Biopsychology
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
98 Terms
What is Biopsychology?
Biopsychology is the study of the biological aspects of behaviour and it focuses mainly on two aspects of human physiology. All animals have two major systems that allow them to gain information from the environment and respond to this information; the nervous system and the endocrine system. Biopsychologists use their knowledge of these systems to explain normal and abnormal behaviour.
What is the Nervous System?
The nervous system: This is a specialised network of cells in the human body and is our primary internal communication system. It has two main functions:
● To collect, process and respond to information in the environment.
● To co-ordinate the working of different organs and cells in the body.
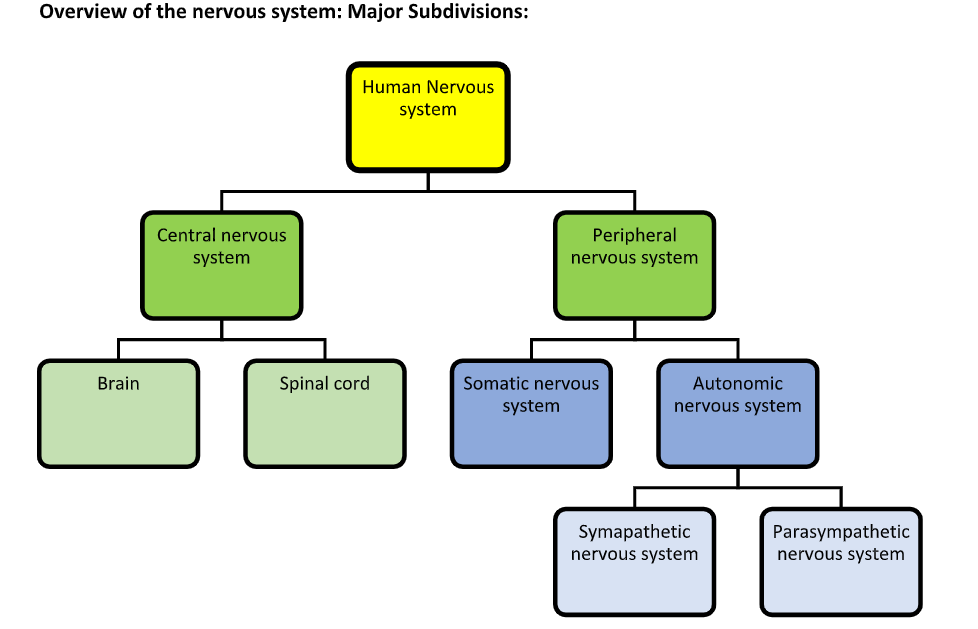
It is divided into two sub-systems:
● Central nervous system (CNS)
● Peripheral nervous system (PNS)
The central nervous system:
The CNS is made up of the brain and the spinal cord.
● The brain is the centre of all conscious awareness. The brain’s outer layer, the cerebral cortex, is highly developed in humans and is what distinguishes us from animals. Only a few living creatures – sponges, sea squirts and jellyfish do not have brain. The brain is divided into two hemispheres, it makes sense of incoming information and processes it so a response can be made.
● The spinal cord is an extension of the brain. It is responsible for the transference of messages to and from the brain as well as reflex actions such as pulling your hand away from a hot plate.
The peripheral nervous system:
The PNS extends beyond the CNS and transmits messages, via millions of neurons (nerve cells), to and from the central nervous system. The peripheral nervous system is further sub-divided into the:
1. Somatic nervous system (SNS) controls the muscle movement and receives information from sensory receptors. It has both sensory and motor pathways and carries commands from the motor cortex in the brain.
2. Autonomic nervous system (ANS) helps to transmit and receive information from the organs. It governs vital functions in the body such as breathing, heart rate, digestion, sexual arousal and stress responses. It has only motor pathways and the control centres are in the brain stem. It can be further divided into the sympathetic nervous system and the parasympathetic nervous system.
Overview of the Nervous System:
Neurons and Synaptic Transmission:
The structure and function of neurons: There are 100 billion neurons (nerve cells) in the human nervous system. 80% of which are located in the brain. By transmitting signals electrically and chemically, these neurons provide the nervous system with its primary means of communication.
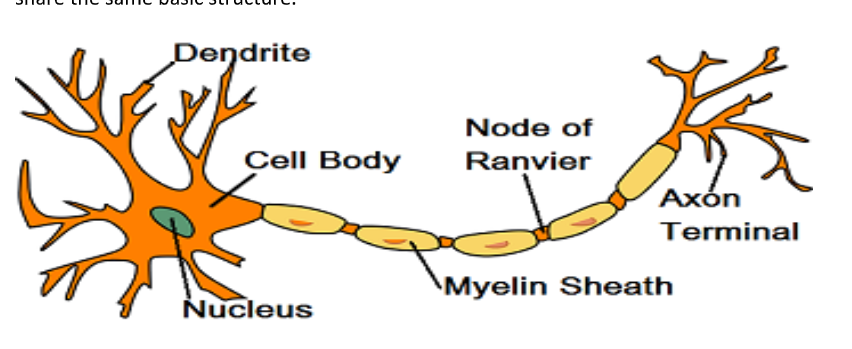
The structure of a neuron:
Neurons vary in size from less than a millimetre to a metre long, but all share the same basic structure.
The cell body (or soma) includes a nucleus, which contains the genetic material of the cell. Branch-like structures called dendrites protrude from the cell body. These carry nerve impulses from neighbouring neurons towards the cell body.
The axon carries the impulses away from the cell body down the length of the neuron. The axon is covered in a fatty layer of myelin sheath that protects the axon from and speeds up electrical transmission of the impulse. If the myelin sheath were continuous this would have the reverse effect and slow down the electrical impulse. Thus, the myelin sheath is segmented by gaps called nodes of Ranvier. These speed up the transmission of the impulse by forcing it to jump across the gaps along the axon. Finally, at the end of the axon are terminal buttons that communicate with the next neuron in the chain across a gap known as the synapse.
Types of neuron:
There are three types of neurons: motor neurons, sensory neurons and relay neurons.
Sensory neurons
Sensory neurons carry electro-chemical nerve signals from the outer parts of the body (periphery such as skin, eyes ears etc.) from one of the five senses into the central nervous system. The electro-chemical signal of sensory neurons only travels in one direction.
Structure:
Long dendrites and short axon. Cell body in the middle of the axon.
Motor neurons
Motor neurons carry electro-chemical nerve signals from the central nervous system to the muscles, organs and glands which mobilises your body and helps it to function. The electro- chemical signal of motor neurons only travels in one direction.
Structure:
Short dendrites and long axons. Cell body at the end.
Relay neurons (Interneurons)
Relay neurons (Interneurons) connect motor and sensory neurons within the central nervous system (i.e. the brain and spinal cord). The electro-chemical signal of relay neurons can travel in either direction.
Structure:
Short dendrites and short axon
How the nervous system controls behaviour: Reflex arc
Reflex reactions in humans are controlled by the reflex arc. When the safety of an organism demands a very quick response, the signals may be passed directly from a sensory neuron, via a relay neuron, to a motor neuron for instant, unthinking action. This is a reflex action. A reflex arc is the nerve pathway, which makes such a fast, automatic response possible. It is in-built, or innate, behaviour, and we all behave in the same way.
A stimulus such as a hot object is detected by the sense organs in the peripheral nervous system, which convey a message along a sensory neuron. The message reaches the central nervous system, where it connects with a relay neuron. This then transfers the message to a motor neuron, which carries the message to an effector such as a muscle causing it to contract and move the hand away. In a more consciously planned move the message will travel to the brain for it to be considered before transferring to a motor neuron.
