Case 6: Ron Chen Pt 2 - Polyneuropathy
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
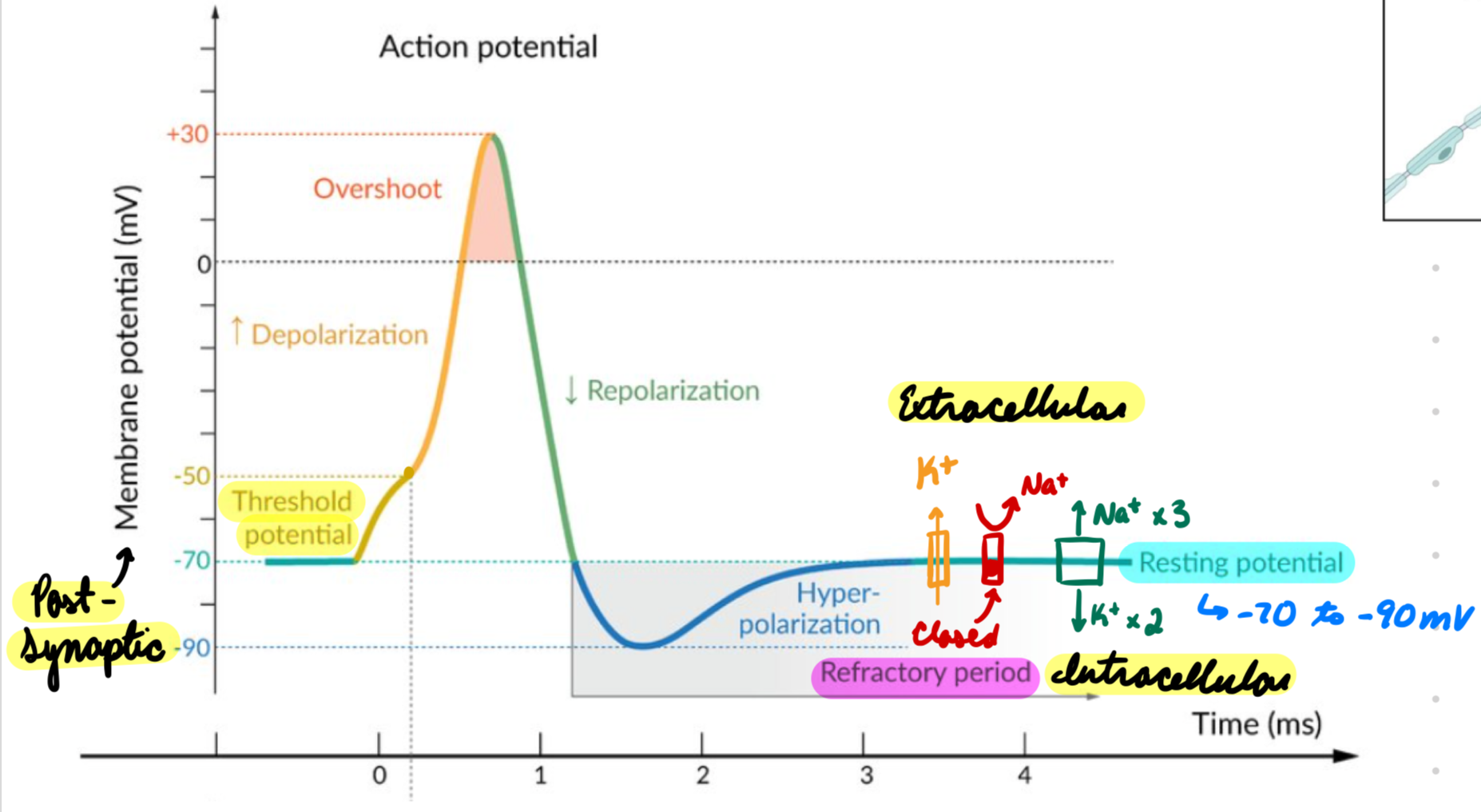
Excitable Cells: Resting Potential
Membrane potential at rest
-70 to -90 mV
Maintained by diffusion potentials
Leaky K+ Channels: K+ move out
Na+/K+ ATPase:
Transport 3 Na+ out
Transport 2 K+ in
Voltage-Gated Na+ Channels: Closed at rest
Keep Na+ extracellular
Excitable Cells: Post-Synaptic Potential
Receive signal from pre-synaptic neuron
Pre-synaptic signal = Release NTs into synaptic cleft = Bind receptors on post-synaptic membrane = Propagate signal
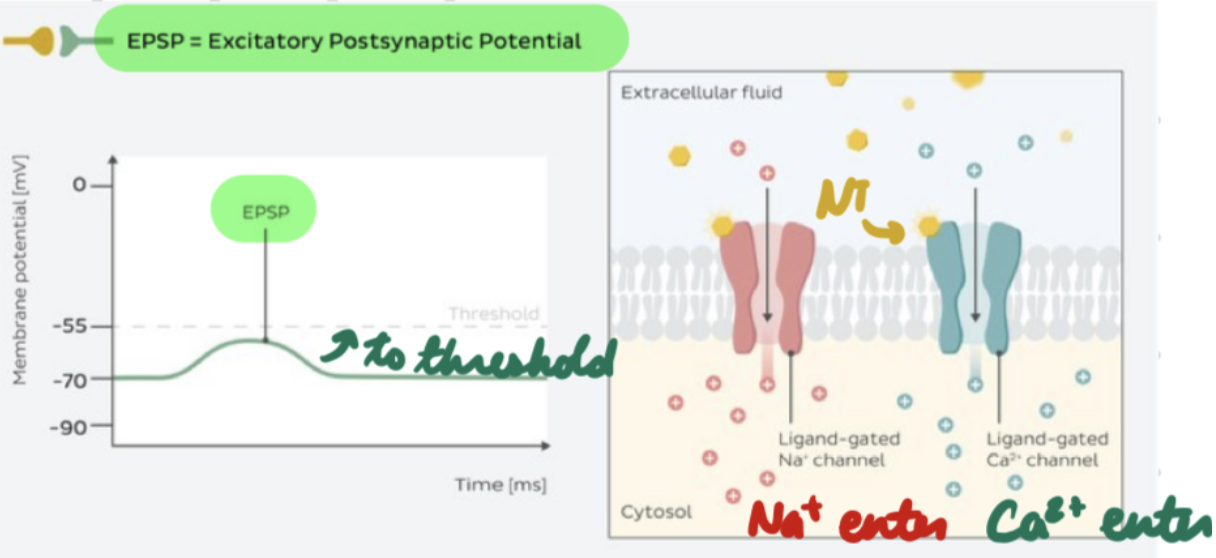
Excitatory post-synaptic potential (EPSP)
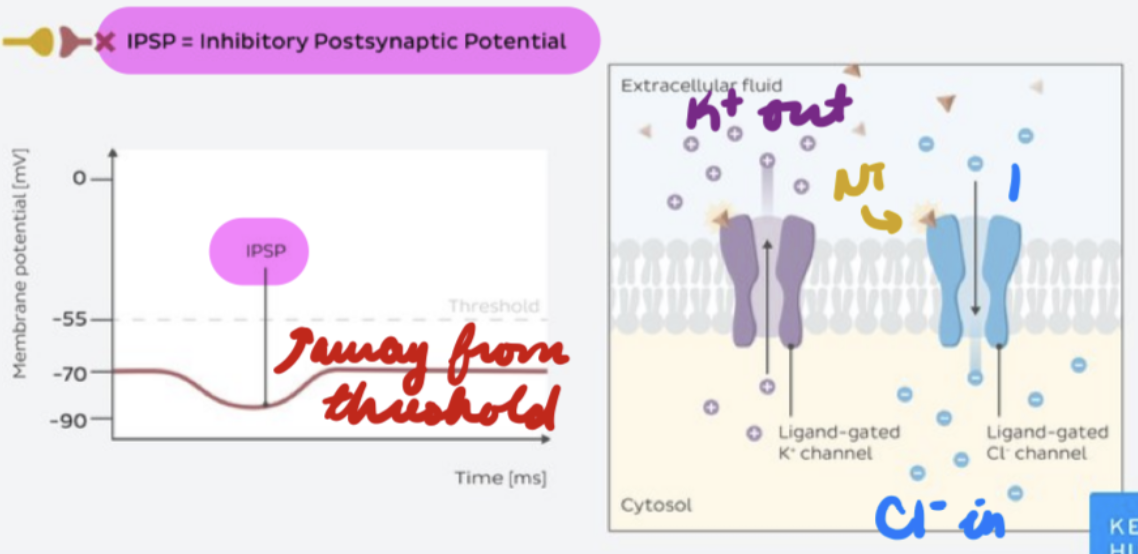
Inhibitory post-synaptic potential (IPSP)
Excitable Cells: EPSP
Depolarizing potential
Post-synaptic receptors open = Cations enter
Summation = Post-synaptic neuron reach threshold potential = AP firing
NTs: ACh, NMDA, dopamine, glutamate
Ex: NMJ, nicotinic synapses, NMDA synapses
Excitable Cells: IPSP
Hyperpolarizing/depolarizing potential
Post-synaptic receptors open = Anions enter
Summation = Post-synaptic neuron move away from threshold potential = Decrease AP firing
NTs: GABA, glycine, dopamine, serotonin
Ex: GABAergic synapses, glycine synapses
Excitable Cells: Action Potentials
Threshold potential = Voltage-gated Na+ channels open = Na+ in = Depolarize membrane
APs: Myelinated Neurons
Saltatory conduction
Generation: Non-myelinated membrane areas (Nodes of Ranvier) ≥ Threshold potential
Propagation: Fast
Note of Ranvier depolarization = Open voltage-dependent Na+ channels at next node of Ranvier = Depolarization skips/jumps along cell membrane → AP
APs: Unmyelinated Neurons
Continuous conduction
Generation: Any membrane area ≥ threshold potential
Propagation: Slow
Membrane depolarization = Open voltage-dependent Na+ channels in adjacent areas = Depolarization migrate along cell membrane → AP
