week 37 - acute surgical problems in children
0.0(0)
Studied by 1 personCard Sorting
1/22
There's no tags or description
Looks like no tags are added yet.
Last updated 4:05 PM on 7/8/26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
1
New cards
Physiological differences between infants and adults
* children have a higher basal metabolic rate and higher oxygen demand
* children have a higher blood volume to body weight ratio but the total blood volume is very small (so surgery must make sure to not cause a lot of blood loss)
* Fluid deficiency and electrolyte imbalances occur rapidly in children because each compartment has such a small fluid volume
* paediatric fluid requirements are relatively higher because the kidneys the kidneys have less concentrating ability and obligatory urine output is greater
* Faecal fluid losses are higher especially < 2 y/o → dehydration and electrolyte imbalances occur very fast in severe diarrhoea of children
* Hypoglycaemia readily occurs because a baby’s glucose stores are meagre
* adrenergic responses to trauma and response also increase glucose requirements
* Likely to occur when a baby is fasted before surgery but not given IV dextrose or when a blood transfusion temporarily replaces IV dextrose
* All small children undergoing surgery need close monitoring of blood glucose to prevent hypoglycaemic brain damage
* Temperature regulation in infants is less robust and hypothermia is a real hazard
* Infants have a large SA:V and poort vasomotor control of skin vessels + unable to generate heat by shivering
* These temperature differences are more obvious in premature babies
* A controlled heated environment is necessary for operating on and nursing newborn infants (< 1 kg → 34.5-35.5 degrees, > 3 kg → 31.5-35.4) keep them insulated, IV fluid and skin cleansers are warmed and anaesthetic gases are humidified and warmed
* Liver function is immature in the newborn (seen by relatively high bilirubin levels etc) + reduced ability to detoxify analgesic drugs (also a lot of drugs readily cross the BBB and may cause cerebral side effects) + reduced prothrombin production (which is why prophylactic vitamin K is given after birth)
* Infection can be rapidly fatal in small babies especially if premature or SGA
* children have a higher blood volume to body weight ratio but the total blood volume is very small (so surgery must make sure to not cause a lot of blood loss)
* Fluid deficiency and electrolyte imbalances occur rapidly in children because each compartment has such a small fluid volume
* paediatric fluid requirements are relatively higher because the kidneys the kidneys have less concentrating ability and obligatory urine output is greater
* Faecal fluid losses are higher especially < 2 y/o → dehydration and electrolyte imbalances occur very fast in severe diarrhoea of children
* Hypoglycaemia readily occurs because a baby’s glucose stores are meagre
* adrenergic responses to trauma and response also increase glucose requirements
* Likely to occur when a baby is fasted before surgery but not given IV dextrose or when a blood transfusion temporarily replaces IV dextrose
* All small children undergoing surgery need close monitoring of blood glucose to prevent hypoglycaemic brain damage
* Temperature regulation in infants is less robust and hypothermia is a real hazard
* Infants have a large SA:V and poort vasomotor control of skin vessels + unable to generate heat by shivering
* These temperature differences are more obvious in premature babies
* A controlled heated environment is necessary for operating on and nursing newborn infants (< 1 kg → 34.5-35.5 degrees, > 3 kg → 31.5-35.4) keep them insulated, IV fluid and skin cleansers are warmed and anaesthetic gases are humidified and warmed
* Liver function is immature in the newborn (seen by relatively high bilirubin levels etc) + reduced ability to detoxify analgesic drugs (also a lot of drugs readily cross the BBB and may cause cerebral side effects) + reduced prothrombin production (which is why prophylactic vitamin K is given after birth)
* Infection can be rapidly fatal in small babies especially if premature or SGA
2
New cards
Fluid depleted children are often…
Lethargic or drowsy and may even be comatose
Eyes and anterior fontanelle may be sinker but skin turgor is not lost
Tachycardia is usual but hypotension is a late sign because of compensatory mechanisms
Urine output is likely to be low
Eyes and anterior fontanelle may be sinker but skin turgor is not lost
Tachycardia is usual but hypotension is a late sign because of compensatory mechanisms
Urine output is likely to be low
3
New cards
Abdominal emergencies in the newborn
1. Intestinal obstruction
4
New cards
Detectable abnormalities that will need surgical corrections soon after birth include…
Diaphragmatic hernia, abdominal wall defects and congenital pulmonary airway malformations etc
Seen in the dating scan (12 weeks) and anomaly scan (20 weeks)
Seen in the dating scan (12 weeks) and anomaly scan (20 weeks)
5
New cards
Intestinal obstruction
* is the underlying phenomenon in most neonatal abdominal emergencies
* Most causes are not detectable by antenatal US
* May result in maternal polyhydramnios
* Presents with vomiting, constipation and abdominal distension (same as adults)
symptoms more specific to babies → poor feeding, failure to pass meconium and bilious vomiting
* Abdominal distension may not occur in upper GI obstruction (even in lower obstruction, sometimes it is not noticed until the baby is completely undressed)
* Meconium is passed in the first 24 hrs in 80% of babies, delay should be cause for concern
* Causes of upper obstruction → duodenal atresia and malrotation with volvulus
* Causes of lower obstruction → hirschsprung disease and meconium ileus
* (Small bowel atresia can be either upper or lower)
* Plain abdominal x rays usually confirm diagnosis
\
1. GI atresias and stenoses:
* oesophageal and duodenal atresias and anorectal malformations are true embryological abnormalities often associated with other congenital abnormalities (eg. Cardiac, vertebral or renal abnormalities are found in 40% of babies with oesophageal atresia and 30% of those with duodenal atresia have Down syndrome)
* SI bowel atresias probably result from intrauterine vascular accidents or failure of canalisation of the bowel and are rarely associated with other abnormalities
* Oesophageal atresia is in another card
* Duodenal atresia:
* web across the lumen or complete separation of the bowel ends
* Bilious vomiting
* Double bubble
* If there is no malrotation or volvulus, surgery can be delayed
surgical treatment involves formation of a duodenoduodenostomy, anastomosing the two ends of the discontinuous duodenum (gastrojejunostomy used to be done but it causes bacterial colonisation of the defunctioned loop causing failure to thrive etc)
* Jejuno ileal atresias
* similar to ^ except visible peristalsis is more likely to be seen
* High jejunal obstruction present like duodenal atresia or malrotation with bile stained vomit and a lack of gas on x ray
* Low ileal obstruction presents like meconium ileus or hirschsprung disease with failure to pass meconium, poor feeding, abdominal distension and dilated intestine on x ray
* Small bowel atresia is sometimes associated with CF → must always have a genetic screen and sweat test to exclude it
2. Midgut malrotation with volvulus
* check theme 9 for pathophysiology
* Previously well children who present acutely with sudden duodenal obstruction (eg. Bilious vomiting), particularly with signs of peritonitis, should have very urgent surgery to prevent infarction
* Short bowel syndrome is likely to occur if there is insufficient small bowel remaining after surgery
* If an older child has a history of intermittent bile stained vomiting, an upper GI contrast study can demonstrate an abnormal position of the duodenal jejunal flexure
surgery may then be needed to broaden the mesenteric base
* Most causes are not detectable by antenatal US
* May result in maternal polyhydramnios
* Presents with vomiting, constipation and abdominal distension (same as adults)
symptoms more specific to babies → poor feeding, failure to pass meconium and bilious vomiting
* Abdominal distension may not occur in upper GI obstruction (even in lower obstruction, sometimes it is not noticed until the baby is completely undressed)
* Meconium is passed in the first 24 hrs in 80% of babies, delay should be cause for concern
* Causes of upper obstruction → duodenal atresia and malrotation with volvulus
* Causes of lower obstruction → hirschsprung disease and meconium ileus
* (Small bowel atresia can be either upper or lower)
* Plain abdominal x rays usually confirm diagnosis
\
1. GI atresias and stenoses:
* oesophageal and duodenal atresias and anorectal malformations are true embryological abnormalities often associated with other congenital abnormalities (eg. Cardiac, vertebral or renal abnormalities are found in 40% of babies with oesophageal atresia and 30% of those with duodenal atresia have Down syndrome)
* SI bowel atresias probably result from intrauterine vascular accidents or failure of canalisation of the bowel and are rarely associated with other abnormalities
* Oesophageal atresia is in another card
* Duodenal atresia:
* web across the lumen or complete separation of the bowel ends
* Bilious vomiting
* Double bubble
* If there is no malrotation or volvulus, surgery can be delayed
surgical treatment involves formation of a duodenoduodenostomy, anastomosing the two ends of the discontinuous duodenum (gastrojejunostomy used to be done but it causes bacterial colonisation of the defunctioned loop causing failure to thrive etc)
* Jejuno ileal atresias
* similar to ^ except visible peristalsis is more likely to be seen
* High jejunal obstruction present like duodenal atresia or malrotation with bile stained vomit and a lack of gas on x ray
* Low ileal obstruction presents like meconium ileus or hirschsprung disease with failure to pass meconium, poor feeding, abdominal distension and dilated intestine on x ray
* Small bowel atresia is sometimes associated with CF → must always have a genetic screen and sweat test to exclude it
2. Midgut malrotation with volvulus
* check theme 9 for pathophysiology
* Previously well children who present acutely with sudden duodenal obstruction (eg. Bilious vomiting), particularly with signs of peritonitis, should have very urgent surgery to prevent infarction
* Short bowel syndrome is likely to occur if there is insufficient small bowel remaining after surgery
* If an older child has a history of intermittent bile stained vomiting, an upper GI contrast study can demonstrate an abnormal position of the duodenal jejunal flexure
surgery may then be needed to broaden the mesenteric base
6
New cards
anorectal abnormalities
* The primitive hindgut forms from the cloaca in the first few weeks of intrauterine life. A septum then descends to divide the anterior compartment (from which the urinary tract and part of the genital tract are formed) from the posterior compartment(which goes on to form the rectum and upper part of the anal canal)
* Easiest way to classify them is to group them by whether the large bowel terminates above or below the levator ani, there is usually an abnormal fistulous connection from the end of the bowel
* when the malformation is low, the ==__fistula__== opens onto the skin ==__anterior to the sphincter complex__==
a bead of meconium CAN pass through this opening → disguises the position of the anus → diagnosis is missed
* When the malformation is high, there is usually a fistula to the urethra in the male or vagina in the female (there may be a fistula to the skin)
!! patients with urethral fistula require prophylactic antibiotics to prevent UTIs
* ==__**First they said separate as above or below the levator ani but then it’s about whether it’s anterior to the sphincter complex???**__==
* UT malformations and lower vertebral anomalies are commonly associated with anorectal abnormalities and should be sought
* In suspected anorectal abnormalities, the perineum is carefully examined for a fistula. If one is not found it is worth waiting 24 hours and then examining the perineum under anaesthesia for one
If one is not found, the anomaly is treated as high and a colostomy is performed as a first stage
* *Treatment depends on the level of the distal pouch. In low lesions, the puborectalis muscle is well formed and a relatively simple operation on the perineum may be sufficient. An anoplasty is performed to increase the calibre of the fistula and the fistula is moved to open within the sphincter complex. Babies who become unwell, or have high lesions , are likely to need a colostomy in the first instance. This rescue procedure allows the baby to feed and empty the bowel. This is followed by complex surgical reconstruction later, involving mobilising the bowel end and reconstructing a sphincter mechanism around it. Long-term faecal continence and bowel and bladder control is imperfect after surgery in many children with high or low anomalies, and careful follow up is needed.*