Electrical transmission – the firing of a neuron:
When a neuron is in a resting state the inside of the cell is negatively charged compared to the outside. When a neuron is activated by a stimulus, the inside of the cell becomes positively charged for a split second causing an action potential to occur. This creates an electrical impulse that travels down the axon towards the end of the neuron.
Synaptic transmission
Neurons communicate with each other within groups known as neural networks. A synapse is a specialised gap that allows electrical messages from one neuron to transfer chemically to an adjacent neuron and this process is known as synaptic transmission.
Initially the electrical nerve impulse travels along the axon of a nerve cell (neurone) towards the pre-synaptic side of the neurone. As the electrical impulse gets closer to the pre-synaptic membrane it prompts the release of neurotransmitters that form into vesicles. The vesicles then merge with the pre-synaptic membrane releasing the neurotransmitter into the synaptic cleft. The neurotransmitter diffuses across the cleft and binds onto the receptor sites on the post-synaptic membrane. This attachment starts a nerve impulse on the post-synaptic side. Any neurotransmitters left in the synaptic gap is then reabsorbed (termed re-uptake process) back into the pre-synaptic neuron enabling the next impulse.
Neurotransmitters
These are chemicals that diffuse across the synapse to the next neuron in the chain. Once the neurotransmitter crosses the gap, it is taken up by the postsynaptic receptor site- in other words, the dendrites of the next neuron. Here, the chemical message is converted back into an electrical impulse and the process of transmission begins again in this other neuron.
A large number of neurotransmitters have been found in the brain (as well as the spinal cord and some glands). Each neurotransmitter has its own specific molecular structure that fits perfectly into a post-synaptic receptor site (complementary)
Neurotransmitters also have specialist functions. An Increased understanding of the way neurotransmitters work in the brain has led to the development of drugs to treat mental disorders. For instance, depression has been linked to a lack of serotonin, which is thought to play an important role in stabilising mood. Also, a category of drugs known as SSRIs (selective serotonin reuptake inhibitors) such as Prozac, slow down the reuptake of serotonin after it has crossed the synapse, ensuring it stays active for longer in the brain.
Excitation and inhibition:
Neurotransmitters have either an excitatory or inhibitory effect on the neighbouring neuron. For instance, the neurotransmitter serotonin causes inhibition in the receiving neuron, resulting in the neuron becoming more negatively charged and less likely to fire. In contrast, adrenaline (an element of the stress response which is both a hormone and a neurotransmitter) causes excitation of the post-synaptic neuron by increasing its positive charge and making it more likely to fire.
Summation:
Often, the activity of individual synapses is not enough to generate postsynaptic action potentials. However, as neurons in the central nervous system are typically made up of thousands of synapses, the action potentials produced by each active synapse can sum together to determine the behaviour of the postsynaptic neuron. This is called summation and means that a neuron integrates the electrical information provided by all the inhibitory and excitatory synapses acting on it at any moment. Whether the sum of active synaptic inputs results in the production of an action potential depends on the balance between excitation and inhibition. If the net or total effect on the post synaptic neuron is inhibitory, the neuron will be less likely to fire but if the net effect is excitatory, the neuron will be more likely to fire.
The Autonomic Nervous System
The autonomic nervous system (ANS) keeps the body functioning in a balanced way by regulating our vital signs (heart, respiration and digestion etc.) as and when it is required. We are not always consciously aware of this, hence the term autonomic. The ANS is responsible for dealing with threats to the body’s existence and for maintaining bodily functions (vital signs). There are two subdivisions of the ANS called the sympathetic nervous system and the parasympathetic nervous system. These two systems work together by having totally opposite functions.
The Sympathetic Nervous System – Speeding You Up!!
The sympathetic nervous system has the function of helping the body respond to emergency situations by speeding up many of our vital signs. For example, stimulating the nervous system to prepare you to either ‘fight or flight’. Digestion will stop and your respiration and heart rates will increase and blood would flow away from internal organs towards muscles enabling you to fight or run away. This will all happen automatically as a result of the sympathetic nervous system.
The Parasympathetic Nervous System – Slowing You Down!!
The sympathetic nervous system is responsible for speeding you up, the parasympathetic nervous system is responsible for slowing your vital signs down (think of para as in parachute which slows you down as you travel through the air). The parasympathetic system then restores your bodily functioning to homeostasis or equilibrium (a state of balance). Your digestion would resume, breathing would become more relaxed and your heart rate would slow and return to normal.
The endocrine system: Glands and hormones:
The endocrine system works alongside and communicates with the nervous system to control vital functions in the body. It acts much more slowly than the nervous system but has widespread and powerful effects. Various glands such as the thyroid gland produce hormones. Hormones are secreted in the bloodstream and affect any cell that has a receptor for that particular hormone. Most hormones affect cells in several organs throughout the body, leading to many diverse and powerful responses.
Thyroid Gland
The thyroid gland produces the hormone thyroxine. This hormone affects cells in the heart (increases heart rate). It also affects cells throughout the body increasing metabolic rates, it regulates metabolic rates (the chemical processes taking place in the cells). This in turn affects growth rates.
Pituitary Gland
The major endocrine gland is the pituitary gland, located in the brain. It is often called the ‘master gland’ because it controls the release of hormones from all the other endocrine glands in the body as well as controlling the release of ACTH and Oxytocin.
Adrenal Gland
The adrenal glands are located above the kidneys and secrete a number of hormones and these secretions help to prepare us for resistance to damage or danger. The most important psychologically is adrenalin. Adrenalin is very important in helping to prepare the body to respond to an emergency or stressful situation. This preparation is referred to as the fight or flight response.
Ovaries (female)
Produces the hormone Oestrogen which regulates the female reproductive system and the menstrual cycle.
Testes (male)
Produces the hormone Testosterone which is involved in the development of male sex characteristics during puberty and muscle growth.
Endocrine and ANS working together: The Fight or flight response:
Often the endocrine system and the ANS work in parallel with each other, for instance in a stressful event. When a stressor is perceived (someone jumping out at you or being scared by a mouse) the first thing that happens is the ANS changes from its normal resting state (parasympathetic state) to the physiologically aroused, sympathetic state. This is termed the fight or flight response and its origins can be found in evolution and the way humans responded to predators.
Flight or Fight Response
Involves three stages as follows:
1. The Immediate Response
2. The Slower Response
3. The Post-Crisis Response
1. The Immediate Response and a State of Preparedness
When the brain perceives a stressful event, the hypothalamus stimulates two processes as a way of responding to the crisis. One takes effect immediately and the other takes approximately 40 seconds to have an impact on your bodily functioning.
The immediate response is where the hypothalamus stimulates both the sympathetic nervous system and the medulla of the adrenal gland to prepare you to stay and fight or to run away. The sympathetic response will dilate your pupils, increase your heart and respiration rate and attempt to cool your body down (sweating) and it will also inhibit functions such as salivation, digestion and sexual activity to maximise the body’s resources to deal with the immediate crisis. There will also be an immediate adrenal gland response via the endocrine system. The medulla, which is the inner part of the adrenal glands is stimulated to release adrenalin which will help to put you into a heightened state of awareness. This heightened state is often referred to as the adrenalin rush.
2. The Slower Response – The Production of Energy
When the initial instant nervous system and adrenal gland response to a crisis is stimulated a slower response is also initiated. This slower response will take approximately 40 seconds to have a physiological effect on the body.
At the same time that the hypothalamus stimulates the medulla and the sympathetic nervous system it will also stimulate the pituitary gland to release the stress hormone ACTH. ACTH then in turn stimulates the cortex of the adrenal gland (the outer part). This is designed to release cortisol which will begin the production of glucose which is required to provide muscles with energy. This muscle energy resource enables you to sustain the action of fight or flight over a period of time should you need to.
