Series 1 Form B Part 3
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
A physical therapist is examining a patient and finds that when the patient's feet are together in standing position, the left iliac crest appears lower than the right. However, when the feet are spread apart, the iliac crests are level. This discrepancy is MOST likely caused by tightness of which of the following muscle groups?
1.Right hip abductors
2.Left hip adductors
3.Right hip adductors
4.Left hip abductors
4,4
1. Tight right hip abductors would not pull the left hip downward; they would tend to raise the left iliac crest.
2. With feet together, there is slack on the hip adductors, so there should not be any effect on the iliac crest height.
3. With feet together, there is slack on the hip adductors, so there should not be any effect on the iliac crest height.
4. The iliac crests are level with the hips abducted (feet spread apart), but the right iliac crest is higher when the hips are adducted (feet together). Tightness in the left hip abductors would be the most likely cause, because the tight left hip abductors would be pulling the left hip downward
A patient with a C7 spinal cord injury wants to perform transfers using the technique shown in the photograph. Which of the following resisted exercises would be MOST appropriate to accomplish this goal?
1.Scapular protraction
2.Elbow flexion
3.Shoulder internal rotation
4.Scapular elevation
1,1
1. During the transfer, protraction and depression of the scapulae increase the height of the lift to clear the buttocks
2. The elbows should be locked into extension either through activity of the triceps or positioning the shoulders in external rotation
3. internal rotation of the shoulders is not needed to maintain elbow extension.
4. The scapulae should be depressed to increase the height of the lift

A patient who had a myocardial infarction is in a cardiac rehabilitation program. Which of the following changes should cause the physical therapist to stop the exercise session?
1.An increase in systolic blood pressure of 10 mm Hg
2.A decrease in diastolic blood pressure of 5 mm Hg
3.An increase in the respiratory rate of 5 breaths/minute
4.A decrease in the heart rate of 15 bpm
4,4
1. A linear increase in systolic blood pressure is expected with increased activity.
2. A diastolic blood pressure increase or decrease greater than 10 mm Hg would be an abnormal finding.
3. An increase in respiration is an expected response to an increase in activity level.
4. A drop in heart rate greater than 10 bpm is an abnormal response to exercise and should cause the physical therapist to halt the activity.
A physical therapist is treating a patient who has Parkinson disease. The patient expresses concern about declining health and a poor prognosis. Which of the following is the MOST appropriate response for the therapist to make?
1.Offer resources on support groups.
2.Refer the patient to a psychiatrist.
3.Have the patient speak with another patient who has Parkinson disease.
4.Tell the patient that physical therapy will prevent disease progression.
1,1
1. Offering resources, including talking with many other patients, will allow choice and keep the locus of control within the patient
2. A psychiatrist could be among the resources that may be used by the patient, but there is no indication in the scenario of a need for psychiatric services. Signs of psychiatric toxicity related to Parkinson medications include visual hallucinations, delusions, and paranoia.
3. Offering support groups would be more appropriate than having the patient speak to another patient. A support group would give the patient more active role in the decision-making process and provide the patient with multiple resources and targeted information than a single individual may be able to provide.
4. The physical therapist should not give misleading statements. The patient should receive accurate information about disease progression.
A patient has an acute grade I sprain of the acromioclavicular joint. Which of the following activities would be MOST painful for the patient to perform?
1.Reaching behind the back to tuck in a shirt
2.Reaching across the chest and scratching the opposite shoulder with the hand
3.Opening a car door
4.Using both hands to lift a 10-lb (4.5-kg) bag of groceries from the floor to a waist-high table
1,2
1. Reaching behind the back to tuck in a shirt would stress the rotator cuff muscle/tendons and not the acromioclavicular joint.
2. Reaching across the chest and scratching the opposite shoulder with the hand is the correct response since active and passive movements in the extreme ranges of motion, especially elevation of the shoulder above 90° and horizontal adduction, reproduce acromioclavicular joint pain in patients who have sprains or degenerative joint disease.
3. Opening a car door requires strength of the elbow flexors and shoulder extensors/scapular retractors and does not stress the acromioclavicular joint.
4. Using both hands to lift a 10-lb (4.5-kg) bag of groceries from the floor to a waist-high table requires strength in the elbow flexors and does not stress the acromioclavicular joint.
A patient has radicular pain due to C4-C5 intervertebral foramen stenosis on the right side. In addition to cervical flexion, which of the following combinations of cervical motions is likely to provide the MOST pain relief for the patient?
1.Right side bending and left rotation
2.Right side bending and right rotation
3.Left side bending and right rotation
4.Left side bending and left rotation
1,4
1. Performing right side bending would decrease the size of the intervertebral foramen
2. Performing right side bending, although limited by coupled left side bending (induced by performing left rotation), still reduces the size of the intervertebral foramen, compared to performing left side bending and left rotation
3. In the mid cervical region the coupling motions of side bending and rotation occur in an ipsilateral fashion. Therefore, performing right rotation would cause a decrease in the area of the intervertebral foramen by inducing coupled right side bending. The induced right side bending will limit the amount of the intervertebral foramen opening on the right side at the affected segment.
4. The area of the intervertebral foramen on the right increases with left side bending and left rotation
Which of the following variables TYPICALLY increases during the aging process in older adults?
1.Vital capacity
2.Skin elasticity
3.Glucose tolerance
4.Resting blood pressure
4,4
1. Vital capacity decreases with aging.
2. Elasticity decreases with aging.
3. Glucose tolerance decreases with aging.
4. Resting blood pressure increases with advancing age.
Which of the following is consistent with pain of musculoskeletal origin?
1.Pain decreases with rest.