* Easiest way to classify them is to group them by whether the large bowel terminates above or below the levator ani, there is usually an abnormal fistulous connection from the end of the bowel
* when the malformation is low, the ==__fistula__== opens onto the skin ==__anterior to the sphincter complex__==
a bead of meconium CAN pass through this opening → disguises the position of the anus → diagnosis is missed
* When the malformation is high, there is usually a fistula to the urethra in the male or vagina in the female (there may be a fistula to the skin)
!! patients with urethral fistula require prophylactic antibiotics to prevent UTIs
* ==__**First they said separate as above or below the levator ani but then it’s about whether it’s anterior to the sphincter complex???**__==
* UT malformations and lower vertebral anomalies are commonly associated with anorectal abnormalities and should be sought
* In suspected anorectal abnormalities, the perineum is carefully examined for a fistula. If one is not found it is worth waiting 24 hours and then examining the perineum under anaesthesia for one
If one is not found, the anomaly is treated as high and a colostomy is performed as a first stage
* *Treatment depends on the level of the distal pouch. In low lesions, the puborectalis muscle is well formed and a relatively simple operation on the perineum may be sufficient. An anoplasty is performed to increase the calibre of the fistula and the fistula is moved to open within the sphincter complex. Babies who become unwell, or have high lesions , are likely to need a colostomy in the first instance. This rescue procedure allows the baby to feed and empty the bowel. This is followed by complex surgical reconstruction later, involving mobilising the bowel end and reconstructing a sphincter mechanism around it. Long-term faecal continence and bowel and bladder control is imperfect after surgery in many children with high or low anomalies, and careful follow up is needed.*
7
New cards
Oesophageal abnormalities
* associated with polyhydramnios in 30%
* Oesophageal atresia with a distal tracheosphageal fistual accounts for 90% of potentially lethal oesophageal abnormalities (pure oesophageal atresia account for 5% and other variations (recall theme 9) account for the last 5%)
* May have other abnormalities as part of a spectrum of disorders → VACTERL association (V—vertebral, A—anorectal, C—cardiac, T—tracheal, E—‘esophageal’ atresia, R—renal and L—limb abnormalities)
* May be suspected before birth if there is an absent gastric bubble on US together with polyhydramnios but it’s unreliable
* Recall the signs of excess saliva and bubbling snot
Exclude this diagnosis before further feeding to avoid choking or aspiration pneumonia
* Diagnosis → passing a nasogastric tube through the mouth until is stops + simultaneous x ray
* If the oesophagus is ==__obstructed but there is gas in the stomach__== there must be a fistula between the distal oesophagus and trachea
* Operation is performed soon after diagnosis (always resuscitate first though)
dysphagia commonly occurs after surgery even if successful because the peristaltic wave is uncoordinated
* *In pure atresia without a fistula, there is often a long gap between the ends of the oesophagus. Reconstruction may then involve a sequence of planned operations to bridge the gap*
* Oesophageal atresia with a distal tracheosphageal fistual accounts for 90% of potentially lethal oesophageal abnormalities (pure oesophageal atresia account for 5% and other variations (recall theme 9) account for the last 5%)
* May have other abnormalities as part of a spectrum of disorders → VACTERL association (V—vertebral, A—anorectal, C—cardiac, T—tracheal, E—‘esophageal’ atresia, R—renal and L—limb abnormalities)
* May be suspected before birth if there is an absent gastric bubble on US together with polyhydramnios but it’s unreliable
* Recall the signs of excess saliva and bubbling snot
Exclude this diagnosis before further feeding to avoid choking or aspiration pneumonia
* Diagnosis → passing a nasogastric tube through the mouth until is stops + simultaneous x ray
* If the oesophagus is ==__obstructed but there is gas in the stomach__== there must be a fistula between the distal oesophagus and trachea
* Operation is performed soon after diagnosis (always resuscitate first though)
dysphagia commonly occurs after surgery even if successful because the peristaltic wave is uncoordinated
* *In pure atresia without a fistula, there is often a long gap between the ends of the oesophagus. Reconstruction may then involve a sequence of planned operations to bridge the gap*
8
New cards
Failure of passage of meconium
1. Meconium ileus:
* the distal ileus is obstructed by abnormal thick, viscid meconium and mucous plugs
* 95% have CF so all babies with meconium ileus must be tested for it
* Diagnosis is suspected when rectal examination reveals a patent but very narrow rectum
* Gastrografin can confirm diagnosis and if is also often therapeutic as it can chemically loosen the viscid meconium and allow it to pass
* Laparotomy is required for unrelieved obstruction or with signs of peritonitis
2. Hirschsprung disease:
* absent ganglion cells in the inter myenteric and submucosal plexuses and the parasympathetic and sympathetic nerves are scattered in a disorderly way throughout the layers of the bowel wall
* Always involves the rectum, 80% reach the sigmoid and 5% reach the small bowel
* No skip lesions
* Deficient peristalsis → functional obstruction
* 80% of these babies do not pass meconium in the first 24 hrs
* rectal examination may cause explosive release of air and meconium
* Recital biopsy is definitive
* A severe form of enterocolitis may occur in infnantd where the diagnosis is delayed and death may result from circulatory collapse
* Definitive surgery can be done at any time but they typically wait until they’re 10 kg (initially a colostomy can be done for the baby to feed and grow but nowadays conservative management is done at first by frequent recital washouts at home) → removes the entire length of aganglionic bowel and joining normal bowel to the rectum
9
New cards
Congenital diaphragmatic hernia\*\*\*???