3. The Post-Crisis Response and Homeostasis
Although the fight or flight response is undoubtedly valuable to us in a threatening or stressful situation, prolonged exposure to these stress hormones can be particularly damaging not only physically (digestion and heart problems) but also psychologically.
Once the crisis/stress is over the parasympathetic system will return the body physiologically to a state of homeostasis (balance). The parasympathetic system will slow vital signs such as your heart and respiration down and as the body cools down the sweating will stop. Functions such as salivation, digestion and sexual will be returned to normal functioning. Following a crisis and the parasympathetic response a person will usually feel very tired (depletion of energy resources), hungry (digestion has been prevented) and very thirsty (sweating depletes fluids).
Evaluation of the Fight or Flight Response:
Physically and psychologically damaging: – While the fight or flight response may have been a useful survival mechanism for our ancestors, who faced genuinely life-threatening situations (e.g. from predators), modern day life rarely requires such an intense biological response. Furthermore, the stressors of modern day life can repeatedly activate the fight or flight response, which can have a negative consequence on our health. For example, humans who face a lot of stress and continually activate the sympathetic nervous system, continually increase their blood pressure which can cause damage to their blood vessels and heart disease. This suggests that the fight or flight response is a maladaptive response in modern-day life.
Freeze response: When faced with a dangerous situation our reaction is not limited to the fight or flight response; some psychologists suggest that humans engage in an initial ‘freeze’ response. Gray (1988) suggests that the first response to danger is to avoid confrontation altogether, which is demonstrated by a freeze response. During the freeze response animals and humans are hyper-vigilant, this allows them to assess the threat before responding to decide the best course of action for that particular threat. This gives an adaptive advantage as we are able to choose the best response to a particular threat.
Typically a male response to danger – Early research into the fight or flight response was typically conducted on males (androcentrism) and consequently, researchers assumed that the findings could be generalised to females. This highlights a beta bias within this area of psychology as psychologists assumed that females responded in the same way as males, until Taylor provided evidence of a tend and befriend response. According to Taylor et al (2000) women are more likely to protect their offspring (tend) and form alliances with other women (befriend), which would strengthen their position rather than fight an adversary or flee. Furthermore, the fight or flight response may be counterintuitive for women, as running (flight) might be seen as a sign of weakness and put their offspring at risk of danger.
Biological Reductionism - The fight or flight response is biologically reductionist as it argues that biological structures underpin behaviour. This means it reduces human behaviour and cognitive processes down to biological processes. Many psychologists suggest that explaining complex human behaviour by hormone levels alone is too simplistic.
Localisation of function:
During the 19th century it was discovered that certain areas of the brain held particular functions. This is known as ‘localisation of brain function’ Localisation: the theory that specific areas of the brain are associated with particular physical and psychological functions.
Hemispheres
The brain is divided into two hemispheres: the left and the right which are connected by the corpus callosum. The corpus callosum acts as a communication pathway so that the two hemispheres can exchange information. The brain is contralateral (opposite sides); so parts of the left hemisphere deal with the right side of the body and the right side of the brain does the same for the left side of the body. If a function is dealt with by one hemisphere it is said to be lateralised. Lateralisation: the dominance of one hemisphere of the brain for particular physical and psychological functions. So the division of functions between the two hemispheres is called hemispheric lateralisation as the hemispheres have different functions. Each hemisphere (side of the brain) is responsible for specific functions. In most respects , the left and right sides of the brain are very similar. One difference however is the presence of the language areas, which are only found on the left hand side.
Each Hemisphere is divided into four lobes: What are they?
Frontal lobe, Parietal lobe, Temporal Lobe and Occipital lobe.
The Frontal Lobe
The Frontal Lobe is the location for awareness of what we are doing within our environment (our consciousness). The frontal lobe is responsible for executive functioning (organising thoughts) and located at the rear of the frontal lobe is the motor cortex which is responsible for motor function. Broca’s Area is located in the left frontal lobe and is responsible for controlling motor information to produce language.
The Parietal Lobe
The Parietal Lobe is the location for sensory and motor movements. The parietal Lobe is responsible for emotions and sensations generally and located at the rear of the parietal lobe is the somatosensory cortex which is responsible for responding to sensations of cold, heat, touch and pain.
The Temporal Lobe
The Temporal Lobe is the location for auditory ability and memory acquisition. The temporal lobe contains the auditory cortex which is mainly responsible for processing auditory information from the ears. Wernicke’s area is located in the left temporal lobe and is responsible for recognition of the spoken word and speech comprehension.
The Occipital Lobe
The Occipital Lobe is the location for vision. The occipital lobe contains the visual cortex which receives and processes information directly from the eyes. Damage to the back of the left hemisphere may produce loss of vision to the right side of our environment in both eyes.
Motor cortex
It is situated at the back of the frontal lobe on both sides. This is where movement is centred in the brain with the left motor cortex relating to the right side of the body and vice versa. It is particularly important for the control of complex voluntary movement and damage to this area of the brain may result in a loss of control over fine motor movement.
Somatosensory cortex
At the front of both parietal lobes is the somatosensory area which is separated from the motor area by a ‘valley’ called the central sulcus. The somatosensory area is where sensory information from the skin via heat, pressure or touch is represented. The more sensitive an area is the greater the amount of the somatosensory area is devoted to that area. For example, receptors for the face and hands occupy over half of the somatosensory area.
Visual cortex
The visual cortex is located in the occipital lobes at the back of the brain. The eyes send information from the visual field to the visual cortex (information from the right visual field is sent to the left visual cortex and from the left visual field to the right visual cortex). Therefore, damage to the left hemisphere could produce blindness in part of the right visual field of both eyes.
Auditory cortex
This is located in the temporal lobes, the auditory areas analyses speech-based information. Damage may produce partial hearing loss.
Language centres: Broca’s and Wernicke’s areas.
In most people, the language centres are in the left hemisphere, which is where most language processing is situated. This means that language is lateralised but some areas of language such as speech production and speech comprehension are localised as well.
Broca’s area.
Broca’s work led to the identification of the area in the brain responsible for speech production. Broca’s Area is located in the left frontal lobe and is responsible for controlling motor information to produce language (mouth, lips larynx). Broca’s Aphasia is a disorder caused by damage to Broca’s Area. Patients can understand language but cannot produce the appropriate sounds associated with language. Typically, they will produce slow laborious speech that lacks fluency.
Wernicke’s area
Wernicke suggested that the area now called Wernicke’s area was important for understanding language and accessing words. Wernicke’s Aphasia is when damage to this area means the person finds it difficult to understand (comprehend) the spoken word and produces ungrammatical speech. In contrast to Broca’s Aphasia speech is fluent.
Evaluation of Localisation
Brain scan evidence of localisation: There is evidence to support the idea that many neurological functions such as language and memory are localised. Peterson et al (1988) used brain scans to demonstrate how Wernicke’s area was active during a listening task and Broca’s area was active during a reading task supporting the theory that these areas of the brain have different functions.
Lashley’s research: The work of Lashley (1950) suggests that higher cognitive functions such as the processes involved in learning are not localised but distributed in a more holistic way in the brain. Lashley removed between 10 and 50 % of the cortex of rats that were learning a maze and demonstrated that no one particular area was more important than another in relation to the rat’s ability to learn the maze. The process of learning appeared to require every part of the cortex. This suggests that some simpler functions such as motor control may be localised but learning is too complex to be localised and requires the involvement of the whole brain. However, as this research was conducted on animals it may not be appropriate to generalise these findings to human learning.