2.Pain is reduced by constant pressure.
3.Pain follows a migratory pattern.
4.Pain awakens the patient at night.
1,1
1. Musculoskeletal pain is often relieved by a change in position or by rest.
2. Pressure may increase musculoskeletal pain but may decrease pleural friction/irritation and decrease visceral pain. Local tenderness to pain is present in musculoskeletal conditions.
3. Migratory pain is pain of a systemic nature.
4. Pain that awakens a patient at night is a symptom of systemic origin.
A physical therapist is performing a supine hamstring stretch on a patient who has a T5 level spinal cord injury. The patient describes a pounding sensation in the ear. What should the therapist do FIRST?
1.Roll the patient to the left side.
2.Take the patient's blood pressure.
3.Bring the patient to an upright position.
4.Notify the patient's physician for immediate medical attention.
2,3
1. A pounding sensation in the ear in a patient with a spinal cord injury above the level of T6 is indicative of autonomic dysreflexia. With autonomic dysreflexia, the patient's blood pressure will be elevated and the patient should be brought to an upright position to lower the blood pressure. Rolling the patient to the left side would not lower the blood pressure.
2. A pounding sensation in the ear in a patient with a spinal cord injury above the level of T6 is indicative of autonomic dysreflexia. With autonomic dysreflexia, the patient's blood pressure will be elevated and the patient should be brought to an upright position to lower the blood pressure.
3. A pounding sensation in the ear in a patient with a spinal cord injury above the level of T6 is indicative of autonomic dysreflexia. With autonomic dysreflexia, the patient's blood pressure will be elevated and the patient should be brought to an upright position to lower the blood pressure.
4. A pounding sensation in the ear in a patient with a spinal cord injury above the level of T6 is indicative of autonomic dysreflexia. Although autonomic dysreflexia can be a life-threatening condition, notifying the physician would not be the most immediate action to take and would be the appropriate action only if the blood pressure cannot be reduced by other means.
What reaction is MOST likely being assessed in the photograph?
1.Moro reflex
2.Startle reflex
3.Landau reflex
4.Positive support reflex
4,3
1. The Moro reflex is elicited by supporting the infant in a supine position, allowing the head to gently drop posteriorly in relation to the trunk, and assessing the response at the arms
2. The startle reflex is elicited by making a sudden loud or harsh noise and results in sudden extension or abduction of the upper extremities and crying
3. The Landau reflex/reaction is elicited by supporting the infant horizontally in prone position. The expected response is that the infant will extend the neck and trunk.
4. The positive support reflex/reaction is elicited by supporting the infant vertically with contact of the feet to a surface and assessing the lower extremity response
A patient has completed a 2-week course of comprehensive physical therapy for treatment of constant right shoulder and scapular pain and has not had any improvement. The patient states that change in position does not alter the pain intensity. The physical therapist should NEXT ask the patient about:
1.persistent sore throat.
2.difficulty swallowing food.
3.burning with urination.
4.intolerance to fatty foods.
4,4
1. A persistent sore throat is not a symptom manifested in acute cholecystitis
2. Dysphagia may be caused by esophageal dysfunction, which typically refers pain to the middle of the back not to the right shoulder or scapula
3. Dysuria is associated with renal/urologic dysfunction. Such dysfunction may refer to the costovertebral areas, low back, and/or groin
4. The signs and symptoms of acute cholecystitis may include pain that radiates to the right shoulder, right scapula, or interscapular area. In patients with renal calculi, there may be a history of past episodes of biliary colic and fatty food intolerance. The patient may also report nausea, vomiting, fever, and right upper quadrant pain
A physical therapist can perform a quick, nonspecific functional assessment of shoulder abduction and lateral (external) rotation by instructing the patient to use the arm being tested to reach:
1.across the chest and touch the contralateral shoulder.
2.overhead and touch the superior medial border of the contralateral scapula.
3.up and touch the ipsilateral shoulder.
4.behind the back and touch the inferior angle of the contralateral scapula.
2,2
1. Reaching across the chest and touching the contralateral shoulder may be used to assess shoulder horizontal adduction and flexion of the shoulder.
2. Reaching overhead and touching the superior medial border of the contralateral scapula requires normal shoulder abduction and external (lateral) rotation.
3. Reaching up and touching the ipsilateral shoulder primarily measures elbow flexion.
4. Reaching behind the back and touching the inferior angle of the contralateral scapula measures extension and internal (medial) rotation of the shoulder.
Which of the following ankle-brachial index values suggests arterial calcification?
1.0.6
2.0.9
3.1.0
4.1.4
1,4
1. An ankle-brachial index of 0.6 is suggestive of moderate peripheral artery disease. This result would warrant referral but does not suggest arterial calcification.
2. An ankle-brachial index of 0.9 is a normal finding.
3. An ankle-brachial index of 1.0 is a normal finding.
4. Ankle-brachial index measures above 1.1 indicate arterial calcification. The calcification limits the compressibility of the artery.
An outpatient physical therapist is working with a patient who suddenly demonstrates repetitive and rhythmic head and neck movements and has an unfocused stare. Which of the following actions should the therapist perform FIRST?
1.Call emergency medical services.
2.Remove objects from the immediate area.
3.Place a tongue depressor in the patient's mouth.
4.Hold the patient's head and neck still.
2,2
1. Seizures are usually finite in duration. Unless the individual develops status epilepticus (which is not described in the stem), calling emergency medical services is not the first action to perform.
2. A patient who is having a seizure normally only needs protection from injury in the environment.
3. It is not appropriate to insert a tongue protector to protect the tongue from injury. This is more likely to harm the patient.
