Sacrum, Coccyx, SI joints positioning notes/ demo
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
SI joints views
AP axial, RPO and/OR LPO
AP axial SI joint technique
90 kVp, 14 mAs, center cell
SI joints & Sacrum/coccyx- breathing/ SID
suspended expiration
40” SID
Ap axial SI joint overview
Collimation
12×10 CW
Centering
1.5” superior to symph & down the MSP
Males- 30 cephalad angle
Females- 35 cephalad angle
AP SI joint- angle for males
30 cephalad
AP SI joint- angle for females
35 cephalad
AP SI joints- evaluation criteria
lumbosacral junction & sacrum
open intervertebral disk space between L5 & S1
both SI joints
merrill’s collimation for SI joints
10×8 CW
merrills breathing for SI joints & sacrum/coccyx
suspended RESPIRATION
merrills note for AP SI joints
images can be taken prone if pt cannot tolerate lying on back
central ray MUST be angle CAUDAD
Too much angle- AP SI joint
pubic bone overlies SI joints
Too little angle- AP SI joints
SI joints are foreshortened & closed off
w/ proper angle- AP SI joints
pubic bone overlies distal coccyx
RPO & LPO SI joints- technique
90 kVp, 16 mAs, center cell
RPO & LPO SI joints: overview
Collimation
6×10 LW
Patient position
25-30 degree oblique (side of interest is UP)
Centering
perpendicular to IR & 1” medial to elevated ASIS
Marker placement
lateral on ELEVATED SIDE
RPO & LPO SI joints- what joint is demonstrated?
Joint FARTHEST FROM THE IR (ELEVATED SIDE)
RPO & LPO SI joints- evaluation criteria
open SI joint space FARTHEST from IR w/ minimal overlapping of ilium & sacrum
joint centered
Under rotation-RPO & LPO SI joints
iliac tuberosity is overlapping sacral ala/ sacrum is sitting in inlet (like AP)
joint is closed off at
over rotation RPO & LPO SI joints
sacrum is under pelvis, can see scotty dogs, SI joint closed off at
proper rotation RPO & LPO SI joints
border of sacrum just inside the inlet
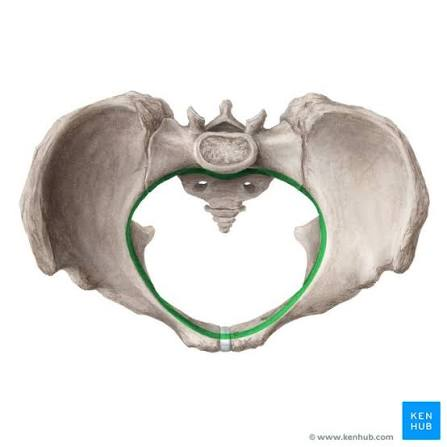
picture of…..
inlet of pelvis
SI joint special view: RAO/ LAO purpose
SI joint CLOSEST to IR is visualized
SI joint special view: RAO/ LAO summary
Pt position
prone, side of interest rotated away from table 25-30 degrees
Marker placement
mark lateral on side CLOSEST TO TABLE
Sacrum/coccyx views
AP sacrum/ coccyx & Lateral sacrum/ coccyx
RH note for sacrum coccyx
if physician orders only a sacrum or only a coccyx, DO BOTH
bladder stim replacement= DO BOTH
merrills recommends what for sacrum coccyx
pre procedure bowel prep
AP axial Sacrum technique
90 kVp, 14 mAs, center cell
AP axial Sacrum- overview
Collimation
10×12 LW
Centering
angled 15 cephalad
center 2” superior to symph (bisect symph & asis)
Marker placement
bottom!
AP axial Sacrum evaluation criteria
sacrum centered & seen entirely (base to apex)
sacrum free of foreshortening, w/ sacral curve straightened (why we angle)
no rotation of sacrum, as demonstrated by symmetric alae & spinous processes down middle (sacrum is in line w/ symph)
merrills recommendation for sacrum & coccyx AP- pt position
place support under patient’s knees
merrills note for Ap sacrum when patient is prone
angle 15 CAUDAD through sacral curve
on a good AP sacrum, the pubic bone lays…
on top of coccyx
too much angle AP axial Sacrum
pubic bone overlaps sacrum
not enough angle AP axial Sacrum
sacrum looks foreshortened & pubic bone lays distal end of coccyx
how to note rotation AP axial Sacrum
that side is flatter & obturator foramen isn’t oval & nicely opened
(coccyx goes opposite way that it is rotated)
AP coccyx- technique
85 kVp, 14 mAs, center cell
AP coccyx- overview
Collimation
6×8 LW
Centering
angled 10 caudad (to get coccyx free of superimposition)
then, center 2” superior to symph (bisect symph & ASIS)
Marker placement
bottom
note for marker placement on AP sacrum to ap coccyx
place marker where cross hair is on AP sacrum, so when you add angle tot he tube, you know where to center again
AP coccyx-evaluation criteria
coccyx centered & seen entirely
coccygeal segments not superimposed by pubic bones
no rotation of coccyx, as demonstrated by distal segment in line with symph
merrills note for AP coccyx- if patient is prone
angle 10 degrees cephalad through coccyx
AP coccyx- not enough angle
pubic bones are over coccyx
sacrum left lateral- technique
96 kVp, 45 mAs, center cell
sacrum left lateral overview
Collimation
10×12 LW
Centering
perpendicular & directed 3.5” POSTERIOR to ASIS
Marker placement
left marker ANTERIOR
sacrum left lateral- evaluation criteria
sacrum (L5/S1 to coccyx)
closely superimposed posterior margins of ischia & ilia, demonstrating no rotation
merrills note for sacrum left lateral & coccyx left lateral
place lead rubber absorbed behind patient to absorb scatter
recommends support under waist to keep spine HORIZONTAL to IR
rotation on sacrum left lateral
femoral heads/sciatic notches are not stacked/superimposed
trick going from lateral sacrum to lateral coccyx
bring centering down 2”
coccyx left lateral- technique
85 kVp, 40 mAs, center cell
coccyx left lateral- overview
Collimation
6×8 LW
Centering
perpendicular & 3.5” posterior & 2” inferior from ASIS
Marker placement
left anteriorly
coccyx left lateral- evaluation criteria
coccyx
closely superimposed posterior margins of the ischia & ilia, demonstrating no rotation
SPECIAL VIEW: sacrum & coccyx technique
96 kVp, 45 mAs, center cell
SPECIAL VIEW: sacrum & coccyx overview
Collimation
10×12 LW
Centering
perpendicular & 3-4” POSTERIOR to ASIS
(may need to be moved 1” inferior to ASIS to include all anatomy)
SUSPENDED RESPIRATION