Deformities of the Hand
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
20 Terms
Heberden’s is DJD of
DIPs, calcified spurs on articular cartilage of bone; thickening of jt capsule
Bouchard’s nodes is less common, but is defined as DJD of
PIP joints
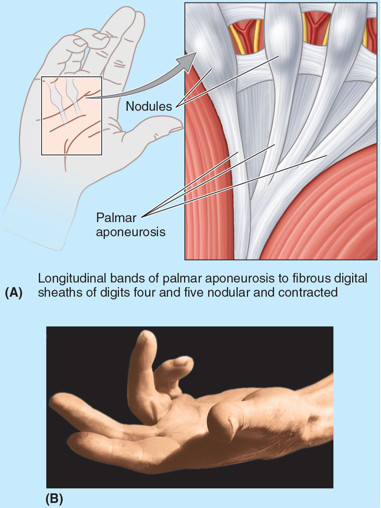
Dupuytren’s contracture is a contracture of the palmar fascia which causes a
flexion deformity in 4th & 5th digits (also 3rd in severe cases)
Dupuytren’s contracture prevalence/population
Usually occurs >40 y/o
Men > women
Genetic Component
Surgical manipulation: Collagenase clostridium histolyticum
Swan neck deformity includes hypermobility of
PIP & volar plate injury
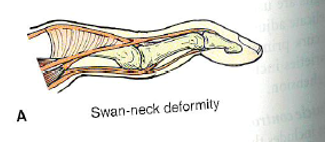
Swan neck deformity shows a bow stringing of lateral bands due to
contracture of intrinsic muscles: Palmar interossei
Swan neck deformity presentation is
PIP hyperextended
DIP & MCP flexed
Swan neck deformity etiology
RA, neurovascular lesion

Boutonnière deformity is due to rupture of the
central slip of extensor hood, seen w/ Trauma or RA
Boutonnière deformity presentation
Extension of MCP & DIP
Flexion of PIP
Mallet finger is an avulsion fx of the
extensor tendon
mallet finger presents w/ no active extension of
DIP joint is possible
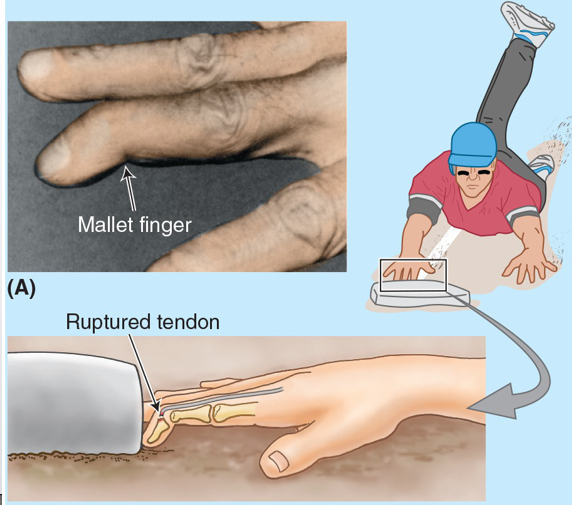
Mallet finger MOI:
jamming a finger in bball or volleyball (Iceman Jason)
De Quervain’s Tenosynovitis definition
Stenosing tenosynovitis of 1st dorsal extensor compartment
De Quervain’s Tenosynovitis anatomy involved
APL/EPB: share 1st dorsal ext compartment (apple & peanut butter)
De Quervain’s Tenosynovitis clinical presentation
Thumb activity ↑ pain
Tenderness & edema over/distal to radial styloid
Pain produced w/ resisted thumb ext & abduction
Pain w/ active/passive ulnar deviation w/ thumb flexed ((+) Finkelstein test)
De Quervain’s Tenosynovitis differential diagnosises
radial nerve entrapment
ligamentous
scaphoid/lunate jt dysfunction
C-spine
De Quervain’s Tenosynovitis diagnostic techniques
Finkelstein Test (+)
ULTT - assess for involvmnt of superficial radial n: It passes over snuff box, examine for sensory changes

Trigger Finger pathology of Flexor tenosynovitis presents w/ a thickening/fibrosis of a tendon, synovial sheath, &/or annular pulley. Flexor tendon can’t glide normally w/in sheath due to a thickening or nodule that catches at the
1st annular pulley (A-1). Nodule may be palpable
The finger may locked in a flexed position
Differential Diagnosis of Wrist & Hand. 1st Rule out proximal contributions (C-spine). Additionally investigate the
MOI: Traumatic Vs atraumatic
Neurology: Altered Sensation, Isolated weakness in myotomal or peripheral nerve patterns, reflexes
Pain location: What structures live in the area
Lifestyle & occupations considerations