4. The physical therapist could harm the patient by trying to restrict movement.
Which of the following exercise combinations is MOST appropriate for a patient who has a forward head posture?
1.Strengthen the deep cervical flexors and stretch the sternocleidomastoids and upper cervical extensors.
2.Strengthen the deep cervical flexors and sternocleidomastoids and stretch the upper cervical extensors.
3.Strengthen the cervical extensors and stretch the sternocleidomastoids and deep cervical flexors.
4.Strengthen the cervical extensors and sternocleidomastoids and stretch the deep cervical flexors.
1,1
1. A forward head position is due to decreased cervical retraction. Treatment should include deep cervical flexor and shoulder retractor strengthening and cervical extensor and pectoral muscle stretching.
2. Treatment for forward head posture should include deep cervical flexor and shoulder retractor strengthening and cervical extensor and pectoral muscle stretching.
3. The deep cervical flexors should be strengthened, not stretched.
4. The deep cervical flexors should be strengthened, not stretched
A physical therapist is examining a patient who reports decreased walking endurance. The therapist notes that the muscles of the L4 myotome weaken after the patient holds the muscle contraction for 4 seconds. These findings are MOST likely due to:
1.a single nerve root lesion.
2.a central nervous system lesion.
3.femoral nerve compression.
4.central spinal stenosis.
1,1
1. Findings for a single nerve root lesion may not be immediately apparent upon testing but may emerge after a few seconds.
2. Central nervous system lesions typically are not manifested in this way.
3. Peripheral nerve injury will cause weakness that is discernible more quickly than weakness resulting from a single nerve root injury.
4. Peripheral nerve injury will cause weakness that is discernible more quickly than weakness resulting from a single nerve root injury.
Following anterior cruciate ligament reconstruction using a graft from the patellar ligament, which of the following early interventions will BEST facilitate healing of the patellar ligament?
1.High-load short-arc quads
2.Prolonged immobilization with the knee fully extended
3.Deep squats
4.Active knee range of motion
4,4
1. Low loads are indicated at this phase of tissue healing, not high loads. High loads may overload the tissue and cause damage.
2. Prolonged immobilization will lead to adhesions and decreased range of motion, along with weak/unorganized tissue that is less able to tolerate the normal stresses eventually placed upon it
3. Although weight-bearing may provide a low-load stimulus, deep squats are too aggressive at this stage and may cause tissue damage/harm
4. Active range of motion provides a light load similar to normal stress to facilitate tissue healing during the repair and regeneration phase of tissue healing
A physical therapist is guarding a patient who is using an assistive device to come down a flight of stairs. Which of the following is the SAFEST position for the therapist to take to avoid self-injury?
1.In front, with one foot on the step immediately below the patient
2.In front, with both feet on the step immediately below the patient
3.In back, with one foot on the same step as the patient
4.In back, with both feet on the same step as the patient
1,1
1. The physical therapist should stand in front and to the side of the patient with one foot on the step to which the patient will step and the other foot on the next step down.
2. Standing with both feet on the same step will make the physical therapist unstable if the patient begins to fall. This position does not provide a wide anteroposterior base of support.
3. In back, with one foot on the same step as the patient is not the safest position for the physical therapist, because the therapist may be pulled forward if the patient loses balance forward.
4. Standing with both feet on the same step will make the physical therapist unstable if the patient begins to fall. This position does not provide a wide anteroposterior base of support.
A patient reports cervical muscle tightness and headaches originating in the back of the head. Which of the following nerves is MOST likely involved?
1.Trigeminal
2.Spinal accessory
3.Hypoglossal
4.Lesser occipital
2,4
1. The trigeminal nerve (CN V) is a sensory and motor nerve of the face, not the area in which the patient reports pain or tightness.
2. Dysfunction of the spinal accessory nerve (CN XI) is more likely to cause weakness of the sternocleidomastoid and trapezius muscles as well as pain in the neck, shoulder, and scapula rather than the muscle tightness and pain distribution described by the patient.
3. The hypoglossal nerve (CN XII) supplies motor innervation to the muscles of the tongue and is unrelated to the tightness or pain.
4. The lesser occipital nerve is a cutaneous nerve supplying the skin of the neck and scalp posterior superior to the auricle, the area in which the patient reports pain
Which of the following scenarios are accurate, regarding the patient in the video? {shows R knee varus and toe out during gait}
1.The lateral collateral ligament is under stress, and the gemelli muscles are shortened
2.The medial collateral ligament is under stress, and the gemelli muscles are shortened
3.The medial collateral ligament is under stress, and the pectineus muscle is shortened
4.The lateral collateral ligament is under stress, and the pectineus muscle is shortened
4,1
1. The lateral collateral ligament (LCL) resists varus of the knee, and the patient in the knee exhibits genu varum (pp. 928, 946). Hip external rotators are shortened in many cases in which patients exhibit toe-out gait, which is shown in the video (p. 299). The gemelli are hip external rotators
4. The LCL resists varus of the knee, and the patient in the knee exhibits genu varum (pp. 928, 946). While the first part of the response is correct, the pectineus is a hip internal rotator synergist (p. 836). Hip external rotators, rather than internal rotators, are likely to be shortened in gait with toe-out (p. 299). The patient in the video exhibits toe out gait with genu varum.
A patient who sits with a severely slumped forward posture may experience respiratory compromise due to which of the following factors?
1.Entrapment of the intercostal nerves with respiratory muscle weakness
2.Inability of the respiratory muscles to resist gravity
3.Hypermobility of the costovertebral joints
4.Compression of the diaphragm by abdominal contents
4,4
1. The intercostal nerves originate from the thoracic spinal nerve roots. The intervertebral foramina are large in this section of the spine, and entrapment of the nerve roots is rare.