Plasticity: An argument against localisation of function is the notion of plasticity. When the brain has been damaged and a particular function affected, the rest of the brain appears, in some circumstances to be able to reorganise itself in an attempt to recover the lost function. This supports the holistic theory rather than the localisation theory because more than one part of the brain is capable of carrying out a function if the area that normally carries it out is damaged. The surviving areas of the brain contribute so that neurological activity can be carried out.
The case study of Phineas Gage: Before brain imaging, localisation of function was investigated by case studies of people who had suffered trauma. Phineas Gage was a railway worker who, in an accident, had a metre-long iron rod blasted through his head from his chin and out through his forehead. He recovered physically but psychologically he was a changed man. Before the accident he was mild mannered and calm but following it he was hostile and rude. This area that was damaged in Phineas has subsequently been found to be responsible for planning, reasoning and control in the individual thus supporting the notion of localisation of function. It is important to consider that this is a case study so while providing valuable information it is very difficult to generalise from the case of Phineas to the wider population as it is such a unique case.
Brain Plasticity
This describes the brains tendency to change and adapt as a result of experience and new learning. As we age rarely used connections are deleted and frequently used connections are strengthened in a process known as cognitive pruning.
Research into plasticity
Maguire et al (2000)- In this study, Maguire et al (2000) studied the brain scans of 16 London taxi drivers and found that they had a particularly large posterior hippocampus than the control group. The posterior hippocampus was largest in taxi drivers with more than 40 years of experience navigating the streets of London. The hippocampus is a region of the brain that is associated with the development of spatial and navigational skills. As part of their training, London cabbies take a complex test, which assesses their recall of the streets and routes in London. It appears that the result of this learning experience altered the structure of their brains.
Strengths of the Maguire study include:
✔ Control group allows us to say that there is a significant difference between taxi drivers and others (good design).
✔ Use of scientific, objective measurements (MRI) increases validity.
✔ An attempt to study a real world phenomena. High in ecological validity.
Limitations of Maguire
However, we can’t be sure that the difference is due to the ‘knowledge’, as they weren’t tested before. They could have been taxi drivers because of the already existing difference (although the positive correlation between experience and structure makes this less likely). This means we cannot establish cause and effect.
Functional recovery of the brain after trauma
Following physical injury or trauma unaffected areas of the brain are able to adapt and compensate for those areas that are damaged. The functional recovery that may occur in the brain after trauma is an example of neural plasticity. Healthy brain areas may take over the functions of those areas that are damaged. Neuroscientists suggest that this process can occur quickly after trauma and then slow down after several weeks or months.
What happens in the brain during recovery?
The brain is able to rewire and reorganise it’s self by forming new synaptic connections close to the area of damage. Secondary neural pathways that would not typically be used to carry out certain functions are ‘unmasked’ to enable functioning to continue. This process is supported by a number of structural changes:
1.Axon sprouting: new nerve endings grow and connect with undamaged areas.
2. Reformation of blood vessels.
3. Recruitment of homologous (similar) areas on the opposite hemisphere to do specific tasks. E.g if Brocas area was damaged then an area on the right might take over
Research into functional recovery:
Tajiri et al (2013) provided evidence for the role of stem cells in recovery from brain injury. They randomly assigned rats with traumatic brain injury to one of 2 groups. One group received transplants of stem cells into the region of the brain affected by traumatic injury. The control group received a solution infused into the brain containing no stem cells. Three months after the brain injury, the brains of stem cell rats showed clear development of neuron-like cells in the area of injury. This was accompanied by a solid stream of stem cells migrating to the brain’s site of injury. This was not the case with the control group. This study supports the theory that the brain can reorganise itself and new synaptic connections can be made.
Strengths of Tajiri
✔ Animal studies enable us to monitor the function of the brain before and after trauma because we cause it. Ethically we couldn’t do this in humans and it’s unlikely that we would have measured their function before a natural event (because we didn’t know it was going to happen).
Limitations of Tajiri
X But it is an animal study so is hard to generalise to humans.
Evaluation of Functional Recovery:
Practical application: Understanding the process involved in plasticity has contributed to the field of neurorehabilitation. Following illness or injury to the brain, spontaneous recovery tends to slow down after a number of weeks so physical therapy may be required to maintain improvements in functioning. Techniques may include movement therapy and electrical stimulation of the brain to counter the deficits in motor and/or cognitive functioning that may be experienced following something such as a stroke. This shows that although the brain may have the capacity to ‘fix itself’ to a point, this process requires further intervention if it is to be completed successfully.
Age and plasticity: Functional plasticity tends to reduce with age, this means that recovery from trauma is more likely while the brain is still maturing. The brain has a greater natural tendency for reorganization in childhood as it is constantly adapting to new experiences and learning. However, studies have suggested that even abilities commonly thought to be fixed in childhood can still be modified in adults with intense retraining. Bezzola et al (2012) demonstrated how 40 hours of golf training produced changes in the neural representation of movement in 40 to 60 year old participants. Using fMRI, the researchers observed reduced motor cortex activity in novice golfers compared to a control group, suggesting more efficient neural representations after training. This shows that neural plasticity does continue throughout the lifespan.
Educational attainment and functional recovery: Schneider et al (2014) found that patients with the equivalent of a college education are seven times more likely than those who didn’t finish high school to be disability-free one year after a moderate to severe traumatic brain injury. They carried out a retrospective study based on data from the US Traumatic Brain Injury Systems Database. Of the 769 patients studied, 214 had achieved disability-free recovery (DFR) after one year. Of these, 39.2% of the patients with 16 or more years of education had achieved DFR compared to just 9.7% of those with less than 12 years of education achieved DFR after just one year. The researchers concluded that ‘cognitive reserve’ (associated with greater educational attainment) could be a factor in neural adaptation during recovery from traumatic brain injury.
Gender: Although research is inconclusive in this area, there is some evidence to suggest that women recover better than men from brain injury as their function is not as lateralised (concentrated in one hemisphere). Ratcliffe et al (2007) examined 325 patients with brain trauma for their level of response for cognitive skills. The patients were 16 – 45 years old at injury, received rehabilitation at a care facility and completed a follow up one year later. When assessed for cognitive skills, women performed significantly better than men on tests of attention/working memory and language whereas men outperformed women in visual analytic skills. Overall the result suggests a better recovery for women but the results do not control for performance pre-injury which could be a confounding variable.
Hemispheric lateralisation
The idea that the two halves of the brain are functionally different and that certain mental processes are mainly controlled by one hemisphere rather than the other.
The right hemisphere controls the left side of the body and the left hemisphere controls the right side of the body. Language is usually processed by the left hemisphere. The processing of faces and emotion is carried out by the right hemisphere.
Research into ‘split-brains’: Sperry (1967)
Sperry studied a group of individuals who had suffered from epilepsy and who had undergone surgery in which the corpus callosum and other tissues which connect the two hemispheres of the brain had been severed. This meant the main communication line between the two hemispheres was removed. This provided a unique opportunity and allowed Sperry to see the extent to which the two hemispheres were specialised for certain functions and whether the hemispheres performed tasks independently of one another.
Procedure:
Sperry devised a procedure which involved covering one of the patients eyes and presenting a word or picture into the left or right visual field for a split second. This ensured that Sperry knew which hemisphere of the brain was being used. This is because if presented to the patient’s right visual field (RVF) the information was processed by the left hemisphere. If presented to the patients left visual field (LVF) the information was processed by the right hemisphere. He compared the performance of the 11 participants on various tasks with the performance of people with no inter-hemisphere de-connection. By doing a number of variations of tasks using this procedure he was able to draw conclusions about the functions of the differing hemispheres.