* failure of the pleuroperitoneal canal close results in the most common type of diaphragmatic hernia which is postero-lateral
80% are on the left side
* Abdominal viscera lie in the chest, displacing the mediastinum
* Lung development is abnormal (why???) with fewer branching events during development → variable pulmonary hypoplasia (may be so severe that it’s incompatible with life)
* Diagnosis is frequently made at antenatal screening
* Soon after birth, the infant develops reap distress, survival depends on adequate residual lung volume and function
* Cyanosis, mediastinal shift and an empty abdomen are classic sings and diagnosis is confirmed on chest x day following passage of an orogastric tube
* Cardiac malformations are commonly associated
* Initial treatment is orogastric decompression to prevent air entering bowel in the chest to minimise pulmonary compression + gentle assisted ventilation
* Pulmonary hypertension and R to L shunt can occur and vigilance is required to prevent early deterioration
* ECMO can maintain systemic oxygen saturation in pulmonary hypertension
* Urgent surgery is usually delayed until the baby is stable and requiring minimal ventilation → close the defect
* Midgut malrotation is present in 25%
* Mortality is 50% for those diagnosed antenatally and for those who come to operation is 90% so overall mortality is 60-70%
80% are on the left side
* Abdominal viscera lie in the chest, displacing the mediastinum
* Lung development is abnormal (why???) with fewer branching events during development → variable pulmonary hypoplasia (may be so severe that it’s incompatible with life)
* Diagnosis is frequently made at antenatal screening
* Soon after birth, the infant develops reap distress, survival depends on adequate residual lung volume and function
* Cyanosis, mediastinal shift and an empty abdomen are classic sings and diagnosis is confirmed on chest x day following passage of an orogastric tube
* Cardiac malformations are commonly associated
* Initial treatment is orogastric decompression to prevent air entering bowel in the chest to minimise pulmonary compression + gentle assisted ventilation
* Pulmonary hypertension and R to L shunt can occur and vigilance is required to prevent early deterioration
* ECMO can maintain systemic oxygen saturation in pulmonary hypertension
* Urgent surgery is usually delayed until the baby is stable and requiring minimal ventilation → close the defect
* Midgut malrotation is present in 25%
* Mortality is 50% for those diagnosed antenatally and for those who come to operation is 90% so overall mortality is 60-70%
10
New cards
Other surgical conditions causing resp problems in the newborn
1. Vascular ring:
* caused by a persistent double aortic arch or by abnormal configurations of vessels arising from the aortic arch → encircle the trachea and oesophagus → compression
* Symptoms → noisy breathing and sometimes acute apnoeic events with cyanosis
sometimes there are persistent real symptoms with frank stridor
oesophageal symptoms include vomiting, choking or dysphagia
* Surgery is required if severe symptoms, mild symptoms may improve spontaneously
2. Congenital pulmonary airway malformations
3. Congenital lobar emphysema:
* usually affects an upper lobe
* Weakness in a lobar bronchus → air enters the lobe
but bronchial collapse during expiration prevents deflation
* Progressive lobar expansion compresses normal lung and leads to deteriorating real function
* Surgically excise the emphysematous lobe
11
New cards
Abdominal wall defects
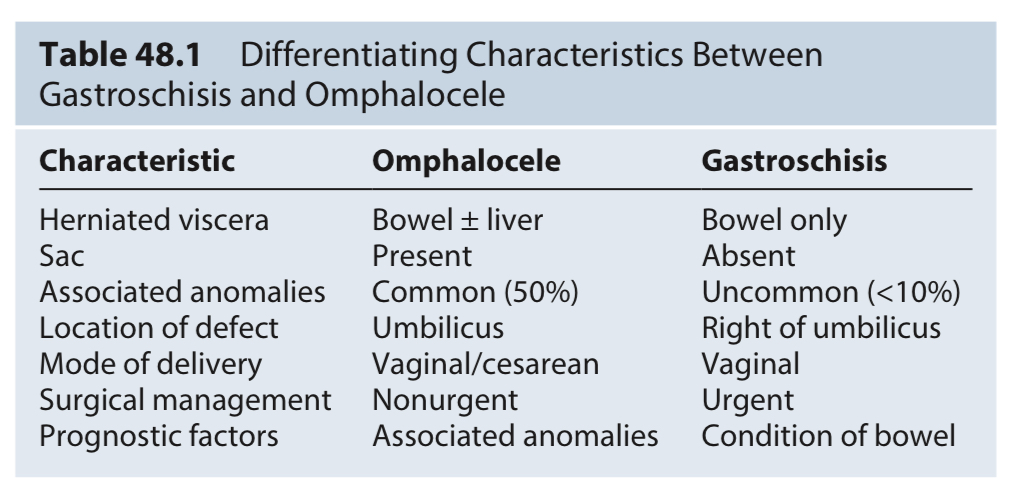
1. Exomphalos/omphalocoele:
* viscera are invested with a layer of fused amnionitic membrane and peritoneum
* Hernia into the base of the umbilical cord due to incomplete folding of the embryonic disc and failure of the umbilical ring to form normally
* Inflammation is thought to be due to chemical irritation from meconium and urine in the amniotic fluid (in this or ruptures/gastroschisis??? Because isn’t it covered)
* Increased AFP but not as often as gastroschisis, diagnosis also made at 20 week US scan
* Isolated omphalocele survival rate is >90% but much less when associated with other defects
* Major = > 5 cm, minor = less
* May also have congenital cardiac problems, neural tube defects (usually spina bifida or anencephaly), chromosomal abnormalities or beckwith-wiedemann syndrome (gigantism, exompjalos, macroglossia, risk of neonatal hypoglycaemia and predisposition to intra abdominal tumours especially Wilms tumours)
* Reactive high risk of coexisting and significant abnormalities (35%)
* Malrotation occurs in 12-20% but rarely with volvulus (although more than gastroschisis), probably due to adhesions between loops and secondary fixation to the abdominal wall
* The sac is initially shiny and translucent but it lacks blood supply and begins to dry out and deteriorate after birth
Within 12 hrs it becomes opaque and yellowish then black, in elastic and desiccated
* The diagnosis at birth is obvious; the only difficulty may be in distinguishing a ruptured exompha los from a gastroschisis. ==__In the latter, there are no sac remnants and the defect is small and separate from the umbilical cord__==
* Exomphalos major:
* part of the abdominal wall is missing
* \
> 5cm with gut, liver and/or spleen
* May be up to 20 cm in diameter and can affect most of the abdominal wall
* At birth the bowel is covered with a sac of amnion and peritoneum, this can rupture spontaneously in utero and present as gastroschisis but this is rare in western countries
* Rupture allows evisceration of the bowel → predisposes to infection and sepsis
* Exomphalos minor:
* represents herniation of the umbilical cord
* < 5 cm with only gut
* Bowel can be easily reduced and the abdominal wall is repaired as a primary procedure
* Associated with more chromosomal abnormalities than ^
* Chest x ray and echocardiogram are required to identify any cardiac lesion and intercurrent pulmonary conditions
2. Gastroschisis:
* coils of bare gut are exposed
* Characterised by bowel herniation through a slit like defect right of the umbilicus
* May be due to rupture of a physiological hernia in the cord between 6 and 10 weeks gestation
* Most diagnosed at the 20 week scan
Often US is performed due to high levels of maternal serum alpha fetoprotein
* Few associated congenital problems although babies may be small and are often premature
* Usually about 3 cm long (so the defect is typically small) and the bowel has no covering membrane
* May involve most of the small and large bowel which becomes densely matted (==__characteristic__==, due to inflammation) and adherent with amniotic (chemical) peritonitis and fibrin from vomiting, defecation and micturition ==__in utero, particularly during the last trimester__==
Inflammatory ‘peel’ may be due to elevated cytokines in the amniotic fluid + effects of foetal urine
* A narrow defect may impair intestinal blood supply → small bowel atresias
* Malrotation is usually present
Typically not repaired at the time of closure and it does not have the same incidence of volvulus as other causes of malrotation
* Cryptorchidism is associated with this in 15-30% of cases
* Antenatal exposure to amniotic fluid can cause adhesions (why???) and shortened oedematous bowel loops → intestinal insufficiency
* Differs from a ruptured exomphalos in that there is → a greater risk of hypothermia, it is a smaller abdominal wall defect and no covering sac, there is a lower incidence of serious coexisting malformation but there is a greater incidence of ==__small bowel atresias__== (also location differs)
* The well-known associa- tion of lower maternal age and low socioeconomic status with a higher incidence of gastroschisis has been linked with violence against women during gestation as a potential factor
* IUGR may also be associated
* Both c section and vaginal are safe (for omphalocele as well or no??? Yes for both, vaginal is preferred)
* Associated with abnormal intestinal motility and nutrient absorption both of which gradually improve in most patients → delay enteral feeding
* Long term outcomes are generally excellent
3. Ectopia vesicae (bladder exstrophy):
* rarest of the major defects, more common in boys
* Presents as a defect between the rectus muscles and public bones with failed development of the entire anterior wall and neck of the bladder and urethra
* Bladder mucosa is exposed on the abdominal wall
* \
* penile epispadias in boys
* Pubic bones may be widely separated → posterior hip joint rotation
* Treatment → close it, aim to achieve urinary continence without back pressure on the kidneys
* initially the exposed bladder mucosa is covered with cling film or a silicone dressing to prevent damage to the fragile urothelium
* Followed be referral to the specialist centre for continuing management
* 2 main operations → soft tissue closure (Kelly procedure) or use of posterior osteotomies to facilitate soft tissue closure (how???)
12
New cards
What is highly suggestive of beckwith-wiedemann syndrome
A large baby with exomphalos minor and macroglossia
13
New cards
Treatment of exomphalos
* aim is to reduce viscera and close the abdominal wall due to high risk of heat and water loss from evaporation because of the moist exposed viscera → place them in a humidicrib with the entire torso wrapped in fresh plastic kitchen wrap or aluminium foil (until surgery)
* Must search for associated anomalies
* Make sure the exposed bowel is not twisted at the opening in the abdominal
* Insert a nasogastric tube to decompress the stomach and herniating bowel + do not feed the baby as it minimises the gut volume and facilitates operative reduction of the bowel
* Commence IV infusion of 10% dextrose to prevent hypoglycaemia during transport especially if the baby has beckwith-wiedemann syndrome (organomegaly, exomphalos and hypoglycaemia secondary to dysregulation of insulin like growth factor 2 expression with hyperinsulinaemia)
* Defects that are less than 1.5 cm in diameter are referred to as a hernia of the cord and are repaired shortly after birth if there are no major associated anomalies
* Immediate reduction of the bowel and closure of the defect are the best courses when the defect is less than 5 cm in diameter; the neonate is fit for an operation and closure may be obtained. Many units may even attempt non-operative reduction in the ward if the baby is well, with closure of the defect using the umbilical cord. Excision of the sac (or remnants, if ruptured) and construction of a cylindrical tube (a 'silo') may be used for larger defects. A sheet of silastic or teflon is sewn to the edge of the defect. Alternatively, a post- operative dressing may be attached to the skin around and over the defect, and used to serially reduce the volume of the exomphalos over 7-10 days by imbri- cation, so that the viscera are returned progressively to the abdomen whilst retaining the integrity of the peritoneum. The prosthesis or dressing is then removed and the defect definitively closed
* in exo, part of the abdominal wall is missing and the abdominal cavity never reached its normal capacity so primary closure would cause diaphragmatic splinting and IVC compression
→ so, a silo bag covering the intestines is used and the bowel is progressively reduced by putting ticks into the silo, expanding the intra abdominal volume
→ repair is performed once this is complete
* IV feeding is usually needed until normal bowel activity returns
* Mortality rate for even larger lesions requiring a silo is low except when associated with cardiac malformations
* Very rarely, non operative management may be required when anaesthesia is contraindicated because of poor condition of the neonate or when the defect is extremely large (> 8 cm) and contains herniated liver
They cause scar formation = development of an eschar over the intact amnion sac
* It is best to not remove the sac covering the liver as it may tear the glisson capsule (i think?)