2. The diaphragm descends (moves caudally) during inspiration. In sitting position, gravity would not resist the diaphragm during inspiration.
3. Normal ventilatory mechanics involve the movement of the thorax in all three planes during inspiration. Mobility in the costovertebral joints facilitates chest wall expansion.
4. The diaphragm descends (moves caudally) during inspiration. The severely slumped forward sitting position would lower the diaphragm and cause it to be compressed by the abdominal contents, thereby resulting in respiratory compromise.
A patient who had a posterolateral total hip arthroplasty should AVOID which of the following movements?
1.Hip adduction and hip medial (internal) rotation
2.Hip adduction and hip lateral (external) rotation
3.Hip abduction and hip medial (internal) rotation
4.Hip abduction and hip lateral (external) rotation
3,1
1. Posterior dislocation of the hip can occur in the presence of excessive flexion, adduction, and medial (internal) rotation. This can occur in a patient who has had a posterolateral surgical approach that has weakened the posterior hip capsule.
2. Posterior dislocation of the hip can occur in the presence of excessive flexion, adduction, and medial (internal) rotation, not lateral (external) rotation.
3. Posterior dislocation of the hip can occur in the presence of excessive flexion, adduction, and medial (internal) rotation, not abduction.
4. Posterior dislocation of the hip can occur in the presence of excessive flexion, adduction, and medial (internal) rotation, not abduction and lateral (external) rotation.
Which of the following chronic hormonal responses to exercise may contribute to menstrual dysfunction?
1.High levels of cortisol, low levels of follicle-stimulating hormone (FSH)
2.High levels of cortisol, high levels of follicle-stimulating hormone (FSH)
3.Low levels of cortisol, low levels of follicle-stimulating hormone (FSH)
4.Low levels of cortisol, high levels of follicle-stimulating hormone (FSH)
1,1
1. It has been proposed that exercise stress chronically elevates cortisol levels in athletes. This in turn suppresses the secretion of gonadotropin-releasing hormone (GnRH), which in turn results in the suppression of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Low levels of FSH will result in menstrual dysfunction.
2. Although it has been proposed that exercise stress chronically elevates cortisol levels in athletes, this rise in levels of cortisol suppresses, not stimulates, the secretion of gonadotropin-releasing hormone (GnRH), which in turn results in the suppression of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) rather than stimulation of the secretion of these hormones.
3. It has been proposed that exercise stress chronically elevates cortisol levels in athletes, although lower levels of follicle-stimulating hormone (FSH) will result in menstrual dysfunction.
4. It has been proposed that exercise stress chronically elevates cortisol levels as well as lowers follicle-stimulating hormone levels in athletes.
A patient had a stroke 2 years ago and has been unable to land on the heel during heel strike (initial contact) for the past year. What is the MOST appropriate way for the patient to lengthen the involved muscle?
1.Use of a night splint
2.Use of a hold-relax stretch
3.A 2-minute passive stretch
4.5 bouts of 1-minute passive stretches
1,1
1. The patient has a fibrotic contracture, which may be effectively treated by using prolonged static stretch with a splint.
2. The duration of stretching is not sufficient to address a fibrotic contracture.
3. The duration of stretching is not sufficient to address a fibrotic contracture.
4. The duration of stretching is not sufficient to address a fibrotic contracture.
A patient sustained a distal radius fracture involving the Lister tubercle 6 weeks ago. During a physical therapist's assessment, no limitation in passive range of motion in the thumb (1st digit) interphalangeal and metacarpophalangeal joints is found. What active thumb (1st digit) motion is MOST likely to be affected?
1.Interphalangeal flexion
2.Interphalangeal extension
3.Metacarpophalangeal flexion
4.Metacarpophalangeal adduction
3,2
1. The flexor pollicis longus acts on interphalangeal flexion. Although its proximal attachment is on the radius, it does not wrap around the Lister tubercle.
2. The extensor pollicis longus brevis wraps around the Lister tubercle and attaches distally on the dorsal side of the distal phalange of the thumb (1st digit). If a patient has a fracture to the distal radius and no other soft tissue restrictions are noted, then interphalangeal extension would be affected.
3. The flexor pollicis brevis acts to achieve thumb (1st digit) metacarpophalangeal flexion. The flexor pollicis brevis does not wrap around the Lister tubercle.
4. The adductor pollicis acts to achieve thumb (1st digit) metacarpophalangeal adduction. The adductor pollicis does not wrap around the Lister tubercle.
In a patient with breast cancer, which of the following sites are the MOST common sites of metastasis?
1.Central and peripheral nervous systems
2.Liver and gastrointestinal tract
3.Lungs and bony skeleton
4.Spleen and pituitary gland
3,3
1. The central nervous system is a common metastatic site, but not the peripheral nervous system.
2. The liver is a common metastatic site, but not the gastrointestinal tract.
3. Lungs and bones are common metastatic sites for breast cancer.
4. Neither the spleen nor the pituitary gland is a common metastatic site for breast cancer.
Which of the following muscular responses would be expected during normal micturition?
1.Relaxation of the detrusor and relaxation of the pelvic floor
2.Relaxation of the detrusor and contraction of the pelvic floor
3.Contraction of the detrusor and relaxation of the pelvic floor
4.Contraction of the detrusor and contraction of the pelvic floor
3,3
1. If the detrusor does not contract, the result is incomplete bladder emptying.
2. Neither relaxation of the detrusor nor the contraction of the pelvic floor would allow for complete bladder emptying as expected in normal micturition.