APs: Refractory Period
Na+ channels close = Membrane hyperpolarization = Prevent signal backpropagation
Polyneuropathy: Description
Peripheral nerve damage
Length-Dependent: Affect neurons with longer axons first
Types:
Axonal: Pathology in neuron axons
Schwann Cells/Myelin Sheath: Pathology affecting Schwann cells/myelin sheath
Polyneuropathy: Epidemiology
Risk factors…
DM
Alcohol use disorder
Chemotherapy
Nutritional deficiencies
Obesity
Autoimmune disorders
Polyneuropathy: Etiology
Axonal:
DM
Alcohol use disorder
Leprosy
Borreliosis
HIV
GBS
Chemotherapy
Cisplatin
Doxorubicin
Myelin:
Chronic inflammatory demyelinating polyneuropathy
Hereditary motor + sensory neuropathies (HMSN)
Charco-Marie-Tooth Disease: Defect in axon/myelin sheath protein function/structure
GBS
Toxins
Diphtheria
Amiodarone
Other Causes:
Idiopathic
Toxins
Heavy metals (lead, arsenic)
Inflammatory
Vasculitis
Connective tissue disorders
Infectious
Herpes
Polyneuropathy: Axonal Pathophysiology
Axon degeneration = Axon/soma injury = Axon + myelin sheath degeneration distal to injury (Wallerian degeneration)
Neurons with longer axons targeted first
Greater metabolic needs = Decrease metabolic trafficking down axon = Difficulty repair from injury
Distal → Proximal symptoms
Polyneuropathy: Schwann Cell + Myelin Sheath Pathophysiology
Abnormal Schwann cell function = Segmental demyelination
Generalized muscle weakness
Distal > proximal
Polyneuropathy: Connective Tissue + Vascular Pathophysiology
Inflammation = Increase capillary permeability = Edema
Polyneuropathy: Clinical Presentation
Symmetrical distal sensory loss
Glove-and-stocking pattern
Neuropathic pain
Burning-Foot syndrome: Burning pain, paresthesias, hyperhydrosis
Paresthesias
Motor weakness
Muscle atrophy (stork legs)
Sensory ataxia
Loss of sensation (proprioception)
Affect postural reflexes
