ventricular system 4/24
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
functions of cerebrospinal fluid (CSF)
buoyancy—support weight of brain in skull
protection—cushion during trauma to skull
stable chemical environment
formation of CSF
average volume=150mL
25 mL in ventricles (remainder in subarachnoid space)
turnover rate=4-5 times/day→~500mL formed/day
CSF circulation
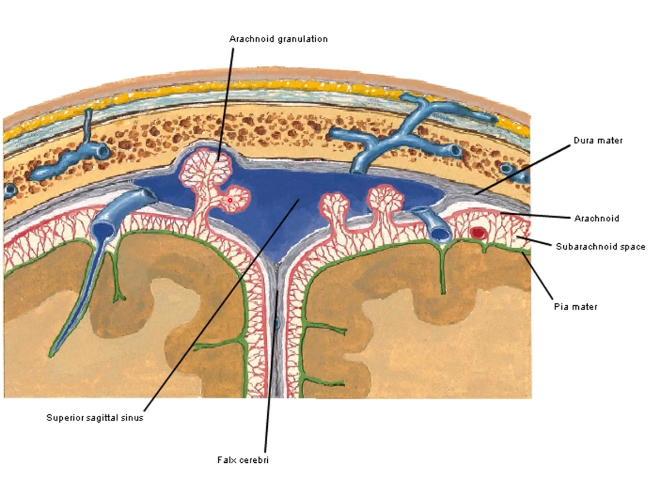
choroid plexus (ventricles)→ventricular circulation→4th ventricular exit foramina→basal cisterns→subarachnoid space over lateral convexities (travel superiorly)→arachnoid villi→absorbed by arachnoid granulations into venous system (superior sagittal sinus)
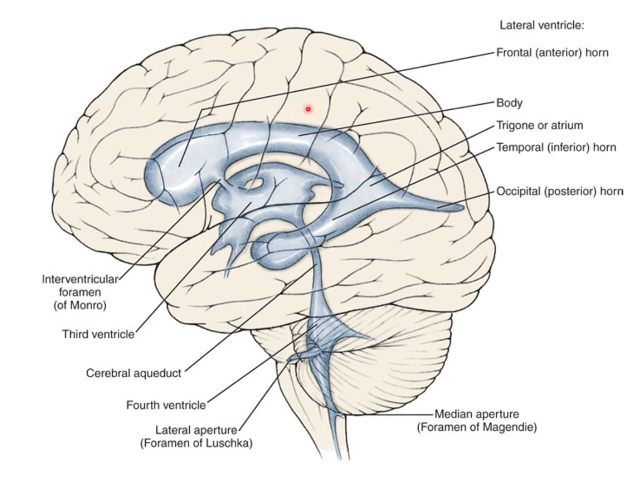
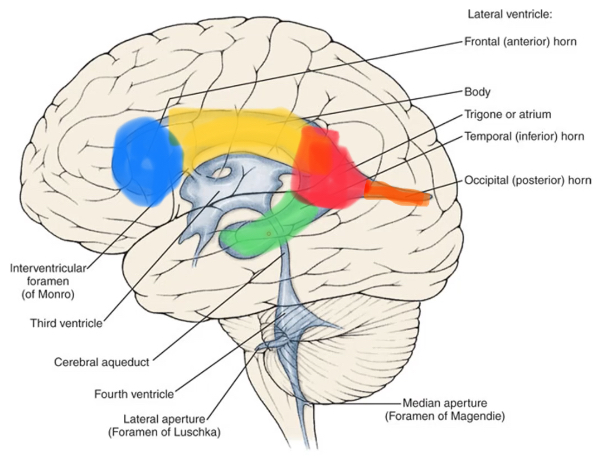
ventricular system
lateral ventricles (1 and 2): interventricular foramen of monroe
3rd ventricle: cerebral aqueduct
4th ventricle: foramen of magendie and luschka
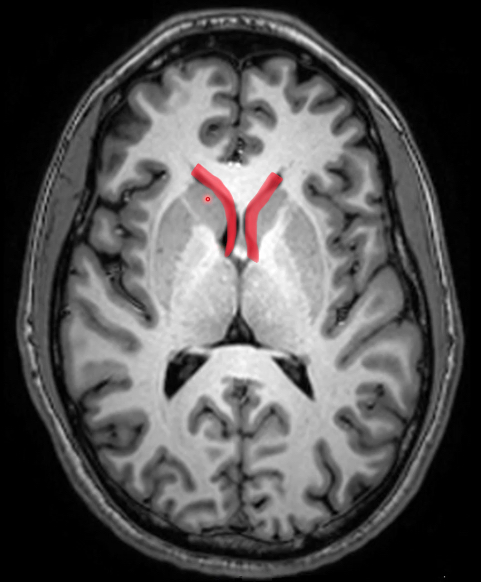
interventricular foramen of monroe
connects each lateral ventricle to 3rd ventricle
