Overview of Descending Pathways: Motor Systems
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
20 Terms
What are the control centers for motor movement?
Motor function is controlled by the frontal lobes
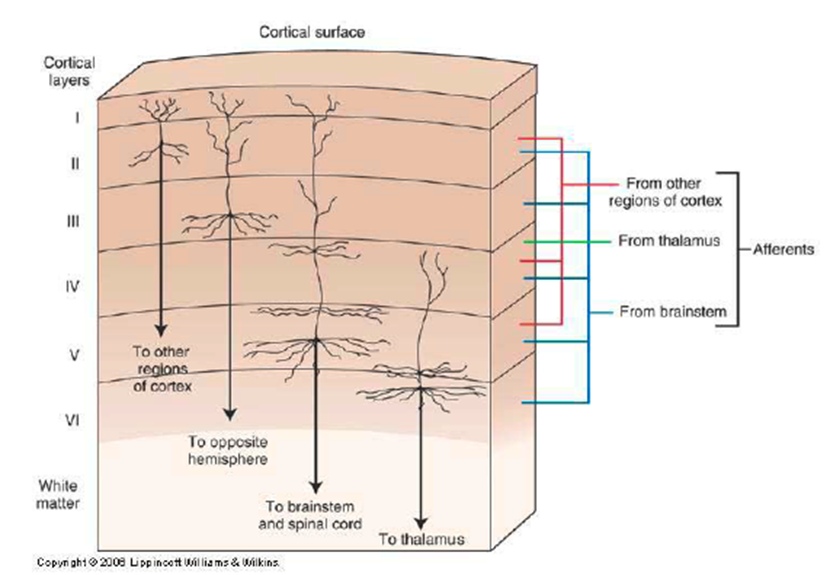
1) Primary Motor Cortex is located precentral gyrus of each frontal lobe. This primary motor cortex is comprised of 6 layers:
→ molecular
→ external granular
→ external pyramidal
→ internal granular
→ internal pyramidal (contains the giant Betz cells which are the largest neurons of the body)
→ multiform
What are giant Betz Cells
Giant Betz Cells are the largest neurons in the body and are localized to Layer V or the internal pyramidal layer of the primary motor cortex
1) these large neurons will project to major descending motor pathways
→ also the UMN that initiate movement
How is the Motor Cortex homunculus organized?
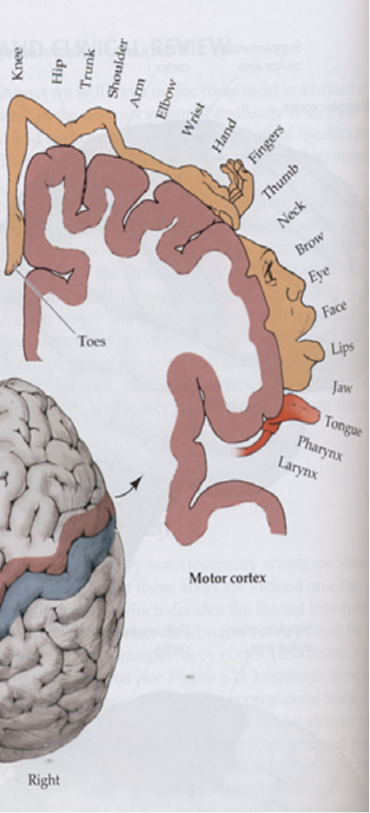
Motor Cortex has somatotopic organization meaning that the brain is mapped out to specific parts of the body
→ Face is localized laterally
→ Legs medially
→ Hands are in between the legs and face
How does the primary motor cortex control motor movement?
the primary motor cortex controls motor movements by influencing the alpha motor neurons in the anterior horn of the spinal cord
1) rather than controlling one individual motor neuron at a time, the primary motor cortex encodes the parameters of a specific movement
→ force
→ timing
→ direction
→ speed
What is the Motor Association Cortex?