* Delayed staged closure\*\*\*
* Most will require mechanical ventilation for several days
* Feeding may commence when bowel activity resumes
* Antibiotics are administered postoperatively for only 24-48 hrs unless there are concerns for a wound infection
* The larger the defect size, the higher the incidence of GERD
* The respiratory insufficiency associated with giant omphaloceles may be secondary to abnormal thoracic development, with a narrow thorax and small lung area leading to pulmonary hypoplasia
* Must search for associated anomalies
* Make sure the exposed bowel is not twisted at the opening in the abdominal
* Insert a nasogastric tube to decompress the stomach and herniating bowel + do not feed the baby as it minimises the gut volume and facilitates operative reduction of the bowel
* Commence IV infusion of 10% dextrose to prevent hypoglycaemia during transport especially if the baby has beckwith-wiedemann syndrome (organomegaly, exomphalos and hypoglycaemia secondary to dysregulation of insulin like growth factor 2 expression with hyperinsulinaemia)
* Defects that are less than 1.5 cm in diameter are referred to as a hernia of the cord and are repaired shortly after birth if there are no major associated anomalies
* Immediate reduction of the bowel and closure of the defect are the best courses when the defect is less than 5 cm in diameter; the neonate is fit for an operation and closure may be obtained. Many units may even attempt non-operative reduction in the ward if the baby is well, with closure of the defect using the umbilical cord. Excision of the sac (or remnants, if ruptured) and construction of a cylindrical tube (a 'silo') may be used for larger defects. A sheet of silastic or teflon is sewn to the edge of the defect. Alternatively, a post- operative dressing may be attached to the skin around and over the defect, and used to serially reduce the volume of the exomphalos over 7-10 days by imbri- cation, so that the viscera are returned progressively to the abdomen whilst retaining the integrity of the peritoneum. The prosthesis or dressing is then removed and the defect definitively closed
* in exo, part of the abdominal wall is missing and the abdominal cavity never reached its normal capacity so primary closure would cause diaphragmatic splinting and IVC compression
→ so, a silo bag covering the intestines is used and the bowel is progressively reduced by putting ticks into the silo, expanding the intra abdominal volume
→ repair is performed once this is complete
* IV feeding is usually needed until normal bowel activity returns
* Mortality rate for even larger lesions requiring a silo is low except when associated with cardiac malformations
* Very rarely, non operative management may be required when anaesthesia is contraindicated because of poor condition of the neonate or when the defect is extremely large (> 8 cm) and contains herniated liver
They cause scar formation = development of an eschar over the intact amnion sac
* It is best to not remove the sac covering the liver as it may tear the glisson capsule (i think?)
* Delayed staged closure\*\*\*
* Most will require mechanical ventilation for several days
* Feeding may commence when bowel activity resumes
* Antibiotics are administered postoperatively for only 24-48 hrs unless there are concerns for a wound infection
* The larger the defect size, the higher the incidence of GERD
* The respiratory insufficiency associated with giant omphaloceles may be secondary to abnormal thoracic development, with a narrow thorax and small lung area leading to pulmonary hypoplasia
14
New cards
Ruptured omphalocele\*\*\*
In cases in which the amnionic sac ruptures in utero, the prenatal imaging may be difficult to distinguish from gas- troschisis (Fig. 48.16).167 A large ruptured omphalocele is one of the most challenging pediatric surgical conditions to manage. At birth, there is the urgent need to cover the exposed viscera like a gastroschisis. However, the abdomi- nal wall configuration and the defect itself are usually not amenable for placing a spring-loaded silo. In addition, as opposed to gastroschisis, there is a much more substan- tial loss of intra-abdominal domain that makes gradual reduction of the viscera very difficult. The goal is to cover the exposed abdominal viscera, which can be challenging. One small series had good outcomes in terms of survival, but there was a high incidence of intestinal fistulas, sepsis, and pulmonary hypoplasia.168 In most cases, a silo will have to be fashioned by suturing to the abdominal wall and skin together. Despite the creation of a silo, the reduction is usually still not possible, and some surgeons have advo- cated the use of biologic mesh to create a bed for skin to grow over and be grafted. At that point, the delayed closure of the ventral hernia may be contemplated. Respiratory issues such as pulmonary hypoplasia may complicate the management.
15
New cards
Treatment of gastroschosis
* Aim is to → reduce the eviscerated organs, close the defect, give nutritional support and prevent/treat complications early
* Gastroschisis → primary abdominal wall closure is often possible
* Establish first aid measures (as with omphaloceles) and check viability and evidence of atresia
* Place the infant on the right side to avoid kinking of the mesentery with resultant bowel ischaemia
* Wrap them up in plastic since loss of water and heat risk is great
* If the neonate and bowel are in good condition and the abdominal cavity is of sufficient volume, primary reduction is the preferred method of treatment (can be done in the cot or operating theatre, with or without general anaesthesia)
* If primary closure is not possible → silo → treat the same as omphalos
* Flap repair may be better than fascia closure (eg. The same as with hernias → use of mesh etc)
* Intraabdominal pressure is measured to guide the surgeon during reduction
* Risk of abdominal compartment syndrome → monitor intraabdominal pressure
* Active manoeuvres that may help reduce the volume of the bowel → nasogastric suction (==__important__==), anorectal washouts, enlargement of the defect and intraperitoneal ‘milking’ of the bowel to evacuate as much meconium as possible through the anus, bladder decompression with urethral catheter
* Delay enteral feeding, during this period, nasogastric decompression and parenteral nutrition are required
When bowel activity begins, enteral feeds can be started and slowly advanced
* Gastroschisis → primary abdominal wall closure is often possible
* Establish first aid measures (as with omphaloceles) and check viability and evidence of atresia
* Place the infant on the right side to avoid kinking of the mesentery with resultant bowel ischaemia
* Wrap them up in plastic since loss of water and heat risk is great
* If the neonate and bowel are in good condition and the abdominal cavity is of sufficient volume, primary reduction is the preferred method of treatment (can be done in the cot or operating theatre, with or without general anaesthesia)
* If primary closure is not possible → silo → treat the same as omphalos
* Flap repair may be better than fascia closure (eg. The same as with hernias → use of mesh etc)
* Intraabdominal pressure is measured to guide the surgeon during reduction
* Risk of abdominal compartment syndrome → monitor intraabdominal pressure
* Active manoeuvres that may help reduce the volume of the bowel → nasogastric suction (==__important__==), anorectal washouts, enlargement of the defect and intraperitoneal ‘milking’ of the bowel to evacuate as much meconium as possible through the anus, bladder decompression with urethral catheter
* Delay enteral feeding, during this period, nasogastric decompression and parenteral nutrition are required
