Module 6 Diabetes & Glucose Regulation
1/74
Earn XP
Description and Tags
NUR1460C; Diabetes
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
75 Terms
Pancreatic exocrine function
Produces digestive enzymes:
• Amylase
• Lipase
• Protease
Pancreatic exocrine cells
Acini cells
-Secrete pancreatic juice
Pancreatic endocrine function
Islet of Langerhans:
-Alpha cells
-Beta cells
-Delta cells
Alpha cells
Release Glucagon
• Raises blood glucose
• Prevents hypoglycemia
Beta cells
Release Insulin
• Lowers blood glucose
• Moves glucose into cells
Delta cells
release somatostatin
Insulin function
• Decreases blood glucose
• Stimulates glucose uptake
• Promotes glycogen storage
• Inhibits ketone formation
-prevents hyperglycemia
Insulin production in the body
The body produces insulin in the beta cells of the pancreas.
This production is triggered by rising glucose levels in the bloodstream after eating
Glycogenesis
the metabolic process by which the body converts excess glucose molecules into glycogen for storage
-activated by insulin
Glycogenolysis
the biochemical process of breaking down stored glycogen into glucose
-immediate energy source
Gluconeogenesis
the metabolic process where the liver and kidneys synthesize new glucose from non-carbohydrate sources
Type 1 Diabetes
autoimmune destruction of beta cells
• Absolute insulin deficiency
• Requires lifelong insulin
• More common in younger patients
Glucagon
a peptide hormone produced by the pancreas (alpha cells) that raises blood glucose levels
• Raises blood glucose
• Stimulates glycogen breakdown
Type 2 Diabetes
a progressive disorder in which the person initially has insulin resistance that progresses to pancreatic beta-cell dysfunction
-insulin resistance- the body's cells do not respond properly to insulin causing pancreas to make more insulin (hyperinsulinemia)
-beta-cell failure- the pancreas cannot produce enough insulin to overcome this resistance
Latent Autoimmune Diabetes of Adult Onset (LADA)
often called "Type 1.5 diabetes"—is a form of autoimmune diabetes that begins in adulthood
-immune system attacks insulin-producing cells, but the damage happens much more slowly, so insulin isn't required right away
• Initially may not require insulin
-”LATEnt” to remember
Normal fasting glucose
70–100 mg/dL
Prediabetic glucose levels
100–125 mg/dL
Diabetic glucose levels
Diabetes
≥126 mg/dL (two occasions)
Random Glucose
≥200 mg/dL + symptoms
Hemoglobin A1C
Normal: 4–6%
Diabetes: ≥6.5%
*Remember: A1C reflects approximately 3 months of glucose control
Metabolic syndrome
the simultaneous presence of metabolic factors known to increase risk for developing Type 2 DM
Obesity
Coronary heart disease
Dyslipidemia (high LDL & low HDL)
Hypertension
Microalbuminuria (protein in the urine)
Increased risk for thrombotic (blood clotting) events
Primary diabetes prevention
balanced diet
exercise
weight control
Secondary diabetes prevention
Lab tests:
-hemoglobin A1C
-cholesterol
-microalbuminuria
Screening to detect complication: BP, dental care, foot care, eye exams
Hyperglycemia (“High & Dry”)
High blood glucose (125-180+ mg/dL)
-result of insufficient insulin production or secretion, excessive counter-regulatory hormones secretion and deficient hormone signaling
-body burning fat instead of using glucose for energy
-leads to metabolic acidosis or DKA
-hemoconcentration, hypovolemia, hyperviscosity, hypoperfusion, hypoxia
Hyperglycemia S/S
polyuria
polydipsia
polyphagia
• Weight loss
• Fatigue
• Blurred vision
• Recurrent infections
• Numbness
Hyperglycemia pathophysiology
-insulin absent > fat breakdown > ketones > metabolic acidosis
signs: Kussmaul respirations, fruity breath, dehydration
Hyperglycemia complications
Hot dry flushed skin, the 3 P’s, fruity breath – Kussmaul’s Respiration
Restless, drowsy- unconsciousness
Treatment: check BG
IV fluids, Insulin infusion
Continue to monitor BG
Basic Metabolic Panel (BMP) for Electrolytes: K+ (may be below 3.5) Supplementation of K+ may be needed
Hyperglycemia treatment/interventions
-Insulin therapy
-Isotonic fluids
-Blood glucose tracking
-Assess for complications - altered mental status, fruity breath, Kussmaul respirations, and severe dehydration
Hypoglycemia
low blood glucose levels (70 mg/dL)
-typically occurs as a result of insufficient nutritional intake
-adverse reaction to medications
-excessive exercise, and/or a consequence of disease states
Levels of hypoglycemia
-Level 1 hypoglycemia is a glucose less than 70 mg/dL but greater than or equal to 54 mg/dL
-Level 2 hypoglycemia is less than 54 mg/dL.
