Looks like no one added any tags here yet for you.
What two categories can risk factors be divided into?
systemic/local
What are systemic risk factors?
- affect multiple organs
- systems
- entire body
e.g. smoking, bleeding disorders
What are local risk factors?
affects a specific area in the body
e.g. inadequate OH or local inflammatory processes
Contraindications can be medical, psychological, or social. Contraindications for implant therapy can be divided into...?
relative or absolute
What is a relative contraindication?
any medical reason, condition, clinical symptom, or circumstance that may or may not prevent implant therapy; it increases the risk of complications
What is an absolute contraindication?
preclude implant therapy
any medical reason, condition, clinical symptom, or circumstance that is so compelling or that carries such a high risk that under no reasonable circumstance is implant therapy advisable
Examples of systemic RF's include:
- immunodeficiency (causes: obesity, alcoholism, drug use, malnutrition)
- immunosuppressive drugs
- bleeding disorders
- chemotherapy
- irradiated bone
- osteoporosis
- poorly controlled diabetes
- history of heavy smoking
What are examples of immunosuppressive drugs?
- long-term high-dose corticosteroids (e.g. RA pts)
> red bone dentistry, immunosuppression
> may compromise osseointegration & peri-implant healing
> suppression of adrenal cortex -> steroid supplementation during surgery may be needed
- organ transplant pts -> inc risk post-op infections
What are oral side effects of chemotherapy?
- xerostomia
- taste changes
- sensitivity
- gingival bleeding
- ulcerations
- mucositis
- infections (herpetic, bacterial, fungal)
How may radiotherapy affect implants?
- scientific evidence to show a higher failure rate of osseointegrated implants in irradiated pts
- radiotherapy may induce vascular fibrosis and thrombosis, withw/subsequent tissue breakdown & development of chronic nonhealing wounds
- immediate risk is ORN
- adequate waiting period after radiotherapy is rec; alt, a series of hyperbaric oxygen tx's can be prescribed before implant surgery
How does osteoporosis and bisphosphonates affect implants?
- osteoporotic pts are at higher risk of perio disease, & pts w/ perio are at higher risk of ONJ
- periodontal intervention & disease prev are imperative
- may be tx w/ antiresorptive meds, typically oral bisphosphonates or yearly IV bisphosphonates.
- adversely affect the ability of the bone to remodel itself, so there is a small risk of compromised bone healing following implant placement if the pt has been in long-term tx w. oral bisphos
How may diabetes affect implants?
- general oral effects incl xerostomia, increased levels of salivary glucose, increased incidence of caries & periodontal disease
- no proven association v/t poor glycemic control & implant failure
- although pts w/ poor glycemic control have been associated w/ an increased susceptibility to postop infections
How may smoking affect implants?
- implant failure rate in smokers is x2 that of non-smokers
- associated w/:
> more marginal BL after implant placement
> higher incidence of peri-implantitis
> lower success for bone grafts
- adversely affects long-term dental implant prognosis
Examples of local RF's include:
- poor OH
- periodontal disease
- oral mucosal diseases
- bruxism
What is a general prerequisite for implant placement?
adequate OH
> substantial evidence that poor OH & microbial biofilms are associated w/ peri-implant dx & implant loss
How may periodontal disease affect implants?
- when teeth affected by PD are lost, remaining bone height is reduced: may limit the available bone height for the placement of implant
- implants replacing teeth lost to chronic perio may have: lower survival rates, more biological complications
- untx PD increases risk of peri-implant dx: evidence that peruo pockets might serve as reservoirs of pathogens that can be transmitted
Give examples of potential diseases which affect the oral mucosa:
- Sjogren
- epidermolysis bullosa
- LP
> medical consulation req prior to implant placement
> long-term follow-up essential
> pts ability to maintain OH may be compromised
How may bruxism affect implants?