When bowel activity begins, enteral feeds can be started and slowly advanced
16
New cards
How long does silo reduction take
1-14 days, most are 5-6 days
17
New cards
What is closing gastroschisis
When the defect size decreases prior to delivery but as the hole gets smaller, the blood supply to the viscera progressively decreases and can result in an atresia
Worst case, the intestines outside the abdominal cavity completely disappear (where the fuck did they go) and results in congenital short bowel syndrome
Worst case, the intestines outside the abdominal cavity completely disappear (where the fuck did they go) and results in congenital short bowel syndrome
18
New cards
What is a complication of reduction
Abdominal compartment syndrome, usually due to overzealous attempts to return the viscera into an abdominal cavity that is too small
19
New cards
Necrotising enterocolitis
* Most common condition needing intra abdominal surgery in newborn babies
* 20-40% mortality
* May run a relatively benign course or be rapidly fatal
* Babies affected are almost always premature, SGA or seriously ill
* Pathophysiology is poorly understood but it involves reduced blood flow to the intestines → relative ischaemia → bowel is invaded by gas producing bacteria → transmural inflammation, necrosis and perforation (+ peritonitis)
* Can affect the SI or LI and may be part of a generalised illness with multi system failure
* Diagnosis can be made clinically if baby has bilious vomiting, dysentery and abdominal distension
confirmed on x day by finding intramural gas = pneumatosis intestinalis
* Stayed using bells staging
suspected NEC = stage 1
definite NEC = stage 2
those requiring surgery = stage 3
* Treatment → resuscitation with IV fluids, nasogastric decompression and broad spectrum antibiotics
* laparotomy and probable surgical resection is done if ^ fails or if bowel perforates and free intraperitoneal gas is seen in x ray
* 20-40% mortality
* May run a relatively benign course or be rapidly fatal
* Babies affected are almost always premature, SGA or seriously ill
* Pathophysiology is poorly understood but it involves reduced blood flow to the intestines → relative ischaemia → bowel is invaded by gas producing bacteria → transmural inflammation, necrosis and perforation (+ peritonitis)
* Can affect the SI or LI and may be part of a generalised illness with multi system failure
* Diagnosis can be made clinically if baby has bilious vomiting, dysentery and abdominal distension
confirmed on x day by finding intramural gas = pneumatosis intestinalis
* Stayed using bells staging
suspected NEC = stage 1
definite NEC = stage 2
those requiring surgery = stage 3
* Treatment → resuscitation with IV fluids, nasogastric decompression and broad spectrum antibiotics
* laparotomy and probable surgical resection is done if ^ fails or if bowel perforates and free intraperitoneal gas is seen in x ray
20
New cards
Abdominal emergencies in infants and young children
1. Incarcerated inguinal hernia:
* incarcerated = hernia has become irreducible
common cause of acute surgical admission in boys (and sometimes girls) below the age of 2 and may occur at any time from birth onwards
high incidence in premature babies (40% of hernias in the neonatal period are discovered because they become irreducible, but the risk declines as they grow up)
* strangulation can follow incarceration but it is uncommon in young children unlike in adults
* There is invariably a congenital patent processus vaginalis (= indirect hernia, wait so there might not be a PPV if direct??? future nour here-- yes there is no PPV in direct)
* When it incarcerates it becomes painful, tender and irreducible
* Child may have vomited but the diagnosis is usually made before intestinal obstruction occurs
* Obstruction of bowel → vomiting → fluid depletion and electrolyte imbalances
\+ strangulation → infarction
* Pressure in the spermatic cord at the ==__external ring__== may cause testicular vascular obstruction (why only external ring???)
* If the child is not systemically unwell and the hernia is not red or tender then it is unlikely that the bowel has become infarcted
* Emergency surgery is best avoided if possible except in the unwell child with signs of intestinal obstruction
* Treatment involves actively reducing (gentle manipulation, succeeds in 80%) the hernia and performing elective herniotomy 48 hrs later when ==__oedema has resolved__==
* It is not impossible to reduce necrotic bowel in a hernia but it is hard
* Failed reduction of an incarcerated hernia is associated a high rate of testicular atrophy (40%)
2. Pyloric stenosis (they say congenital but last theme they said it wasn’t congenital):
* check theme 9
* Despite hypochloraemic alkalosis, there is also usually a paradoxical aciduria due to dehydration causing the kidney to conserve plasma tonicity at the expense of hydrogen ions which causes the aciduria and further adds to the alkalosis
* Diagnosis → test feed = feeding the baby and palpating the abdomen at the same time
* it is important to first decompress the stomach first by nasogastric tube as a dilated stomach often displaces the pylorus to lie under the liver edge
* If it is pyloric stenosis then a firm mass about 2 cm (olive like) is palpable deeply below the liver and disappears after the feed
* Can be detected by US but harder
* If still in doubt → upper GI contrast reveals a narrow pylorus and little contrast in the duodenum
* Treatment:
* natural history without surgery is for the hypertrophy to gradually resolve over several months but most children would die from electrolyte imbalances or malnutrition before this can happen
* So, treatment is surgical after resuscitation
3. Intussusception:
* check theme 9
* Acquired between 6 weeks and 2 years
* 40% have adenovirus infection
* seasonal increase of intussusception in the spring and autumn, virus is also most common at these times of year
* Lead point (intussusceptum) is commonly a thickening of the bowel wall caused by non specific or viral hypertrophy of peyers lymphatic patches
* If untreated the sections may undergo venous infarction
* 10% have an anatomical abnormality termed a pathological lead point
* In older children or adults, the initiating factor may be a bowel wall tumour or polyp
* Redcurrant jelly stool is almost pathognomonic when the other clinical features are present
* Vomiting begins later but there may be profound fluid depletion even without complete obstruction
* A sausage shaped made is often found in the upper right quadrant with a scaphoid (hollowed) appearance in the right iliac fossa
* Rectum is empty but may contain a little bit of blood
* A normal US does not exclude it
* Air enema and plain x ray are quick and reliable but diagnosis is urgent so must be done quick
* Fluid resuscitation is vital even before attempting to diagnose or reduce it
usually given a fluid bolus of suitable crystalloid and an empirical broad spectrum antibiotic before transfer to the radiological department
* Treatment needs to be prompt and active, air enema may be diagnostic and therapeutic (in 90%)
* Resection with primary bowel anastomosis may be necessary if the intestine is ischaemic or it is impossible to reduce without causing major trauma to the bowel
4. Swallow foreign body:
* bunch of bullshit
* Coins are not removed, parents must inspect stool for it and come back if signs of bowel obstruction or abdominal pain develop
21
New cards
Abdominal emergencies in older children
The acute abdomen:
\
* Appendicitis is usually suspected
* Acute non specific abdominal pain is common, closely followed by mesenteric adenitis (are these the most common 2 or?)