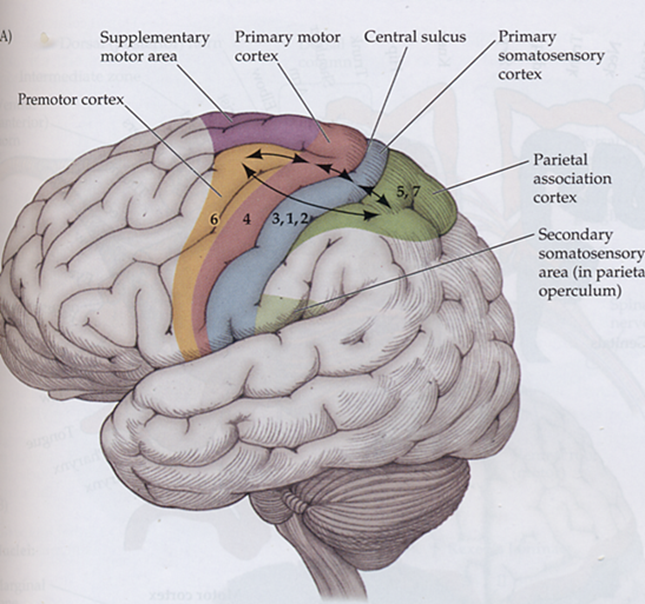
there are cortexes that are anterior to the premotor cortex and coordinates with the premotor cortex for movement
1) supplementary motor cortex
→ used in internally generated movements - internal stimuli
→ planning of bilateral movement such as using hands together
2) premotor cortex
→ selection of motor plans based on external stimulus such as catching a ball
What is the organization of the corticospinal pathway as it enters through the internal capsule?
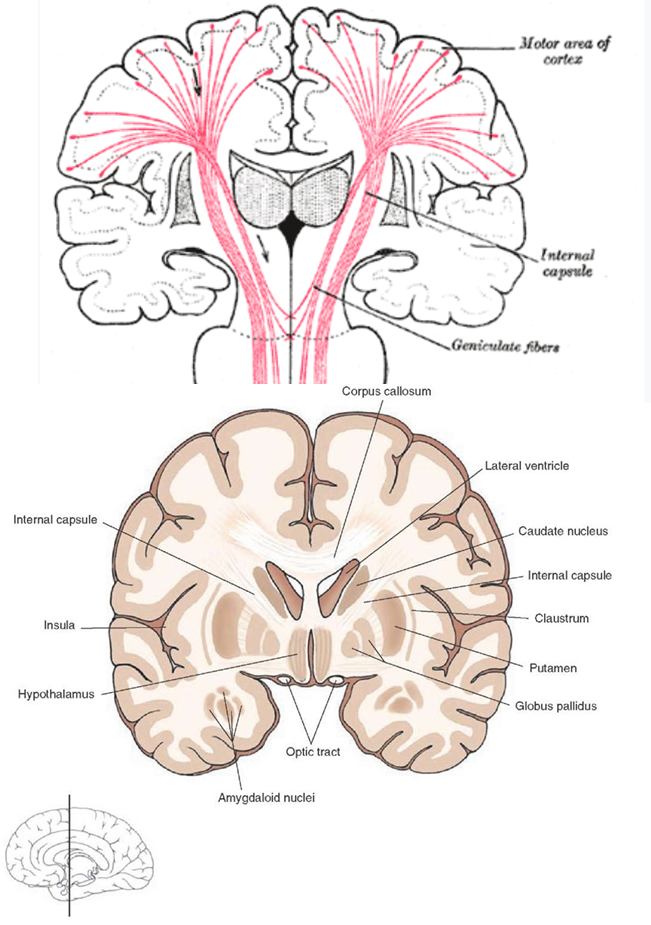
1) Fibers from Layer V or the Intrapyramidal layer pass through white matter bands called the corona radiata and then through the internal capsule
→ internal capsule passes through the basal ganglia
2) Somatotopic organization is maintained as it moves through the internal capsule
→ corticobulbar tract responsible for the face is in the genu of the internal capsule
→ areas for arm, trunk, and leg are in the anterior 2/3 of the posterior limb of the internal capsule
What happens to the corticospinal tract in the medulla?