Sperry’s Variations: The describe what you see task
The describe what you see task- here a picture was presented to either the left or right visual field and the participant had to simply describe what they saw.
Findings:
When information was presented in the RVF and therefore processed by the left hemisphere patients could describe what they saw, showing the superiority of left hemisphere for language. However, when information was presented in the LVF and processed by the right hemisphere the patients could not describe what was shown and often said there was nothing present, Again indicating that the left hemisphere has superior language ability.
Sperry’s Variations- Tactile Test
Tactile Test- In the tactile test, an object was placed in the patient’s left or right hand and they had to either describe what they felt, or select a similar object from a series of alternate objects.
Findings:
When an object was placed in the right hand this was processed by the left hemisphere. Patients could describe verbally what was in their hand and could also select a similar object from some other objects presented to them, which they could not see. However, when an object was placed in their left hand and processed by the right hemisphere the patient could not describe the object and often made wild guesses. The left hand could identify a similar object by selecting one from a range given. This shows again the superiority of the left hemisphere for language.
Sperry’s Variations: The drawing task
The drawing task- Finally, in the drawing task, participants were presented with a picture in either their left or right visual field, and they had to simply draw what they saw. In the normal brain the corpus callosum would immediately share the information between both hemispheres giving a complete picture of the visual world. However, presenting the image to one hemisphere of a split-brain patient meant that the information could not be conveyed from that hemisphere to the other.
Findings:
When a word was presented in the RVF this would be processed by the left hemisphere and this would control the right hand. Patients would attempt to draw a picture but it was not clear, even thought they were right handed. In contrast when a word was presented to LVF to be processed by the right hemisphere in control of the left hand the picture was clearer and better even though the participants were right handed. This demonstrates the superiority of right hemisphere for spatial tasks.
Overall Conclusions from Sperry:
Findings from a variety of research including the split-brain research has led to a general model of hemispheric specialisation. The left hemisphere is seen as more analytic and verbal and the right hemisphere as more visuo-spatial and musical.
Evaluation of Sperry:
Sperry’s pioneering work: The research carried out on split brain patients has made a key contribution to our understanding of brain processes. The main conclusions are that the left hemispheres are more analytic and verbally orientated and the right is more adept at performing spatial tasks and music. The right hemisphere can only produce rudimentary language.
Methodology: The experiments made use of innovative standardised procedures that enabled Sperry to test the left and right visual field separately ensuring only one hemisphere was receiving information. The experiment had controlled conditions and followed a standardised procedure which increases the internal validity and reliability. However, there were many extraneous variables that could have confounded his results so it is important that other research (that could be more controlled) using neurotypical participants has subsequently supported his findings.
Issues with generalisation: The split-brain patients constitute a very unique sample of people, therefore limiting generalisability as this is not large enough sample to generalise. There were 11 people who made up the sample which limits population validity. They all had a history of epileptic seizures but varied in age, gender and handedness. There was also differences in the age at which they developed epilepsy, had the operation and when they were tested. It is also true that the disconnection between the hemispheres was greater in some patients than others. For these reasons it is not possible to build a universal model of hemispheric lateralisation using only split-brain research. It may be inappropriate to make generalisations about non-epileptic brain patterns from these patients. The epileptic seizures could have made changes to the brains that could have affected the findings.
Language may not be restricted to the left hemisphere. Gazzaniga (1998) suggests that some of the early discoveries from split-brain research have been disconfirmed by more recent discoveries. E.g. split-brain research had suggested that the right hemisphere was unable to handle even the most rudimentary language. Damage to the left hemisphere was found to be far more detrimental to language function than was damage to the right. However, case studies have demonstrated that this is not necessarily always the case. One patient, known as J.W., developed the capacity to speak out of the right hemisphere, with the result that J.W. can now speak about information presented to the left or to the right brain. This suggests that language may not be exclusively limited to the left hemisphere. It also supports brain plasticity as before his surgery (callosotomy) he had language dominant left hemisphere so it shows the brain can recover functions.
Biopsychology: Ways of investigating the brain
Key Terms
Invasive – Inside the brain
Non-invasive – Does not enter the brain
Spatial resolution – Refers to the smallest feature that can be detected, allows discrimination between brain areas to be made accurately.
Temporal resolution – Refers to accuracy in relation to time – how quickly the scanner can detect changes in brain activity.
Some modern scanning techniques are able to record global neural activity through the assessment of brainwave patterns whilst others are able to hone in on activity in specific parts of the brain as the brain performs certain tasks and processes. Psychologists can gain important insights into the brain’s function.
Scanning technology
There are a number of different scanning techniques including MRI, fMRI, PET. They provide images of cortical activity or structure of brain.
MRI scans (Magnetic resonance imaging)
The human body is made up of water molecules. Hydrogen molecules contain protons: like tiny magnets and very sensitive to magnetic fields. When under the powerful MRI scanner magnets, with bursts of radio waves the signals produced provide information that helps to distinguish between the various types of tissue in the body. In an MRI scan, the goal is to get an image of anatomical features in a given area of the body, like the abdomen or brain. The equipment can be used to generate high resolution images where various organs will appear as clearly distinct from each other, and abnormalities such as tumours can be seen.
Advantages of MRI scans:
MRI scans are non-invasive and therefore safe without ethical concerns.
They produce high spatial resolution images that allow abnormalities to be identified.
Disadvantages of MRI scans:
However, a problem with MRI scans is the cost. They are very expensive to carry out as specialist equipment is required.
One drawback is that brain activity is not recorded, it only provides static images which means that it cannot provide more detailed information about the brain (unlike fMRIs)
PET Scans
The patient is injected with a very small amount of radioactive glucose. The PET scan records the absorption of the radioactivity from outside the scalp. If brain cells are active they will consume more of the glucose, this is shown on a colour-coded brain map.
Strengths of PET scans
PET scans are non-invasive so are not painful for the patient.
They produce 3D colour images that show brain activity so comparisons can be made between normal and abnormal activity.
Weaknesses of PET scans
A problem with PET scans it that they use radioactive substances so provides a health risk if used too often. For this reason, they are not used with children.
fMRI Scans (functional magnetic resonance imaging)
This is a technique for measuring changes in brain activity while a person performs a task. It does this by measuring changes in blood flow in particular areas of the brain, which indicates increased neural activity in those areas. It measures blood flow in the brain using radio waves and a magnetic field. If a particular area of the brain becomes more active, there is an increased demand for oxygen in that area. The brain responds to this extra demand by increasing blood flow, delivering oxygen in the red blood cells. So, when an area of the brain is active it is therefore using more oxygen, the change in the amount of energy released by the haemoglobin is detected by the magnet in the scanner and the changes measured. As a result of these changes in blood flow, researchers are able to produce maps showing which areas of the brain are involved in a particular mental activity. This gives a dynamic (moving) picture that shows activity about 1 - 4 second after it occurs and it is thought to be accurate within 1–2 mm.
Strengths of fMRIs
fMRIs are non-invasive - This means they are virtually risk-free and straightforward to use. fMRIs, unlike PET scans, do not rely on the use of radiation so therefore are not as dangerous. They can be used more widely to gain further insight in to brain function.
fMRIs have high spatial resolution - They produce images that have a very high spatial resolution, giving detail by the millimetre that are accurate to within 1- 2 mm. This means they have greater accuracy in comparison to EEGs. This means that psychologists can discriminate between brain regions with accuracy.
Weaknesses of fMRIs
fMRIs are costly - fMRI is expensive compared to other neuroimaging techniques and can only capture a clear image if the person stays perfectly still.