* Mesenteric whatever sometimes causes a higher fever than appendicitis, signs and symptoms usually settle within 24 hrs, there is often a recent history of viral upper respiratory infection and enlarged cervical lymph nodes may be palpable
* Less commonly, acute abdominal pain in this age group may be caused by extra abdominal causes
* torsion of the testis may be one (abdominal pain may be the only symptom) so, genitalia must always always be examined in boys with abdominal pain
* Exclude UTI
* Also check ENT, meningitis, basal pneumonia (usually right sided) etc
* Acute appendicitis is importsnt to exclude in this age group (uncommon < 2 y/o)
* check theme 9
* Unlike adults, children often present with peritonitis and children under 5 y/o usually have a perforation or a gangrenous appendix at operation
* Fasting delays diagnosis
* The child may just be admitted to the hospital and checked every 2 hours or so (this makes zero sense, go over it)
\
* testicular torsion can present with iliac fossa pain alone without testicular pain
* just be suspected in any make under 25 with acute testicular pain
* Predisposition is usually bilateral and both testes are at risk
* Check precious flash cards
* May be mimicked by torsion of hydatid of morgagni and epididymitis
* Palpating individual scrotal structures is often impossible because of extreme tenderness and sometimes oedema
* Very localised tenderness at the superior pole of the testis is sometimes found in torsion of a hydatid
* When a diagnosis of torsion cannot be excluded, the only safe option is to carry out urgent surgical exploration
\
* Appendicitis is usually suspected
* Acute non specific abdominal pain is common, closely followed by mesenteric adenitis (are these the most common 2 or?)
* Mesenteric whatever sometimes causes a higher fever than appendicitis, signs and symptoms usually settle within 24 hrs, there is often a recent history of viral upper respiratory infection and enlarged cervical lymph nodes may be palpable
* Less commonly, acute abdominal pain in this age group may be caused by extra abdominal causes
* torsion of the testis may be one (abdominal pain may be the only symptom) so, genitalia must always always be examined in boys with abdominal pain
* Exclude UTI
* Also check ENT, meningitis, basal pneumonia (usually right sided) etc
* Acute appendicitis is importsnt to exclude in this age group (uncommon < 2 y/o)
* check theme 9
* Unlike adults, children often present with peritonitis and children under 5 y/o usually have a perforation or a gangrenous appendix at operation
* Fasting delays diagnosis
* The child may just be admitted to the hospital and checked every 2 hours or so (this makes zero sense, go over it)
\
* testicular torsion can present with iliac fossa pain alone without testicular pain
* just be suspected in any make under 25 with acute testicular pain
* Predisposition is usually bilateral and both testes are at risk
* Check precious flash cards
* May be mimicked by torsion of hydatid of morgagni and epididymitis
* Palpating individual scrotal structures is often impossible because of extreme tenderness and sometimes oedema
* Very localised tenderness at the superior pole of the testis is sometimes found in torsion of a hydatid
* When a diagnosis of torsion cannot be excluded, the only safe option is to carry out urgent surgical exploration
22
New cards
When does the abdominal wall form etc
4th week, when differential growth of the embryo causes unfolding in the craniocaudal and mediolateral directions
\
In the context of gastroschisis, during the 6th week, rapid intestinal and liver growth leads to herniating of the midgut into the umbilical cord
\
Elongation and rotation of the midgut occurs over the ensuing 4 weeks, by week 10, the midgut returns to the abdominal cavity, where the first, second, and third portions of the duode- num and the ascending and descending colon assume their fixed, retroperitoneal positions
\
In the context of gastroschisis, during the 6th week, rapid intestinal and liver growth leads to herniating of the midgut into the umbilical cord
\
Elongation and rotation of the midgut occurs over the ensuing 4 weeks, by week 10, the midgut returns to the abdominal cavity, where the first, second, and third portions of the duode- num and the ascending and descending colon assume their fixed, retroperitoneal positions
23
New cards
Bladder exstrophy (ectopia vesicae)
Failure of fusion of the lower abdominal wall during embryonic development leaves the bladder exposed as a flat plaque on the lower abdomen \[Fig. 8.4\]. There is no covering muscle or skin. The pubic rami do not fuse in the midline and remain widely separated. The ureters protrude from the exposed bladder and dribble urine
The urethra is exposed as a flat strip and the bladder outlet sphincters are not functional. Bladder exstrophy, also known as 'ectopia vesicae', is rare, with an inci- dence of 1:40,000 births. Reconstructive surgery to close the bladder and abdominal wall with restoration of bladder sphincters is one of the greatest challenges of pediatric urology. An even rarer variant of bladder exstrophy is known as cloacal exstrophy. In this condition, the shortened proximal colon is fused on to the bladder exstrophy and there may be an imperforate anus
The urethra is exposed as a flat strip and the bladder outlet sphincters are not functional. Bladder exstrophy, also known as 'ectopia vesicae', is rare, with an inci- dence of 1:40,000 births. Reconstructive surgery to close the bladder and abdominal wall with restoration of bladder sphincters is one of the greatest challenges of pediatric urology. An even rarer variant of bladder exstrophy is known as cloacal exstrophy. In this condition, the shortened proximal colon is fused on to the bladder exstrophy and there may be an imperforate anus