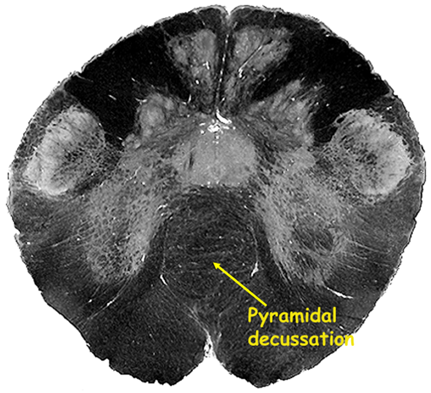
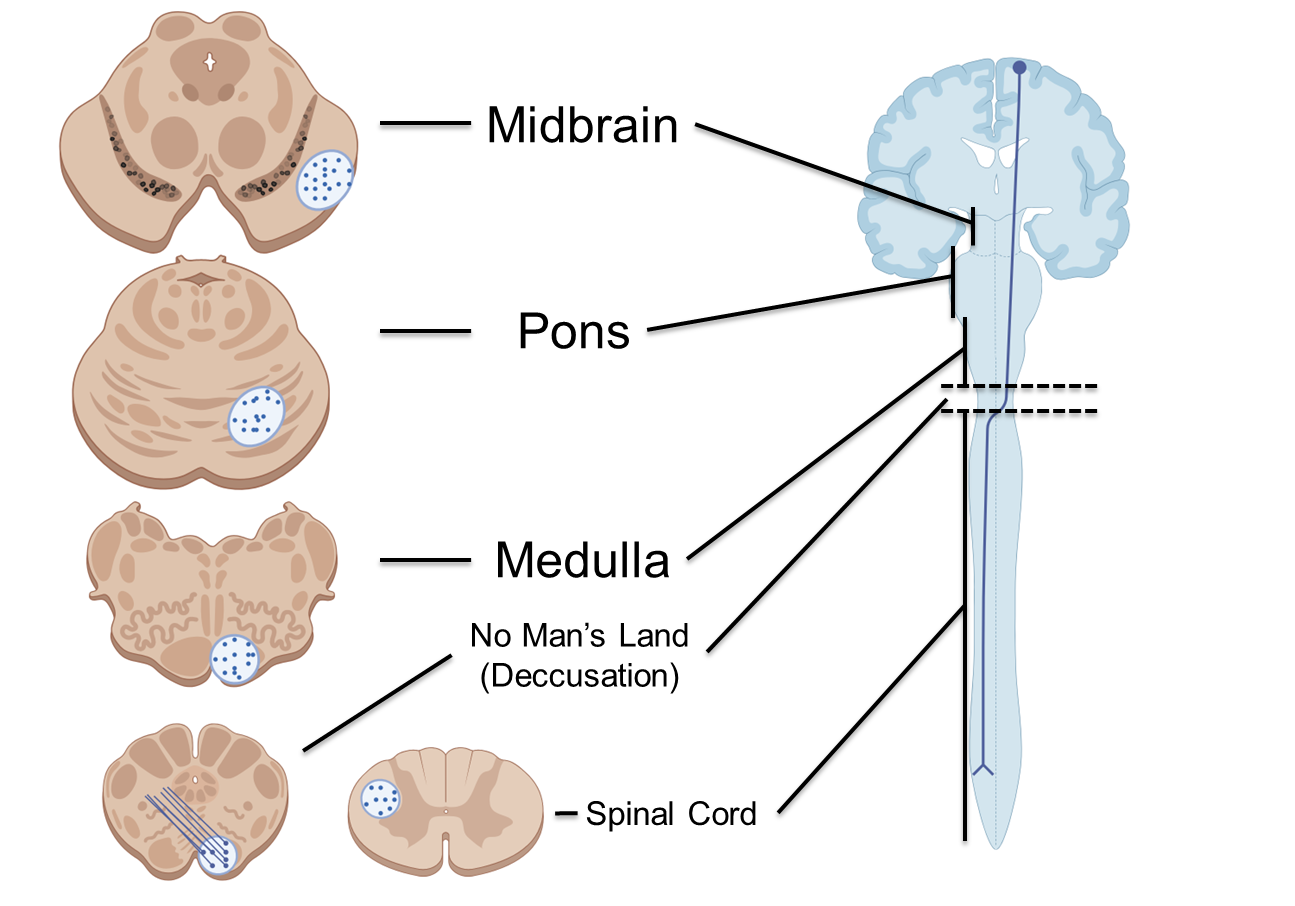
Fibers from the corticospinal tract of the internal capsule will move through the cerebral peduncle of the midbrain and then through the bridging fibers of the pons
→ the pathway then reaches the medullary pyramids where the majority of the fibers will decussate or cross over immediately after the medulla in a process known as pyramidal decussation
→ also known as pyramidal pathways
→ the remaining portion of the fibers will stay ipsilateral (stay on the same side of the body) and form the anterior corticospinal pathway
What happens to the corticospinal tract in the spinal cord?