Poor temporal resolution - fMRIs have poor temporal resolution because there is around a 4 second time-lag behind the image on the screen and the firing of the neurons. This is poor in comparison to EEGs/ERPs that have a temporal resolution of 1-10 milliseconds. Therefore fMRIs cannot predict onset of brain activity very accurately.
Lacks detail - fMRI can only measure blood flow in the brain. It cannot hone in on the activity of individual neurons and so it can be difficult to tell exactly what kind of brain activity is being represented on the screen.
Causation – fMRIs do not produce a direct measurement of neural activity, it measures changes in blood flow. Therefore it is not possible to establish cause and effect, as it is based on correlation. This suggests a relationship may exist and so provides the opportunity for further research.
Difference between MRI and fMRI
One key difference between MRI and fMRI is that MRI can generate static images that may be reviewed later for information about the inside of the patient’s body. In an fMRI study, the result is a real-time log of brain activity. It can be frozen at individual frames, such as a highlight of brain activity, or it may be viewed in video form later. Researchers might want to use fMRI to identify the areas of the brain involved in particular responses, for example, a doctor might order the test to see why a patient can’t perform some cognitive tasks.
Electroencephalograph (EEG)
EEGs work on the basis that information in the brain is processed as electrical activity, in the form of action potentials or nerve impulses. This electrical activity is measured within the brain via electrodes that are fixed on the scalp, usually using a skullcap. Electrodes are placed on the scalp and sometimes on the face to monitor eye movements. Electrical activity in the brain is recorded directly under the electrode to reveal the frequency of the ‘brain wave’. The recording is presented in a graph that represents the brainwave patterns that are generated from the action of millions of neurons, providing an overall account of brain activity. There are 4 types of EEG patterns: Alpha waves, Beta waves, Theta waves and Delta waves. Each has two properties: Amplitude – the intensity or size of the activity and Frequency – the speed or quantity of the activity. EEGs are often used by clinicians as a diagnostic tool. Patterns are synchronised (regular – sleep) or desynchronised (irregular – awake) Desynchronised or unusual patterns of activity (no particular rhythm) may indicate neurological abnormalities such as epilepsy, tumours, or disorders of sleep.
Strengths of EEGs
Useful Diagnostic tool - EEGs are important in the diagnosis of conditions such as epilepsy, a disorder characterised by random burst of activity in the brain that can be easily detected. Similarly, it has contributed much to our understanding of the stages involved in sleep.
Safe and Non-invasive - EEG is non-invasive, does not use radiation and therefore is virtually risk free. It is also less expensive than other methods such as fMRI which makes it widely available to researchers in order to further develop understanding of psychological phenomena such as sleep.
High temporal resolution - EEG technology has extremely high temporal resolution. Today’s EEG technology can accurately detect brain activity at a resolution of 1-10 ms. This means it has the advantage of recording in real time leading to accuracy of measurement.
Weaknesses of EEGs
Different brain regions - EEGs tend to produce very generalised information from several areas of the brain so it is not useful for pinpointing the exact source of neural activity. This means that EEGs do not allow researchers to distinguish between activity originating in different but adjacent locations of the brain.
Event Related Potentials (ERPs)
ERPs use the same equipment as EEG; electrodes are placed on the scalp in both methods of recording. The key difference between EEGs and ERPs is that with ERP a stimulus is presented (image or sound) to a participant and the researcher looks for activity related to the stimulus. The stimulus is presented many times (100s) and an average response is put on a graph. Research has shown different forms of ERPs, linked to cognitive processes such as attention and perception.
Strengths of ERPs
Specificity - ERPs bring much more specificity to the measurement of neural processes than could be achieved using raw EEG data.
As ERPs are derived from EEG measurements, they have excellent temporal resolution, especially when compared to fMRIs. (1-10ms)
Cognitive function - The excellent temporal resolution of ERPs have led to their widespread use in the measurement of cognitive functions and deficits.
Researchers have been able to identify many different types of ERP and describe the precise role of these in cognitive functioning including parts of working memory.
Weaknesses of ERPs
Lack of standardisation - Critics have pointed to a lack of standardisation in ERP methodology between different research studies, making it difficult to confirm findings.
Difficult to eliminate extraneous material - A further issue is that, in order to establish pure data in ERP studies, background noise and extraneous material must be completely eliminated, which is not always easy to do.
Poor spatial resolution. This is because they only detect activity in superficial areas of the brain (cortex) and are unable to provide information on what is happening in the deeper regions of the brain such as the hypothalamus making it limited in comparison to fMRI which has high spatial resolution.
Post Mortems
This is a technique that involves the analysis of a person’s brain following their death. In psychological research, those whose brains are subject to a post-mortem are likely to be those who have a rare disorder and have experienced unusual deficits in mental processes or behaviour during their lifetime. Areas of damage within the brain are examined after death as a means of establishing the likely cause of an affliction the person suffered while alive. This may also involve comparing the brain of the person who has died with a neurotypical (healthy) brain in order to see the extent of the difference. Paul Broca (1824-1880) helped to pioneer localisation of function. He used post-mortems and compared function before death with structural damage located after death. This is how he discovered that language and speech originated in the frontal lobe.
Strengths of Post Mortems
Developed understanding. Post-mortem (PM) evidence was vital in providing a foundation for early understanding of key processes in the brain. Both Broca and Wernicke relied on PM studies in establishing links between language, brain, and behaviour decades before neuroimaging began.
Detailed examination - PMs provide a detailed examination of the anatomical structure and neurochemical aspects of the brain that is not possible with scanning techniques. PMs can access areas like the hypothalamus and provide precise detail and insight into deeper brain regions. This has led to new areas of research.
Weaknesses of Post Mortems
Cause and effect. Causation is an issue within PMs. Observed damage to the brain may not be linked to the deficits under review. It may be due to some other unrelated trauma or decay. Therefore cannot conclude the deficit is caused by the damage in the brain. Many extraneous variables affect PM results such as cause of death, age, medication etc.
Ethical concerns. PM studies raise ethical issues with regard to informed consent. Although it is ‘invasive’ this is not an issue. But whether the patient provides consent before death raises severe ethical concerns. Furthermore many post-mortems are carried out on individuals with severe psychological deficits such as HM who are unable to provide fully informed consent.
Biological Rhythms
Most human and non-human animal functions are cyclic, alternating over a period of time. Obvious examples include the sleep-wake cycle which repeats over a 24-hour cycle, or the hibernation patterns of some creatures that typically rest through the winter months and awaken in spring. The major debate, is to consider to what extent biological rhythms are determined by internal clocks (endogenous factors) and by environmental/external factors (zeitgebers).
Circadian Rhythms
Relates to a cycle that repeats over an approximate 24 hour period. There are some cycles that we are consciously aware of; the sleep/wake cycle being an obvious one which dictates when humans and animals should be asleep and awake. Light provides the primary input into this system, acting as the external cue for sleeping or waking. Light is first detected by the eye, which conveys a message regarding the level of brightness to the suprachiasmatic nucleus (SCN). The SCN uses this information to coordinate the activity of the entire circadian rhythm system.
Other cycles we are not usually aware of such as our core body temperature; this fluctuates over a 24- hour period. Generally, it peaks mid-afternoon at about 37.1 C and troughs in the early hours at about 36.7 C.
Evaluation of Circadian Rhythms
Supporting research: Siffre (1975) conducted a case study using himself as the participant. Siffre spent six months in a cave with no natural light or cues as to the day or time. When he woke he would use artificial light to help him navigate within the cave and keep himself busy. His internal body clock was allowed to ‘free run’ and settled into a sleep/wake cycle of between 25 and 30 hours. He lost track of how many days he had been in the cave, believing it to be one month less than he had actually stayed in. He was in the cave for a total of 170 days. This suggests that natural light sources in the environment are vital for keeping the individual to a 24-hour cycle.
