack of self-control and social norms