1) In the spinal cord the lateral fibers or the fibers that have decussated will descend in the lateral column to their level
2) fibers that remained ipsilateral (on the same side) descend through the anterior/ventral column
→ provide bilateral innervation, so if one path is destroyed another pathway for axial musculature is preserved
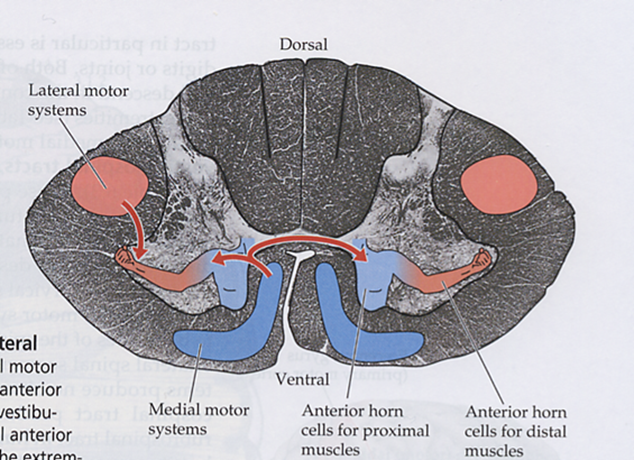
Fibers will then synapse with LMN at the anterior horn (gray matter)
What is the difference between the anterior and lateral corticospinal pathway?
Lateral corticospinal pathway is the major descending motor pathway of the body
→ responsible mostly for limb movement and will cross over at the caudal medulla
Anterior Corticospinal pathway is the portion of the pathway that remains ipsilateral