- RF for excessive loading of implants & prostheses
- increased risk for mechanical & technical complications:
> screw loosening
> srew/abutment fracture
> prosthesis fracture
A relative contraindication in one patient may be considered to be an absolute contraindication in another patient if what exists?
other conditions or RFs
Give examples of relative contraindications:
- insufficient bone vol
- periodontitis
- RR
- local infection
- drug/alcohol abuse
- psychological disorders
- young age
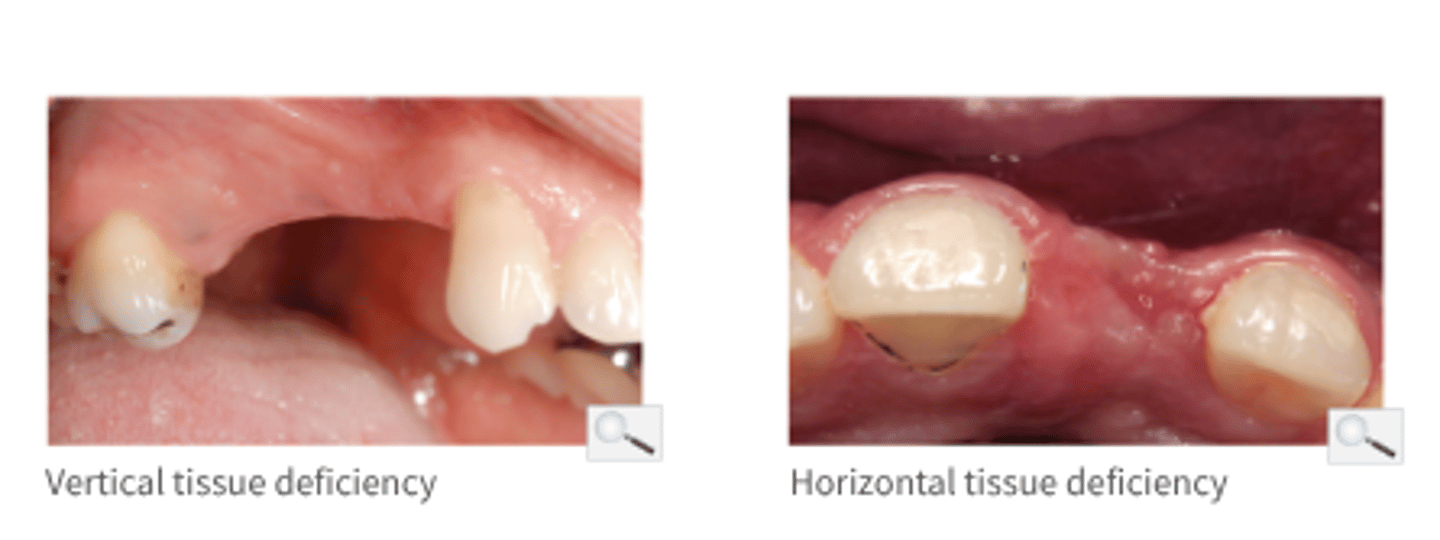
Why is insufficient bone volume considered to be a relative contraindication to implant therapy?
Many augmentation techniques have been developed for:
- prior (stages) or simultaneous bone grafting
- vertical or horizontal ridge augmentation
As a rule retained roots should be removed prior to implant placement. In what cases would be an exception?
- where the gingival & bone health around the root are sound
- root removal at the time of implant placement can be considered
How may local infections affect implants?
- infection may compromise osseointegration of the implant
- furthermore, chronic endo infections result in inflammatory bone resorption, & after healing the residual bone vol may be insuff to house an implant
- teeth adj to the planned implant site should also be assessed for endo pathology & other infections that could jeopardise
How may alcohol and drug abuse have an effect on the success of implant therapy?
- likelihood of poor nutritional intake
- possible red ability to heal
- interference w/ prescribed pre & pos-op meds
- poor complaince w/ post-op & hygiene instructions
Why might it be important to carry out pre-treatment evaluation of compliance in patients living with mental or psychological conditions?
- the dentist may be confronted with behaviours that may interfere with the safe & efficient delivery of implant therapy
- may also pose problems with compliance
What role does age play to implant therapy?
- not be placed until growth/development complete
- implants do not erupt during dentoalveolar development
- if placed in immature pts, can become infraoccluded
- consider dental age & skeletal amturation
- adv age itself isn't a contraindication
Give examples of absolute contraindications to implant therapy:
- ASA-5/6
- IV bisphosphonates
- high-dose H/N radiation
- active chemotherapy
- high-dose immunosuppressives
- serious systemic dx
- allergy to implant materials
- lack of compliance
What osseous disorders is an absolute contraindication to implant therapy?
osteomalacia (softening of bones), OI
Why are patients currently being treated with high-dose intravenous bisphosphonates not candidates for implant therapy?
risk of developing MRONJ among pts exposed to antiresorptive drugs for dental implant placement is unknown but considered to be comparable to the risk associated w/ tooth extraction