3. The contraction of the detrusor acts to empty the bladder, while the relaxation of pelvic floor allows the urine to pass.
4. Contraction of the pelvic floor would limit the flow of urine.
A patient who is taking an angiotensin-converting enzyme (ACE) inhibitor is performing a therapeutic exercise program in a heated pool. Which of the following physiologic effects is MOST likely to occur in this scenario?
1.Cardiac arrhythmias
2.Increase in fluid retention
3.Decrease in blood pressure
4.Difficulty breathing
3,3
1. Exercise in a heated pool is not a common trigger for arrhythmias. Exercise may be beneficial in patients with cardiovascular issues and decreased tolerance for land-based exercise.
2. With immersion, the physiologic changes include increased need to urinate to eliminate fluid; the need to hydrate orally to replace fluid excreted from the system by renal, endocrine, and cardiovascular responses to immersion; and a potential decrease in systemic and local edema from this peripheral-to-central fluid shift response
3. Both heated aquatic immersion and use of ACE inhibitors are known to cause peripheral vasodilation and therefore, decrease blood pressure. Because two factors are present that would cause low blood pressure, this is most likely to occur.
4. ACE inhibitors are used to primarily to manage blood pressure. This medication does not suggest that the patient has respiratory compromise and the medication does not have respiratory side effects. Therefore, difficulty breathing is not most likely to occur
A physical therapist has been treating a female patient with low back pain for 6 weeks. The patient reports that the pain seemed to lessen earlier in the course of treatment but has intensified again in the past week. To help identify a systemic cause for the pain, the therapist should ask the patient whether the pain:
1.decreases when she lies down.
2.corresponds with her menstrual cycle.
3.increases when she is driving to work.
4.increases when she has a bowel movement
2,2
1. Decreased pain with rest is more likely to indicate a mechanical cause of pain.
2. Pain from endometriosis often is cyclic in nature and corresponds with the menstrual cycle.
3. Pain with driving is more likely to indicate a mechanical cause of pain.
4. Pain with bowel movement is more likely to indicate a mechanical cause of pain.
A patient with C5 and C6 nerve root compression is MOST likely to have a decrease in motor function of which of the following muscles?
1.Elbow flexors
2.Scapular elevators
3.Elbow extensors
4.Finger flexors
1,1
1. The biceps muscle is a critical muscle for the C5 level, so it, and the motion of elbow flexion, are probably impaired if there is damage to C5-C6.
2. The trapezius is innervated by C4 and the spinal accessory nerve (CN XI), so this motion should be intact in this person.
3. The triceps are innervated at the C7 level, so this motion should not be affected by this patient's injury.
4. The finger flexors are innervated at the C8 to T1 level and should be intact.
A patient has a resting blood pressure of 120/80 mm Hg. During an activity with a metabolic equivalent level of 4, which of the following blood pressure responses is MOST likely associated with poor left ventricular function?
1.108/78 mm Hg
2.129/76 mm Hg
3.138/83 mm Hg
4.164/84 mm Hg
1,1
1. A drop in systolic blood pressure greater than or equal to 10 mm Hg with an increase in workload is considered an abnormal response and correlates with left ventricular dysfunction.
2. An increase in systolic blood pressure is a normal response. Diastolic blood pressure may remain the same or increase or drop by 10 mm Hg. This drop in diastolic blood pressure is within normal limits.
3. An increase in systolic blood pressure is a normal response. Diastolic blood pressure may increase or drop by 10 mm Hg. These increases in systolic and diastolic blood pressure are normal.
4. An increase in systolic blood pressure is a normal response. A drop in systolic blood pressure is associated with left ventricular failure.
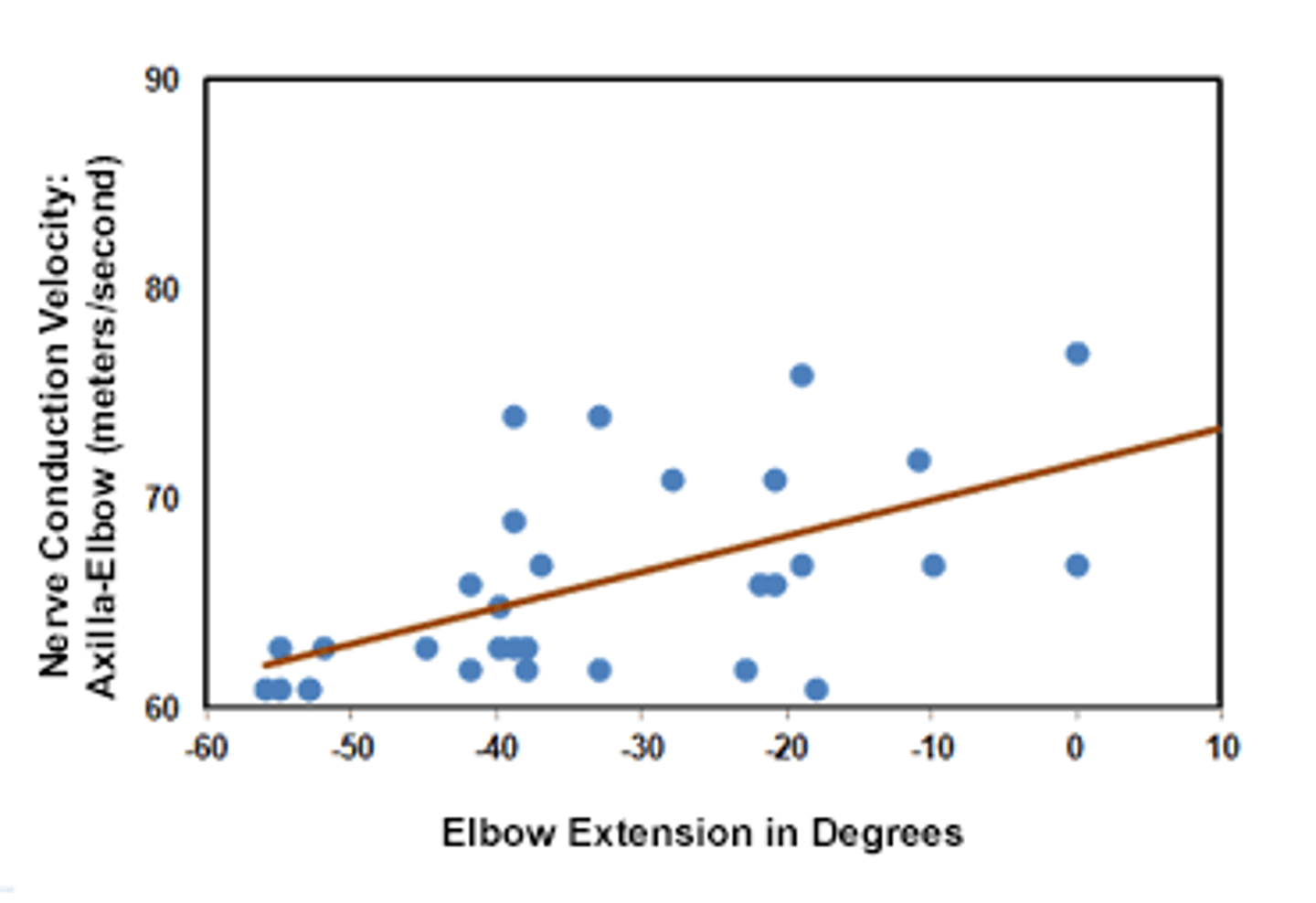
The displayed graph shows conduction velocity testing for the median nerve. According to this graph, which of the following statements BEST describes the relationship between nerve conduction velocity and elbow extension range of motion?