-Level 3 hypoglycemia is any event requiring external assistance because of mental or physical alterations.
Hypoglycemia S/S
“Low is Slow”
• Irritability
• Confusion
• Tremors
• Fatigue
• Seizures
• LOC changes
• Gastroparesis -delay in gastric emptying
Hypoglycemia treatment/interventions
15g carbohydrates (juice, crackers, glucose tablets)
reassess in 15 minutes
severe patients (< 30 mg/dL):
-glucagon IM/SQ- repeating the dose in 10 minutes if the patient remains unconscious; notify the PCP immediately
-25 to 50 mL of D50W via IV push at a rate of 10 mL/min
Hypoglycemia complications
Confusion, irritability, tremor, sweating
Hypothermia, seizures
Coma and death will occur if not treated
Treatment – check BG
IF ALERT AND ABLE TO SWALLOW
Oral forms of concentrated glucose
Orange juice – may repeat if BG still low
If NOT ALERT
5% dextrose in water (D50W)
Glucagon IV or IM
Blood-free glucose monitoring
FreeStyle Libre (continuous glucose monitoring system)
-detects highs & lows
-have to reapply a new sensor to your arm every 14 days
Continuous Subcutaneous Infusion of Insulin (CSII)
Continuous Subcutaneous Infusion of Insulin (CSII)
-An insulin pump administers insulin on a continual basis. Rapid Acting Insulin Used
Patient Education:
-Hand washing Use aseptic technique when cleaning site
-The cannula should be changed every 1-2 days.
-Ketoacidosis may occur because of infection, obstruction, or mechanical pump problems.
-If BG levels ↑than 300 mg/dL – Need for Ketone testing
Rapid-acting Insulin
-Blocks hepatic production of glucose
-Tx: Type I & Type 2 Diabetes
Aspart (Novolog)- peak 1 hour
Lispro (Humalog)- peal 40-50 minutes
-onset: 15 minutes
-durations: 3-5 hours
Short-acting Insulin
Regular insulin (Humulin R, Novolin R)
Tx: Type I & Type II Diabetes, Acute Hyperglycemia, DKA, Severe Hyperkalemia, Insulin in D5W
-The only type of insulin that should be given intravenously is regular human insulin (can be SQ too)
-onset: 0.5-1 hour
-peak: 2-3 hours
-duration: 4-6 hours
Intermediate-acting Insulin
Isophane insulin (NPH)
Tx: Type I & Type II Diabetes
-onset: 2-4 hours
-peak: 6-8 hours
-duration: 12-16 hours
Long-acting Insulin
Glargine (Lantus) & Detemir (Levemir)
-Tx: Type I & Type II Diabetes
-onset: 2 hours
-peak: no peak
-duration: 24 hours
-should be drawn up in a separate syringe*
Single dosing
Intermediate or long acting Insulin
-Some Type II DM patients once-daily for basal coverage
-Oral antidiabetic to stimulate Insulin secretion
Multiple Insulins
a combination of short/intermediate based on blood glucose levels pre and postprandial (before and after meals)
Intensified (insulin) Regimes
Rapid/short/intermediate/long acting – the aim is to attain the target range
-Blood glucose levels will determine Insulin dosage-Sliding-Scale
Insulin injection sites
Subcutaneous injection
-45° ANGLE FOR OLDER FRAIL PATIENTS
-90° ANGLE FOR YOUNGER AND THOSE THAT ARE OVERWEIGHT
-Rotation of injection sites to prevent a decrease in absorption and lipodystrophy of the SQ Tissue
Importance of Insulin Peak times
-Peak time is the period when a medication has its strongest effect
-It’s essential to know the peak time of the insulin so that one can predict how much and when a person should eat to keep the blood sugar constant.