Decreased deep tendon reflexes
Polyneuropathy: Investigations
Blood tests
Nerve conduction studies
EMG
Biopsy
Genetic testing
Polyneuropathy Investigations: Blood Tests
CBC
Anemia
CMP
Electrolytes
Serum glucose (DM)
Vit B12 (low)
TSH (thyroid disease)
Heavy metal
Lead
Ethanol level
Serology
Hep B/C
HIV
Lyme disease
Polyneuropathy Investigations: Nerve Conduction Studies
Axonal: Normal impulse conduction velocity + decreased response amplitude
Myelin: Decreased impulse conduction velocity + normal response amplitude
Polyneuropathy Investigations: EMG
Spontaneous electrical activity (fibrillation potentials)
Decreased interference pattern (decreased electrical activity density)
Polyneuropathy Investigations: Biopsy
Not routine
Sural nerve: Sensory nerve in leg
Skin
Polyneuropathy: Treatment
Treat underlying cause
Nonpharmacological
Pharmacological
Polyneuropathy Treatment: Nonpharmacological
Symptom management
Refer patients to…
Podiatry: Foot care
Physical therapy: Exercises
Occupational therapy: Home assessment + modification
Polyneuropathy Treatments: Pharmacological
First-Line:
Tricyclic antidepressants (TCAs)
SNRIs
Gabapentinoids
Topical analgesic: Adjuvant for pain
Tramadol: Treatment failure
Polyneuropathy Treatment: TCAs
MOA: Inhibit norepinephrine + serotonin (less) reuptake in synaptic cleft = Increase inhibitory pathways in spinal cord = Decrease pain transmission
Ex: Amitriptyline
Polyneuropathy Treatment: SNRIs
MOA: Same as TCAs
Ex: Duloxetine
Polyneuropathy Treatment: Gabapentinoids
MOA: Bind voltage-gated Ca2+ channels = Decrease excitatory NT (glutamate) release = Inhibit pain signal transduction
Polyneuropathy Treatment: Tramadol
MOA:
Weak opioid agonist
Inhibit serotonin + norepinephrine reuptake
Polyneuropathy: Complications
Impaired balance = Increase fall risk
Charcot Joint: Neuropathic arthropathy
Bone + joint destruction in foot + ankle