1.There is a positive relationship between the two variables.
2.There is no relationship between the two variables.
3.There is a negative relationship between the two variables.
4.The direction and strength of the relationship cannot be determined.
1,1
1. This scatter plot is a useful method to examine the relationship between the variables. This plot shows a positive relationship.
2. If no relationship existed, then the points representing the variables would be more dispersed or would have a random pattern.
3. The line indicating the relationship of the variables would go in the opposite direction (left higher than right) if a negative relationship existed.
4. This type of scatter plot allows the direction and strength of the relationship to be determined.
Which of the following monofilament grades supplies the MINIMUM amount of force that can be detected by a patient who has protective sensation but not fully normal sensation?
1.3.61
2.4.37
3.5.07
4.6.65
3,3
1. Ability to sense the 3.61 monofilament indicates fully normal sensation because it is smaller than the 5.07 monofilament.
2. Ability to sense the 4.37 monofilament indicates fully normal sensation because it is smaller than the 5.07 monofilament..
3. The 5.07 monofilament supplies the least amount of force that can be sensed by patients with only protective sensation intact.
4. Ability to sense only the 6.65 monofilament indicates a loss of protective sensation because it is larger than the 5.07 monofilament.
The photograph demonstrates the joint integrity test MOST likely to be positive following which type of injury mechanism?
1.Midtarsal stress
2.Dorsiflexion
3.Eversion
4.Inversion
4,4
1. Midtarsal stress is not the traditional method of injury for any single ligament, including anterior talofibular ligament.
2. Dorsiflexion would be the most likely mechanism of injury for the anterior tibiofibular ligament (high ankle sprain), not the anterior talofibular ligament. The integrity of the anterior tibiofibular ligament would be tested with a dorsiflexion/rotation maneuver, not a straight anterior glide.
3. Eversion would be the most likely mechanism of injury for the deltoid ligament, not the anterior talofibular ligament. The integrity of the deltoid ligament would be tested with a straight eversion stress, not a straight anterior glide.
4. The photograph shows an Anterior Drawer Test, which is used to evaluate the anterior talofibular ligament. This is the ligament that is injured most often with an inversion mechanism.

A physical therapist is working with a patient who has pneumonia and who exhibits symptoms of respiratory distress while walking. Which of the following signs is the patient MOST likely to exhibit?
1.Bradypnea
2.Tachypnea
3.Sternal protraction
4.Symmetrical chest expansion
2,2
1. Bradypnea is not a symptom of respiratory distress. A high respiratory rate is associated with respiratory distress.
2. Of the options listed, tachypnea is the most likely symptom of respiratory distress
3. Sternal retraction is a symptom of respiratory distress; however, it is not the most likely symptom of respiratory distress
4. Paradoxic (often asymmetrical) chest expansion is a symptom of respiratory distress; however, it is not the most likely symptom of respiratory distress
Which of the following conditions would MOST likely occur in a patient who has decreased production of insulin?
1.Accelerated fat metabolism
2.Accelerated protein synthesis
3.Increased thirst
4.Decreased urination
3,3
1. Reduction of insulin production results in the opposite effect. Fat production is altered, and fat breakdown occurs to liberate more glucose.
2. Reduction of insulin production impairs protein synthesis because amino acid transport into cells requires insulin.
3. Reduction of insulin production results in large quantities of urine being excreted, resulting in excessive thirst.
4. Reduction of insulin production results in large quantities of urine being excreted.
A patient has a cerebellar dysfunction that affects both the trunk and the limbs. During examination, which of the following findings will MOST likely be observed?