-Snacks should be ingested around peak times to avoid hypoglycemia
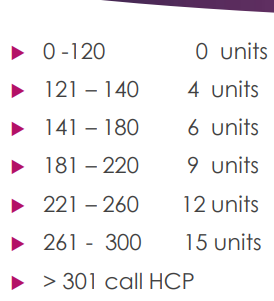
Insulin Sliding Scale
a reactive dosing method where short-acting or rapid-acting insulin is administered in increasing amounts based on pre-meal or bedtime blood sugar levels
-Basically, add ordered insulin and units to administer based on pts blood glucose levels (scheduled insulin + correction insulin)
Metformin (Glucophage)
-Biguanides Oral - Antidiabetic
-Tx: Type II Diabetes
-Blocks glucose production from the liver and prevents glucose reabsorption in the intestines, & increases insulin sensitivity
-It DOES NOT cause HYPOglycemia
-GI upset, and bloating can occur, take with food to lessen symptoms
-Avoid alcohol (EtOH), may induce Latic Acidosis (do not take with kidney disease*)
Contrast & Metformin
-Hold metformin for 48 hours before procedures that require iodine-containing contrast agents because these agents cause renal failure in patients treated with metformin.
-Resume medication no earlier than 48 hours following the procedures, after renal function is confirmed to have returned to baseline.
Micronase (Glyburide)
Sulfonylurea
-Tx: Type II Diabetes
-Stimulates the pancreas to produce more insulin
-Longer duration (up to 24 hours), not recommended for adults 65+
-Take before a meal can decrease the potential for hypoglycemia
-Severe effects for those with liver/renal disease
-Interacts with many medications
Glipizide (Glucotrol)
Sulfonylurea
-Tx: Type II Diabetes
-stimulates insulin release
-shorter duration (12-24 hours), lower risk, generally safe for 65+ adults
-risk: hypoglycemia
Injectables:
-Exenatide (Bydureon/ Byetta)
-Dulaglutide (Trulicity)
-Liraglutide (Victoza)
-Semaglutide (Ozempic)
Incretin Mimetics (GLP-1 Agonists) Antidiabetic Injectables
-Tx: Type II Diabetes
-stimulate glucose-dependent insulin secretion, inhibit glucagon release, slow gastric emptying, and promote satiety
-Once a week subq. injectables
-Not a replacement for insulin
-Risk: hypoglycemia, weight loss, delay gastric emptying
Antidiabetic Drugs Patient Education
-Antidiabetic drugs are not a substitute for dietary modification and exercise.
-Nutritional considerations
-Exercise
-All patients with DM should monitor blood glucose levels regularly
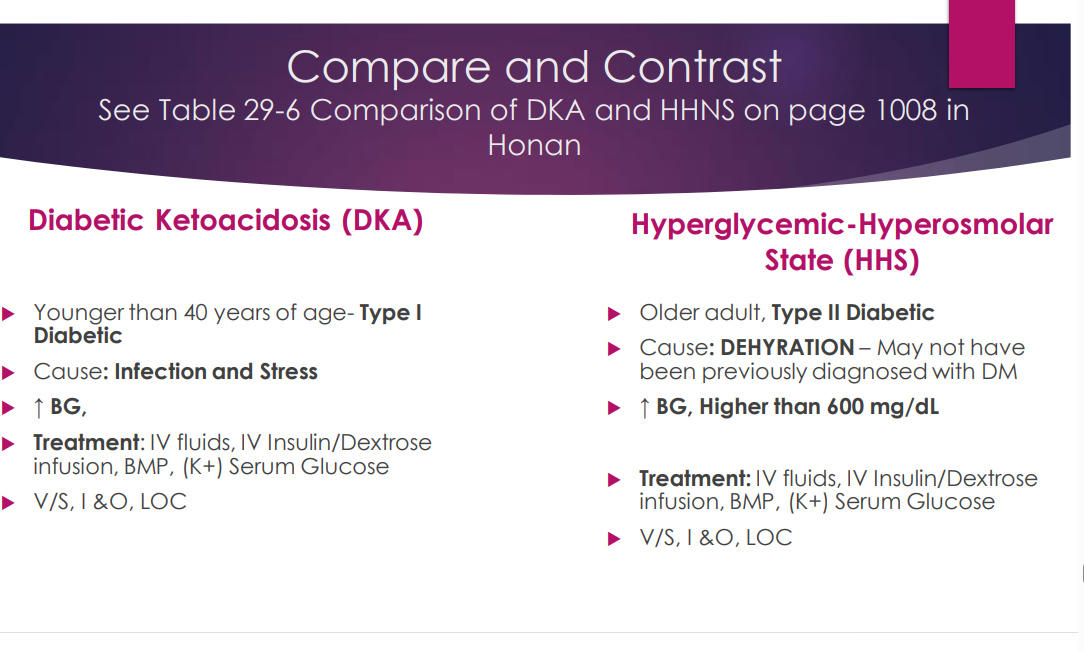
Diabetic Ketoacidosis (DKA)
-The combination of insulin deficiency and an increase in hormone release that leads to increased liver and kidney glucose production and decreased glucose use in peripheral tissues.