Further support: To study endogenous clocks it is necessary to isolate people from external cues for many months. In 1962 Aschoff and Wever studied a number of volunteers that agreed to spend time cut off from the outside world in a disused WWII bunker in Munich. After a month or so cut off from external cues they adopted a 25-hour daily cycle. This shows the importance of natural light for this circadian rhythm.
Use of case studies and small samples: Studies of the sleep/wake cycle tend to involve small groups of participants (Aschoff and Wever) or individuals (Siffre). The people involved may not be representative of the wider population and this limits the extent to which generalisations can be made.
Methodological issues – poor control: Some have criticised this research since it is so artificial. In particular, they object to the use of strong artificial light by the participants. On waking the volunteers such as Siffre switch on lights, which are likely to artificially re-set the body clock. This means there was poor control in these studies as it was assumed that only natural light would influence the biological rhythms. However, research by Czeisler showed that dim artificial light could adjust circadian rhythms to between 22 – 28 hours. This means that the results of the original studies may lack validity and the sleep/wake cycle may vary more than Siffre suggested. This may also impact on daily life as artificial light from phones; ipad etc. may have an impact on circadian rhythms when they are used at different times of the day.
Practical application to drug treatments- Circadian rhythms co-ordinate a number of the body’s basic processes such as heart rate, digestion and hormone levels. This in turn has an effect on pharmacokinetics, the action of drugs on the body and how effectively they are absorbed and distributed. Research into Circadian rhythms has revealed that there are certain peak times during day or night when drugs are likely to be at their most effective. For example, the risk of heart attack is greatest in early morning so drugs can be taken at night, but not released until the time they will be most effective. This has led to the development of guidelines about the timing of drug dosing for anticancer, cardiovascular, respiratory drugs in order to maximise their efficiency.
Individual differences- There are considerable differences between individuals when it comes to circadian rhythms and this further complicates the generalisation of findings from studies. The most noticeable being the larks/owls division; larks being morning types that prefer to rise and go to bed early and owls preferring to rise and go to bed later. Typically, when studied larks seem to be clock advanced having rhythms about two hours ahead of owls. There are also age differences in the sleep/wake cycle with teenagers having a circadian rhythm that started two hours after those of adults explaining why they find it difficult to focus in the morning as their body still need sleep. This means that there may be innate differences in circadian rhythms that researchers should focus on in their investigations.
The consequences of disrupted rhythms
Practical application to shift work- Knowledge of circadian rhythms has given researchers a better understanding of the adverse consequences that can occur as a result of their disruption. Shift work can result in fatigue, sleep disturbance, digestive problems, lack of concentration, memory loss and mood swings. Shift work involves prolonged conflict between internal clocks and external stimuli. As a result, during the day when metabolism etc. is at its peak the person is expected to sleep. At night when body temperature is low the person is expected to be working. This situation is often compounded by the person reverting to ‘normal’ sleep/wake cycles at the weekend and shifts altering from one week to the next.
As a result, the person never adapts to a new rhythm, leaving their biorhythms in a permanent state of desynchronisation. It is estimated that 20% of Western employees work shifts. In the very least this can result in reduced productivity and reduced employee morale. In extreme cases it can have catastrophic consequences. Major disasters such as Chernobyl and Three-mile Island, Bhopal (explosion at a chemical plant in India), have occurred in the early hours of the morning and been attributed to tiredness. Additionally on the roads in Britain there are a disproportionately high number of fatal accidents in the early hours of the morning In addition to accidents and disasters there are also health risks associated with regular shift work. These include increased risk of heart disease and digestive disorders and regular tiredness. Twenty per cent of shift workers report falling asleep whilst at work. This clearly has implications both for safety and for productivity and efficiency (potential economic implication). Research by Tilley and Wilkinson suggests that daytime sleep is shorter than night-time sleep which produces lower levels of energy and has implications if the person has to be active during the night.
Another issue that people experience when working shift patterns is that their biological rhythms are synchronised differently than their family, which can cause considerable social disruption. People who work hours that are different to their family and friends find it difficult to spend quality time with them.
Endogenous pacemakers
Endogenous pacemakers or ‘internal body clocks’ regulate biological rhythms such as regular times of sleep. They are rhythms that are from the internal bodily systems although these can be affected by the environment.
Endogenous pacemakers in the sleep-wake cycle: The suprachiasmatic nucleus (SCN) is the most important endogenous pacemaker. It is one of the primary endogenous pacemakers in mammalian species and is influential in maintaining circadian rhythms such as the sleep/wake cycle. Nerve fibres connected to the eye cross in an area called the optic chiasm on their way to the visual area of the cerebral cortex and SCN receives information about light directly from this structure. This continues even when our eyes are closed, enabling the biological clock to adjust to changing patterns of daylight whilst we are asleep. The SCN passes the information on day length and light that it receives to the pineal gland. During the night the pineal gland increases production of melatonin – a chemical that induces sleep and is inhibited during periods of wakefulness.
Exogenous zeitgebers:
Exogenous zeitgebers are cues from the environment that play an important role in regulating time and hence the circadian rhythm in humans.
Exogenous zeitgebers such as light synchronise our internal body clock with the outside world. In this way the endogenous pacemaker and exogenous zeitgeber work together to make sure we are awake and alert during the day and sleep at night. The SCN is reset every morning by light (probably the most important zeitgeber in relation to the sleep/wake cycle) but there is also evidence that other zeitgebers can help reset the body clocks such as temperature and social cues.
1. Light appears to be a crucial zeitgeber in humans and can reset the body’s main endogenous pacemaker, the SCN. It therefore plays a role in maintaining the 24-hour sleep/wake cycle. Light also has an indirect influence on other key processes in the body involved in the control of key functions such as hormone secretion and blood circulation.
2. Social cues. In human infants the initial sleep/wake cycle is very random. The schedule and routine imposed by parents has a key influence on the circadian rhythms that develop. This includes mealtimes and bedtimes. Research also suggests that adapting to local times for eating and sleeping when travelling is an effective way of entraining circadian rhythms and beating jet lag when travelling long distances.
Evaluation of the effect of endogenous pacemakers and exogenous zeitgebers on the sleep/wake cycle.
Supporting evidence for the importance of endogenous pacemakers. The influence of the SCN has been demonstrated in studies involving animals. Decoursey et al- The SCN connections were destroyed in the brains of 30 chipmunks that were then returned to their natural habitat and observed for 80 days. The sleep/wake cycle of the chipmunks disappeared and by the end a significant number of the chipmunks had been killed by predators (perhaps because they were awake and vulnerable when they should have been asleep). Ralph et al- The SCN was removed from genetically abnormal hamsters that had a circadian rhythm of 20 hours. They then transplanted the SCN cells into normal hamsters which had no such abnormality and functioned on the normal; 24-hour cycle. Following the transplant, the circadian rhythm of the transplant hamsters shortened to 20 hours. This suggests the SCN is pivotal in regulating the internal body clock.
Ethics in animal studies: Animals are often exposed to considerable harm and as is the case with DeCoursey’s study the chipmunks were put into a dangerous situation when they were returned to their natural environment. It is a matter of debate whether what we learn from investigations such as this justifies the procedures involved.
Supporting evidence for the role of exogenous zeitgebers. When Siffre returned from staying underground with no clocks or natural light, he believed the date to be a month earlier than it actually was. This suggests that his 24-hour sleep wake cycle had increased due to the lack of external cues resulting in his body clock changing. This highlights the impact that external factors have on circadian rhythms.