1.Bradykinesia
2.Festinating gait
3.Impairments in muscle force generation
4.Impairments in the timing of muscle activation
4,4
1. Bradykinesia is associated with Parkinson disease and is not seen with cerebellar disorders. Parkinson disease affects the basal ganglia and not the cerebellum.
2. Festination of gait is typically seen with persons living with PD, not persons with cerebellar ataxia. Parkinson disease affects the basal ganglia and not the cerebellum.
3. Cerebellar impairments may cause some hypotonia initially, but patients recover normal passive muscle tone and normal reflexes quickly.
4. Cerebellar dysfunction is characterized by delays in initiating and timing of movements. Ataxia is a general term used to describe abnormal coordination of movements. It is demonstrated by deficits in speed, amplitude of displacement, directional accuracy, and force of movement. Ataxic movements are thought to occur due to impairments in the timing and duration of muscle activation.
A patient has severe chronic obstructive pulmonary disease and bilateral knee osteoarthritis. During aquatic therapy involving slow walking, which of the following water levels is MOST appropriate for this patient?
1.Knees
2.Hips
3.Navel
4.Shoulders
3,3
1. Water level up to the navel would minimize knee compressive force to a greater extent than water level up to the knees, because more loading forces would be removed.
2. Water level up to the navel would minimize knee compressive force to a greater extent than water level up to the hips.
3. Patients who have knee arthritis often have difficulty and pain when walking on land. Buoyancy, ground reaction forces, and knee joint forces are less during walking in the water, compared to these same forces while walking on land. The greater the amount of water displaced by the body, the less the ground reaction forces experienced, and the less force transmitted up the body through the ankles, knees, hips, and trunk. Therefore, as water depth increases and more of the body is immersed in water, knee compressive force decreases. This allows a patient who has knee arthritis to be able to walk in water with minimal difficulty and pain, even though the patient may be unable to walk without pain and difficulty on land. Water level up to the navel would minimize knee compressive force to a greater extent than water level up to the knees or hips.
4. A water level to the shoulders could affect the ability of the lungs to expand
Which of the following scenarios BEST illustrates a violation of the Health Insurance Portability and Accountability Act of 1996?
1.A physical therapist contacts a patient's physician to discuss the patient's progress without asking the patient for written consent to do so.
2.A physical therapist discusses a complicated case with a colleague while driving home together after work without first seeking the patient's consent.
3.A patient asks a physical therapist to release a copy of the evaluation and plan of care to an insurance carrier without providing written consent to do so.
4.A patient asks a physical therapist what surgery another patient underwent and is told that the second patient had a total knee arthroplasty 1 month ago.
4,4
1. The Health Insurance Portability and Accountability Act (HIPAA) specifies that providing information to another health care provider who is involved in the patient's care is acceptable.
2. HIPAA does not prohibit health care providers from sharing information with another provider without written consent when the purpose relates to the provision of the patient's care. Consulting another physical therapist in order to improve care is not prohibited.
3. HIPAA specifies that providing copies of medical records to insurance companies for reimbursement purposes is acceptable.
4. The type of surgery or condition that a patient has is protected health information and should not be divulged without the patient's consent.
A patient in the 3rd trimester of pregnancy has a 2-week history of progressive pain in the right wrist. The right lateral wrist appears swollen, and pain is exacerbated over the styloid process when the patient closes the fingers around the thumb (1st digit) and the wrist is passively moved into ulnar deviation. Which of the following diagnoses is MOST likely?
1.De Quervain tenosynovitis
2.Carpal tunnel syndrome
3.Scapholunate instability
4.Scaphoid fracture
1,1
1. De Quervain tenosynovitis is a progressive condition that affects the tendon sheath of the abductor pollicis longus and extensor pollicis brevis tendons. Arthritis and overuse, consisting of repetitive tasks that involve overexertion of the thumb (1st digit) or radial and ulnar deviation of the wrist, are the most common predisposing factors
2. Compression of the median nerve in the carpal tunnel can occur in pregnancy due to fluid retention or can occur due to repetitive trauma usually associated with repeated wrist flexion and extension. The clinical features include intermittent pain and paresthesia in the median nerve distribution in the hand
3. The lunate is the most commonly dislocated carpal bone, and the scapholunate articulation is the most common area for carpal instability. Scapholunate synovitis or posterior wrist syndrome presents with tenderness or swelling over the posterior wrist.
4. A scaphoid fracture most commonly occurs with a fall on an outstretched hand. Most individuals with a scaphoid fracture have severe discomfort over the scaphoid.
A physical therapist is considering using neuromuscular electrical stimulation as an alternative to static bracing for control of ankle position during gait in a client 3 months post cerebrovascular accident. Which of the following criteria improves chances of success with this treatment approach?
1.Limited spasticity in the ankle plantar flexors
2.Altered selective control of the hip/knee with volitional ankle activity
3.Hyperactive deep tendon reflexes at the ankle and knee
4.Limited sensation of the lower extremity
1,1
1. Spasticity in the ankle plantar flexors may reduce the effectiveness of electrical stimulation; therefore, limited spasticity would improve the chances of success with this treatment.
2. The hip and knee control may be important, but if the patient has volitional ankle activity, electronic stimulation is not needed.
3. Hyperactive deep tendon reflexes indicate spasticity is present, which will reduce the effectiveness of electrical stimulation.
4. Limited sensation may also reduce the effectiveness of electrical stimulation.
A patient reports feeling a "pop" in the posterior leg accompanied by sudden onset of pain localized to the middle third of the posterior lower leg. There is no loss of functional strength. This injury is consistent with complete rupture of the:
1.tibialis posterior muscle.