-uncontrolled hyperglycemia, metabolic acidosis, and increased production of ketones
-DKA occurs in Type I DM, but it can occur in Type II DM under severe stress.
-The most common precipitating factor for DKA is INFECTION
S/S of Diabetic Ketoacidosis (DKA)
Polyuria, Polydipsia, Polyphagia
-Fruity breath
-Kussmaul respirations
-Weakness
-Confusion
-Abdominal pain
-Hypokalemia (after treatment starts)
DKA treatment
-IV fluids FIRST
-Regular insulin IV in D5W
-Frequent monitoring of BG
-Monitor anion gap (normal 7-9 mEq/L), if high indicates metabolic acidosis
-Common cause of death is Hypokalemia**
-Monitor ECG
Hyperglycemia-Hyperosmolar State (HHS)
a life-threatening complication of diabetes (mostly type 2; older adults) characterized by extremely high blood sugar, severe dehydration, and concentrated blood (high osmolality)
-ketone levels are absent or low compared to DKA
-BG level may exceed 600mg/dL
-blood osmolarity may exceed 320 mOsm/kg
-”High high sugar” (HHS) to remember
HHS in Older Adults
-Most common cause is DEHYDRATION
-Kidney impairment in HHS allows for extremely high blood glucose levels.
-Many are unaware they have the disease.
-Mortality rates in older patients are high.
-The onset of HHS is slow and may not be recognized.
HHS Treatment
• IV fluids
• Insulin
• Electrolyte correction (K+)
-Important to continually monitor the patient being managed for HHS state to recognize status changes
-Assess the patient hourly for signs of cerebral edema with abrupt changes in mental status, abnormal neurologic signs, and coma
-Notice changes in LOC, as well as pupil size, shape, or reaction, and seizures. If any of these signs are present notify the care provider immediately
DKA & HHS Comparison
DKA occurs in < 40 yr. old Type 1 Diabetic
HHS occurs in older adults Type 2 Diabetic
DKA is caused by infection & stress
HHS is caused by dehydration
HHS blood glucose are higher compared to DKA (600mg/dL)
DKA has high ketones while HHS has high serum osmolality
Dawn Phenomenon
Early AM hyperglycemia
-caused by natural early-morning hormone release, not hypoglycemia like Somogyi
Tx: Increase evening insulin
Somogyi Effect
a controversial diabetes concept suggesting that an episode of low blood sugar overnight triggers the body to overcompensate, causing high blood sugar in the morning
-”rebound hyperglycemia”- rebound from nighttime hypoglycemia
-Tx: bedtime snack, adjust insulin, exercise program
Macrovascular Diabetic Complications (macroangiopathy)
CAD
Stroke
PVD
• Blood vessel walls thicken, sclerosis, and become occluded by plaque that adheres to the vessel walls
• Leads to coronary artery disease, cerebrovascular disease, and peripheral vascular disease
• Focus of management is aggressive modification and reduction of risk factors
-Think Brain, Heart, Extremities
Microvascular Diabetic Complications
Retinopathy - vision loss
Nephropathy - kidney disease
Neuropathy - Peripheral neuropathy (Gabapentin med)
Think Eyes, Kidneys, Nerves
Cardiovascular Autonomic Neuropathy
affects sympathetic and parasympathetic nerves of the heart and blood vessels.
-This leads to orthostatic (postural) hypotension, resting tachycardia, exercise intolerance, silent ischemia
Autonomic Neuropathy
can also affect the GI system (gastroesophageal reflux, delayed gastric emptying and gastric retention, early satiety, heartburn) nausea, vomiting, constipation and diarrhea, and anorexia
Peripheral Neuropathy
chronically high blood glucose levels- numbness, loss of sensation, pain in feet and legs or hands
-Medication - *Gabapentin (Neurontin)*
Gabapentin (Neurontin)
anticonvulsant and nerve pain medication for diabetic peripheral neuropathy
Tx: Seizures, Neuropathic Pain, Migraines, Post-herpetic neuralgia- following Shingles, Fibromyalgia
-not recommended for pts with COPD or other respiratory issues
Foot Care for Diabetics
Shoes on at all times.
Properly fitted shoes.
Shop late in the day
Inspect feet daily.
Keep feet and skin moist to prevent cracks.