Validity: Much of the research can be criticised for lacking external validity. It is often carried out in artificial conditions and therefore the resulting behaviour could be also false. Monitoring sleep can also have an effect on the sleep patterns of the participants. This means that the sleep patterns recorded could be a by-product of being monitored rather than the effect of the zeitgeber/pacemaker.
Ultradian Rhythms
Ultradian rhythms are biological rhythms that last less than 24 hours and occur more than once a day. One of the most researched ultradian rhythms is the sleep cycle. Psychologists have identified five distinct stages of sleep that altogether span approximately 90 minutes – this is a cycle that continues throughout the night. Each stage is characterised by a different level of brainwave activity, which can be monitored using EEG.
A complete sleep cycle goes through four stages of NREM (Non Rapid Eye Movement) sleep before entering REM (stage 5) and then repeating. Research using EEG has highlighted distinct brainwave patterns during the different stages of sleep.
● Stages 1 and 2 are ‘light sleep’ stages. During these stages brainwave patterns become slower and more rhythmic, starting with alpha waves and progressing to theta waves.
● Stages 3 and 4 are ‘deep sleep’ or slow wave sleep stages, where it is difficult to wake someone up. These stages are associated with slower delta waves.
● Finally stage 5 is REM (dream) sleep. Here the body is paralysed (to stop the person acting out their dream) and brain activity resembles that of someone who is awake.
On average the entire cycle repeats every 90minutes and a person can experience up to five full cycles in a night.
This cycle repeats throughout the night, however, we spend most of the first half of the night in deep sleep (slow wave or NREM), and most of the second half in REM sleep. A typical night’s sleep takes you from stage 1 to 4 then back to 2 and finally into REM. There are a number of similar cycles during the daytime too. Sometimes these are referred to as diurnal. Examples include eating (approximately every four hours), smoking and drinking caffeine (in those addicted), and urination.
Evaluation of Ultradian Rhythms
Supporting evidence: Dement and Kleitman (1957) conducted a study, the aim was to investigate brain activity throughout night-time sleep. Method: Nine participants were studied (seven males and two females). Participants ate normally (excluding coffee and alcohol) and arrived at the laboratory just before their normal bedtime. They went to sleep with electrodes attached beside the eyes (EOG) and on the scalp (EEG) to record brain activity and eye movement. Findings: Everyone had periods of REM throughout the night. Participants frequently described dreams when woken in REM but rarely did so from NREM sleep. In NREM awakenings, participants tended to describe feelings but not specific dream content. Eye movement patterns were related to dream content, e.g. vertical movements in a dream about ladders. Conclusion: There a number of stages in the sleep cycle. Dreaming is reported from REM but not NREM sleep, participants can judge the length of their dream duration and REM patterns relate to dream content.
Small sample size. As with most sleep research, sample size is very small making generalisations difficult, particularly when there are such great individual differences between participants.
Sleep laboratories are very artificial settings. The participants’ pre-sleep routine is very different to at home, they are in unfamiliar surroundings and covered with a plethora of electrodes and wires. They also know that they’re being observed.
Objective measurement. However, sleep studies like this do allow for physiological measurements, which are objective and replicable. Unfortunately, self-report techniques are just the opposite, subjective and non-verifiable. Given the fragile nature of dreams self-report of these must be seen as particularly unreliable.
Infradian Rhythms
Infradian rhythms last longer than 24 hours. An example is the menstrual cycle, which is dictated by the endocrine system. However, this rhythm is not imposed purely by the release of hormones. It is suggested that zeitgebers such as light and odours are also involved. Another example of an infradian rhythm in the animal world is hibernation which is an annual rhythm. A human example would be SAD (Seasonal Affective Disorder).
Seasonal Affective Disorder (SAD)
Although it is apparently normal for most people to feel more cheerful in the summer months than in winter, a small number of people suffer an extreme form of this that appears to be related to the lack of bright light in the winter months. Light levels, are detected by receptors in the eye and influence levels of melatonin and serotonin which is implicated in mood. At night low light levels stimulate the production of melatonin, this is what triggers sleepiness. Therefore, you would expect the lower light levels of the winter months to have a similar affect.
In areas where light levels are exceptionally low for prolonged periods, such as the Polar Regions, you would expect the effects to be particularly noticeable. Terman (1988) found that SAD was five times more common in New Hampshire, a northern state of the USA, than in Florida.
Research into SAD: Terman et al (1998)
The symptoms of SAD can be reduced in polar regions by sitting patients in front of very bright artificial lights for at least one hour per day. This lowers the levels of melatonin in the bloodstream which in turn reduces the feelings of depression. The precise mechanism for this is still unclear. Drugs used to treat depression such as Prozac and other MAOIs (monoamine oxidase inhibitors), appear to work by altering serotonin levels.
Terman et al (1998) researched 124 participants with SAD. 85 were given 30-minute exposure to bright light, some in the morning, and some in the evening. Another 39 were exposed to negative ions (a placebo group).
Findings: 60% of the am bright light group showed significant improvement compared to only 30% of those getting light in the evening. Only 5% of the placebo group showed improvement.
Conclusions: The researchers concluded that bright light administered in this way may be acting as a zeitgeber and resetting the body clock in the morning. Research into SAD has led to effective treatments such as light therapy suggesting that the theory has some validity.
The menstrual cycle
This is a cycle that lasts about one month, so therefore an infradian rhythm. Like other rhythms, the menstrual cycle appears to be under the influence of both internal (endogenous) mechanisms, and external zeitgebers.
Endogenous control- The cycle is under the internal control of hormones, particularly oestrogen and progesterone, secreted by the ovaries. These cause a number of physiological changes within the body including the release of at least one egg from the ovaries and the thickening of the lining of the womb (uterus), in preparation for the arrival of the egg. If the egg is not fertilised, then the lining of womb is shed and menstruation occurs. The contraceptive pill mimics the effects of pregnancy and cons the body into ceasing production of further eggs.
External control (zeitgebers)- It has long been known that the menstrual cycle can be influenced by external factors, most notably by living with other women. The most likely mechanism for this is by the action of pheromones; chemical substances similar to hormones but which carry messages between individuals of the same species.
Research into the Menstrual Cycle: McClintock and Stern (1988)
Armpit pheromones and the McClintock effect: Martha McClintock (1971) was the first to notice possible synchronisation of menstrual cycles amongst women living in close proximity. In 1988, McClintock & Stern published their findings of a 10-year longitudinal study into external control of the menstrual cycle. They had followed 29 women (aged 20-35) who had had a history of irregular menstrual cycles. Sweat samples from the armpits of 9 of the women had been collected, sterilised and dabbed onto the upper lip of the other twenty. Findings: On 68% of occasions the recipients of the sweat donation had responded to the pheromones. Armpit compounds collected from the nine donors in the later phase of the menstrual cycle shortened the cycles of 20 recipients. Conversely, when the nine donors were in the early phase, the compounds lengthened the cycles of the same 20 recipients. Conclusion: This study shows that the menstrual cycle of a woman can be altered by communication via pheromones.
via pheromones.
Evaluation of McClintock
The Effects of pheromones can help to explain menstrual synchronicity in situations where women live together, such as at university or in nunneries. The communication via pheromones explains it as there must be something in the shared environment that acts as a zeitgeber. Although how closely women live together and for what length of time for synchronicity to occur is not clear and still requires further research.
Evolutionary advantages Bentley (2000) believed that synchronisation between women living in close proximity would ensure that the women would conceive and give birth at similar times. This would be beneficial since they could share breast feeding, a behaviour observed in other species. However, the validity of the evolutionary perspective has been questioned. If there were too many females in synchrony this would produce competition for the highest quality males, which would lower the fitness of potential offspring. Therefore avoiding synchrony would be a more adaptive evolutionary strategy.