2.popliteus muscle.
3.Achilles tendon.
4.plantaris tendon.
4,4
1. The tibialis posterior muscle is a significant plantar flexor and invertor of the ankle. Complete rupture of this tendon will significantly affect functional strength evidenced by gait.
2. Rupture of the popliteus tendon will result in decreased knee function and difficulty unlocking the knee from an extended position.
3. Complete rupture at the Achilles tendon will result in the inability to flex the foot and an inability to walk, run, or jump.
4. Rupture of the plantaris is often felt as a "pop." However, the plantaris is a vestigal tendon that has no significant role in function at the knee or ankle
23 y/o female
R post SH pain; mild numbness to lat arm along middle deltoid, onset 2 wks ago after forceful contact of the shoulder with the ground during softball, heard a pop in shoulder; numbness started 1 week later
x-ray (-) fx
College-level softball player
Medications: ibuprofen 800 mg 3 times/day
Pain: 4/10 at worst; intermittent, variable, deep, sharp w/ occasional catching sensation in shoulder
Aggs: throwing more than 20 fast softball pitches (extended arm rotates 360° around the shoulder)
Ease: rest, avoiding throwing
Right SH gross AROM normal, except pain w/:
Abduction at 100°
Flexion at 120°
ER 80°
IR 45°
Right SH
Deltoid (4/5)
Teres minor (4/5)
Infra (4/5)
Subscap (3/5)
Supra (3/5)
No neck pain or pain in LUE
Left SH WFL
Which diagnostic imaging test would be BEST if pain persists?
1.Diagnostic US
2.Computed tomography
3.Magnetic resonance imaging arthrography
4.Magnetic resonance imaging angiography
1. Diagnostic ultrasound is useful in the assessment of the rotator cuff or biceps tendon. Ultrasound is comparable to magnetic resonance imaging in evaluating full-thickness rotator cuff tears and rotator cuff atrophy but is inferior to a magnetic resonance imaging arthrogram in evaluating partial-thickness rotator cuff tears and other intra-articular pathological conditions, such as a labral tear.
2. Computed tomography is used most often to characterize complex fractures to assist in surgical decisions. It has the advantage of characterizing both bony lesions and significant soft tissue injuries and can identify labral tears. However, magnetic resonance imaging arthrography is considered the gold standard for imaging traumatic shoulder injuries, with superior capability in the diagnosis of intra-articular pathological conditions such as superior labral anterior-to-posterior tears, labroligamentous injuries, and partial rotator cuff tears.
3. Magnetic resonance imaging arthrography is considered the gold standard for imaging traumatic shoulder injuries, with superior capability in the diagnosis of intra-articular pathological conditions such as superior labral anterior-to-posterior tears, labroligamentous injuries, and partial rotator cuff tears. The arthrogram injects contrast directly into the joint under fluoroscopy guidance. This is preferred over a magnetic resonance imaging scan with contrast, in which the contrast is injected into the vein and not the joint.
4. Magnetic resonance imaging angiography is used to evaluate the arteries of the cerebrovascular system as well as the aorta and its major branches, the renal arteries, and the lower extremities. It is not used to assess labral tears or intra-articular shoulder conditions.
Which of the following peripheral nerves has MOST likely been injured?
1.Ulnar
2.Median
3.Radial
4.Axillary
2,4
1. The patient's presentation is more consistent with an axillary nerve injury, not an ulnar nerve injury
2. The patient's presentation is more consistent with an axillary nerve injury, not a median nerve injury
3. The patient's presentation is more consistent with an axillary nerve injury, not a radial nerve injury
4. The axillary nerve can be damaged with trauma to the shoulder (subluxations, dislocations, fractures of the humerus, repetitive stretching or compression). Pain is usually present in the posterior shoulder, with sensory disturbances in the lateral aspect of the shoulder (sergeant's patch area). Because the axillary nerve innervates the deltoid and teres minor, these muscles would demonstrate weakness on manual muscles testing. In addition, signs and symptoms of shoulder instability (clicking, giving way) or even wasting of the deltoid may occur.
Which of the following resistance exercise prescriptions is MOST appropriate INITIALLY for this patient?
1.Single-set exercises at low intensities
2.Single-set exercises at high intensities
3.Multiple-set exercises at low intensities
4.Multiple-set exercises at high intensities
1,1
1. Single-set exercises at low intensities should be implemented in the very early phases of a resistance exercise program. In resistance training, the volume of exercise is the summation of the total number of repetitions and sets of a particular exercise during a single exercise session multiplied by the intensity of the exercise. There is an inverse relationship between the sets and repetitions of an exercise and the intensity of the resistance. The higher the intensity or external resistance, the lower the number of repetitions and sets are possible. Conversely, the lower the external resistance, the greater the number of repetitions and sets are possible.
2. This answer is incorrect as single-set exercises at low intensities should be implemented in the very early phases of a resistance exercise program. Higher intensities can be added later on as the patient tolerates lower intensities. Multiple-set exercises are used to progress the program and have been shown to be superior to single-set regimens in advanced training.
3. This answer is incorrect as single-set exercises at low intensities should be implemented in the very early phases of a resistance exercise program or in a maintenance program. Higher intensities can be added later on as the patient tolerates lower intensities. Multiple-set exercises are used to progress the program and have been shown to be superior to single-set regimens in advanced training.
4. This answer is incorrect as single-set exercises at low intensities should be implemented in the very early phases of a resistance exercise program or in a maintenance program. Higher intensities can be added later on as the patient tolerates lower intensities. Multiple-set exercises are used to progress the program and have been shown to be superior to single-set regimens in advanced training.