Apply lotion to feet except between toes.
Seamless hose and stockings
Toenails clipped by a podiatrist (recommended).
-Neuropathy main cause of diabetic ulcer
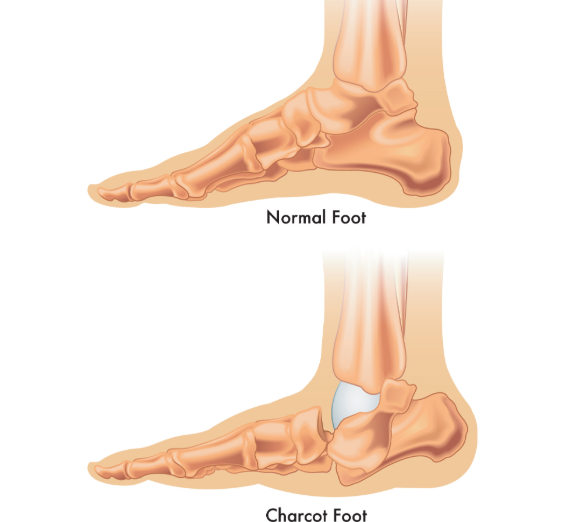
Charcot foot
a type of diabetic foot deformity with any abnormalities, often including a hallux valgus (turning inward of the great toe).
Walking collapses the arch, shortens the foot, and gives the foot a “rocker bottom” shape.
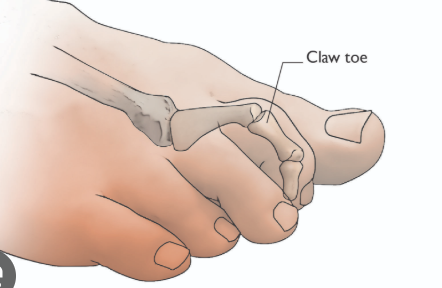
Claw toe
-Thinning or shifting of the fat pad under the metatarsal heads decreases cushioning and increases areas of pressure.
-In claw toe deformity, toes are hyperextended and increase pressure on the metatarsal heads (ball of the foot).
-These changes predispose the patient to callus formation, ulceration, and infection
Diabetes Surgery
Risks:
• Hyperglycemia
• Infection
• Delayed healing
Monitor:
• BG
• Skin
• Hydration
• Stress response
Diabetic Teaching
-Patient must be willing to focus on reducing modifiable risk factors such as smoking cessation, diet, exercise, blood pressure control, maintaining prescribed aspirin use – maintain prescribed lipid-lowering drug therapy.
-The patient must be able to plan for periodic evaluation of blood glucose control by the PCP, as well as periodic dental and eye examinations.
-The patient must be able to integrate the demands of diabetes into daily and recreational schedules while keeping blood glucose stable.
-Encourage all patients to participate regularly in exercise or physical activity appropriate to their health status for better blood glucose regulation
Diabetes Insipidus
Caused by a deficiency of—or resistance to—antidiuretic hormone (ADH), also called vasopressin
-severe polyuria (very diluted urine)
-polydipsia
-dehydration
-increased electrolyte levels (hypernatremia)
-normal blood sugar
-Tx: Vasopressin
Vasopressin (synthetic ADH)
Tx for Diabetes Insipidus
-Close monitor of vital signs, ECG, I&O
Interventions for Diabetes Insipidus
Drug therapy with Desmopressin
Urine output can be lowered with a low-salt, low-to-normal protein diet and diuretics.
Restricting sodium intake to less than 2.3 g/day and reducing protein intake to less 1.0mg/kg daily diminishes urine output.
Thiazide diuretic induces mild volume depletion; even a weight loss of 1 to 1.5 kg can reduce urine output significantly.
Measure fluid intake and output
Check urine specific gravity
Record the patient’s daily weight.
Urge the patient to drink fluid in an amount equal to urine output
Ensure the patency of the access catheter and accurately monitor the amount infused intravenously hourly
DI vs. SIADH
SIADH is the excessive retention of water, while DI is the excessive loss of water
SIADH think LOW- oliguria, hyponatremia, low blood osmolality (diluted)
DI think HIGH- polyuria, hypernatremia, high blood osmolality (concentrated)
Desmopressin (DDAVP)
synthetic hormone that mimics vasopressin; signals kidneys to reabsorb water, thus reducing urine production (water regulation)
-Tx for Diabetes Insipidus
-monitor sodium levels (hyponatremia), I&O, & neuro changes
-daily weights
-restrict fluid intake to prevent water intoxication