→ responsible for movement of the axial muscles
where do somatic efferent pathways exit?
Somatic Efferent pathways will exit from the anterior horn of the spinal cord and head and move directly to the target tissue or muscle
What are Autonomic Pathways?
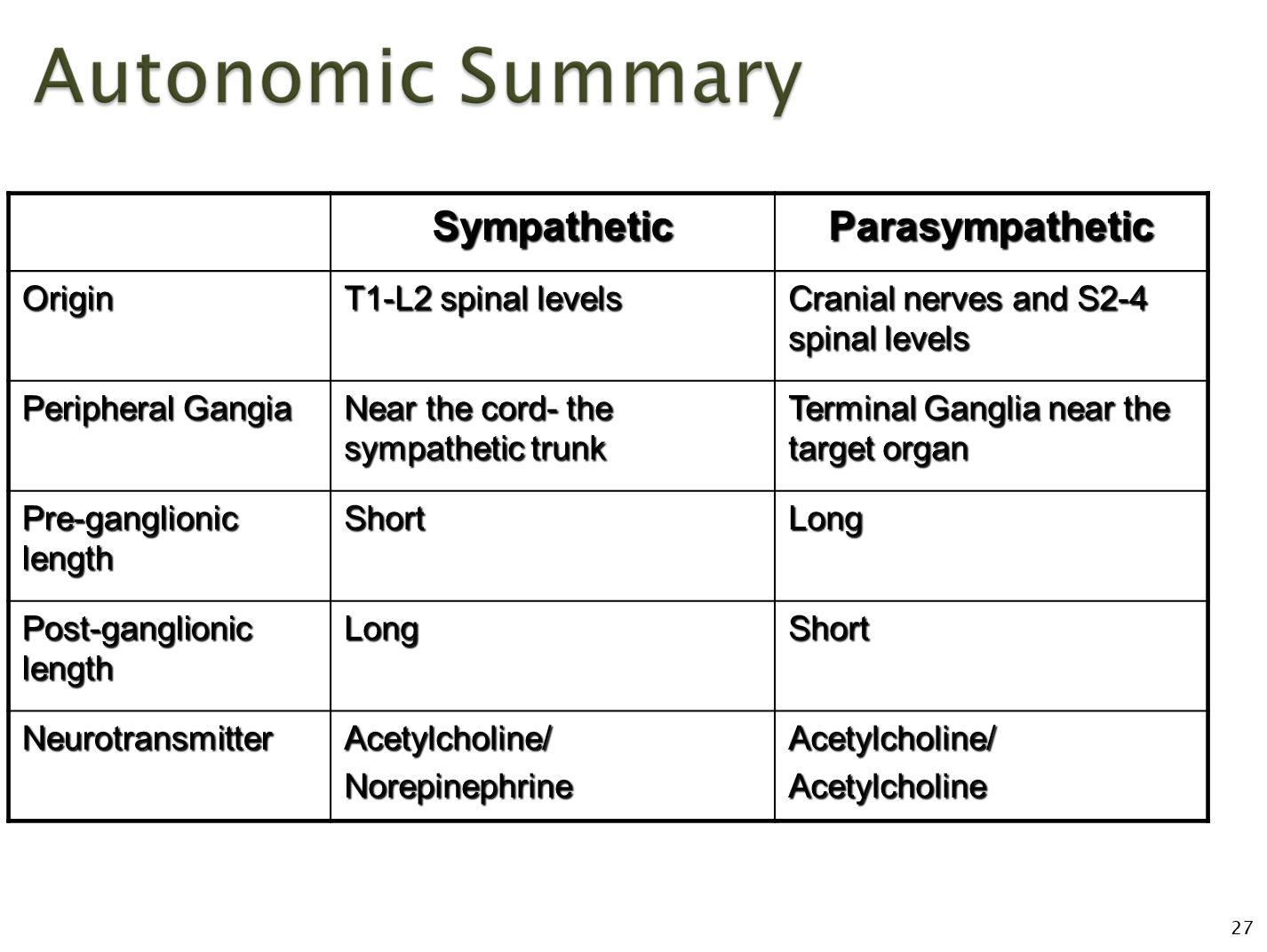
Unlike somatic efferent pathways that directly target to the organ, autonomic pathways must project to the peripheral ganglion and synapse before going to their target
1) Where they exit is dependent on if they are parasympathetic or sympathetic
→ parasympathetics exit from the cranial nerves (III, VII, IX, and X) and in the sacrum. Ganglion are typically farther away
→ sympathetics exit from the thoracic and upper lumbar (T1-L2), with their ganglion being close to the spinal cord
2) Parasympathetics and sympathetics use different transmitters
→ parasympathetic uses acetylcholine for both pre and post
→ sympathetic uses acetylcholine for pre and norepinephrine for post
How do you assess whether something is an upper or lower motor symptom? (6)
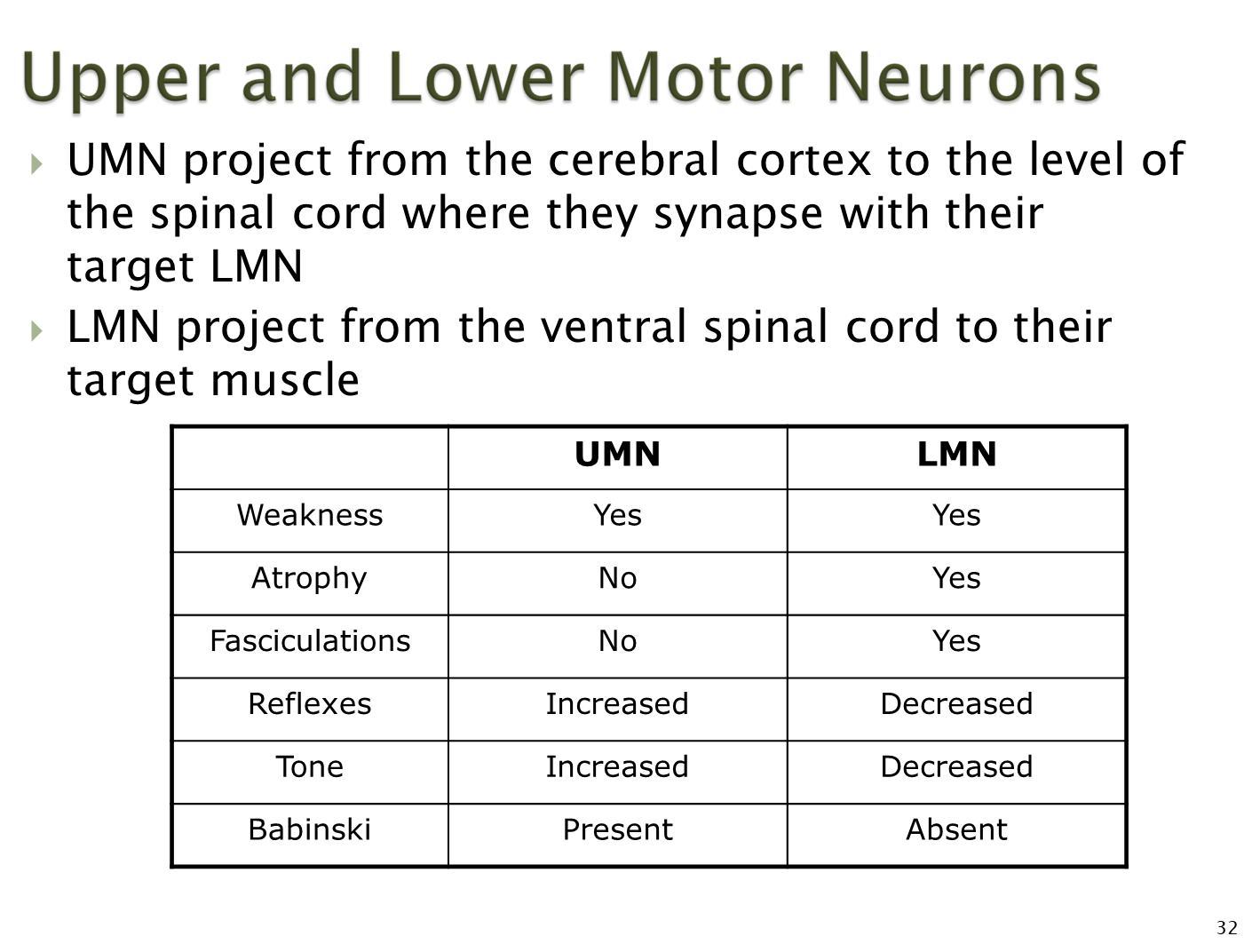
Symptoms for UMN or LMN injury is organized based on:
→ weakness
→ atrophy
→ fasciculations
→ reflexes
→ tone
→ babinski
What is the difference between paresis, plegia, paralysis and palsy?
Paresis - weakness
Plegia - no movement
Paralysis - no movement
Palsy - imprecise term for weakness
What is the difference between hemi, para, mono, di, and quadri?
Hemi - one side of the body
Para - both legs
Mono - one limb
Di - both sides of the body equally affected
Quadri - all limbs
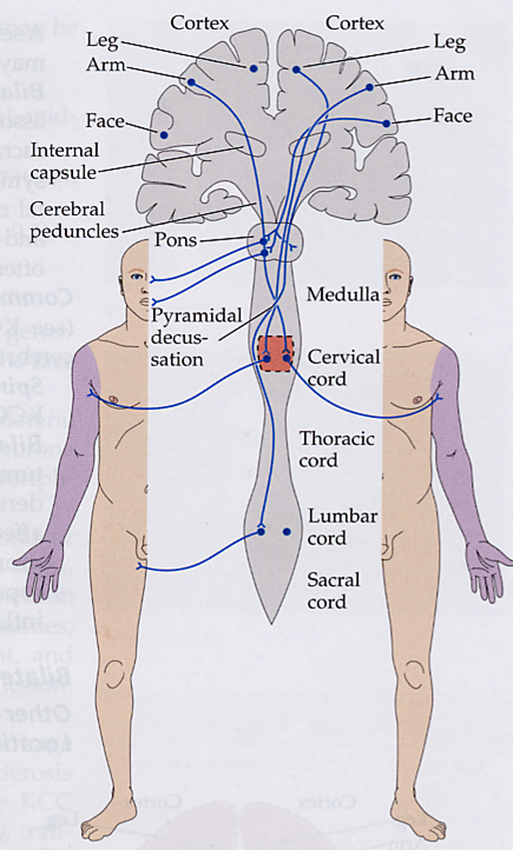
What causes hemiparesis
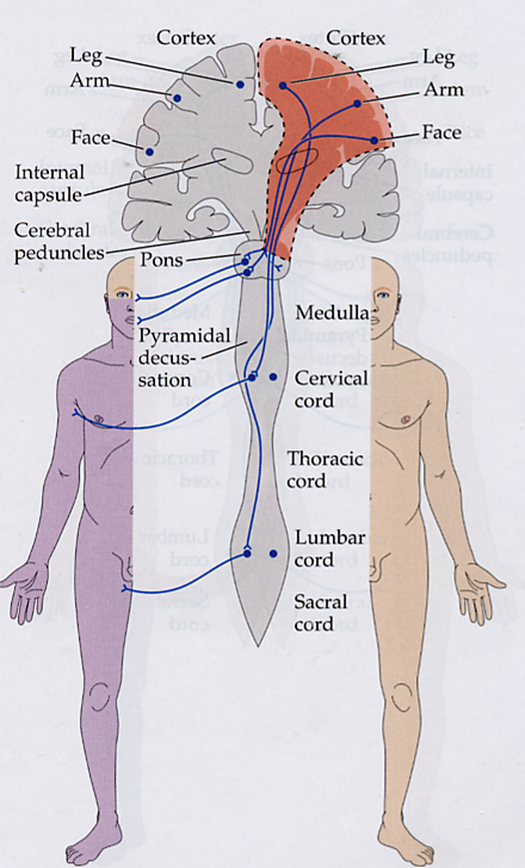
Hemiparesis is one side of the body having weakness
→ because hemiparesis involves the entire half of a body, including the face the lesion is localized from the pons up to the cortex, most commonly in the internal capsule
→ weakness will be contralateral to the lesion
What causes Unilateral Arm Weakness
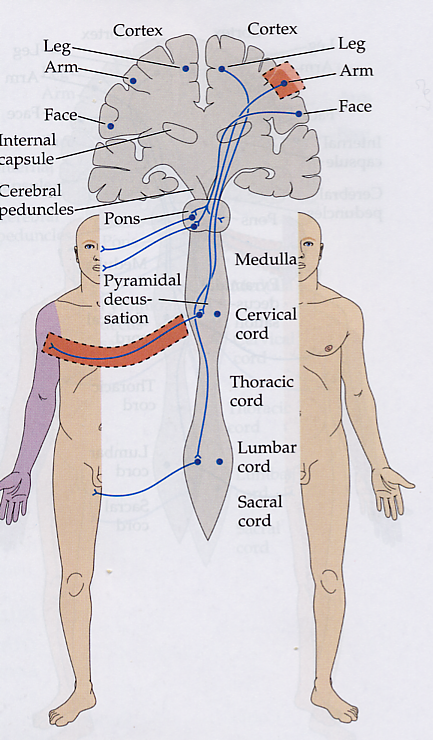
Unilateral Arm Weakness can be either upper or lower in origin often associated with a small portion of the cortex or a peripheral nerve
→ in order to localize it, look for additional symptoms associated with UMN or LMN
What causes Unilateral Leg Weakness
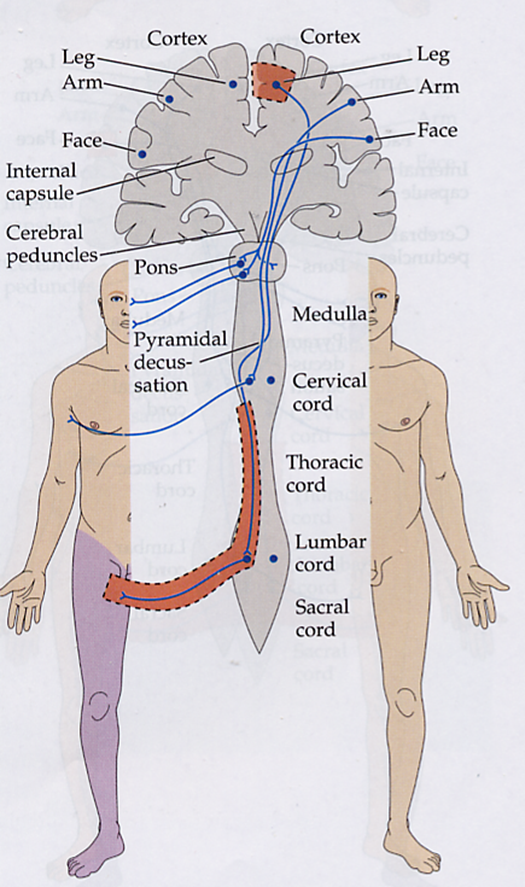
One leg is affected with the lesion being localized to the → motor cortex
→ lower lateral spinal cord
→ peripheral nerve
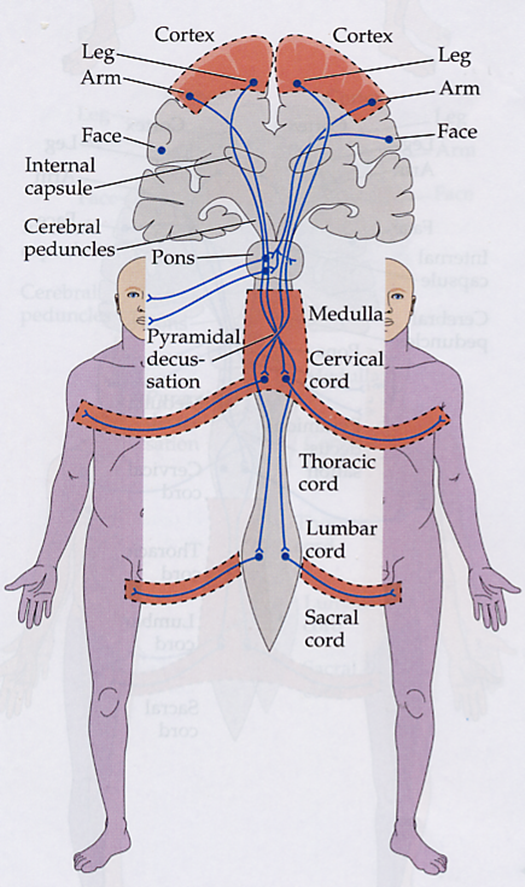
What causes Bilateral Arm Weakness
Bilateral arm weakness, or weakness of both arms is typically caused by central cord syndromes that affect the medial fibers of the corticospinal tract
What causes Bilateral Leg Weakness
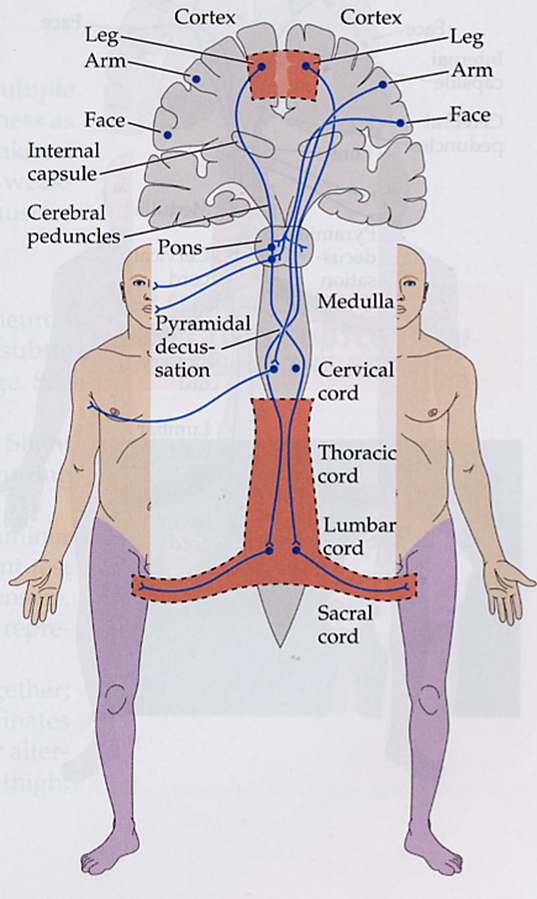
Weakness of both legs can be seen in lesions of the medial cortical lesions or lower cord lesions
→ this can be a cortical lesion unlike the arms because the leg regions are located right next to each other
What causes Quadriparesis
Quadriparesis can be localized anywhere whether that’s some injury to the motor cortex, spinal cord, or peripheral nerves