contains choroid plexus
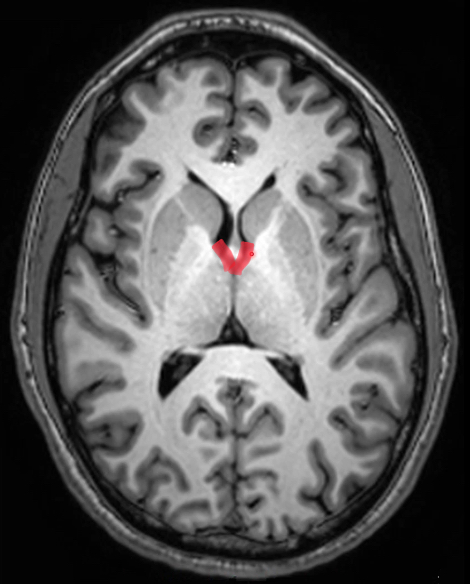
3rd ventricle
midline cavity found in diencephalon
connects with 4th ventricle via cerebral aqueduct
contains choroid plexus
lateral walls: hypothalamus (inf) and thalamus (sup)
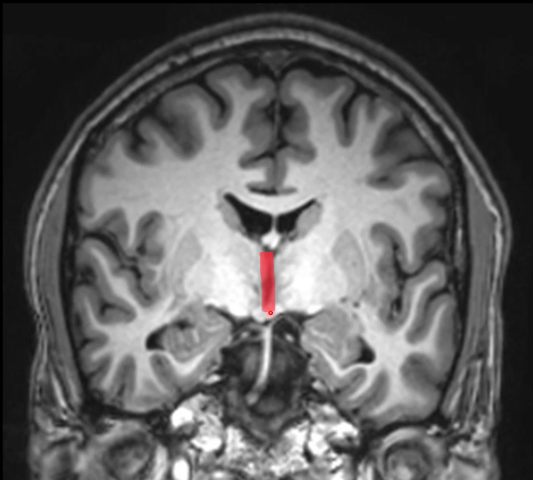
cerebral aqueduct
15-18 mm in length, 1-2 mm in diameter
within posterior midbrain
anterior to cerebellum
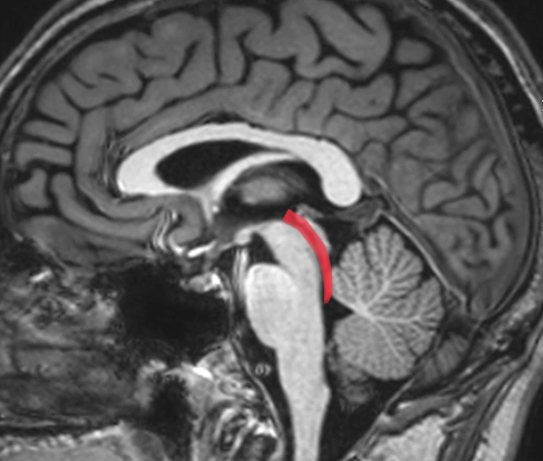
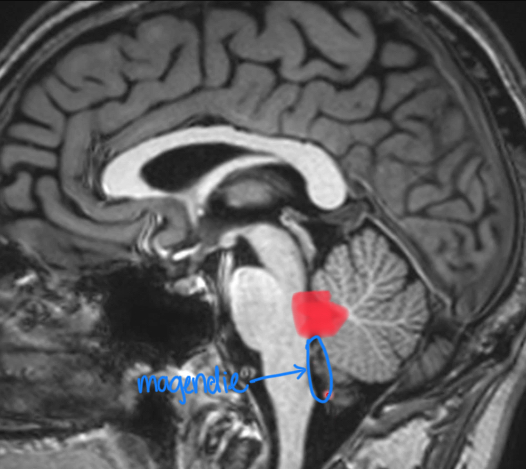
4th ventricle
between brainstem and cerebellum
CSF leaves via 3 exit foramina (1 magendie near midline and 2 luschka on lateral sides)
lateral ventricle anatomy
largest, seen in both hemispheres
frontal/anterior horn: deep within frontal lobe
body: interventricular foramen to trigone/atrium
atrium: triangular region posterior to body
occipital/posterior horn: deep within occipital lobe, protruding from atrium
temporal/inferior horn: inferior part deep within temporal lobe
frontal horn of lateral ventricle
anterior to interventricular foramen
no choroid plexus
lateral wall: caudate nucleus
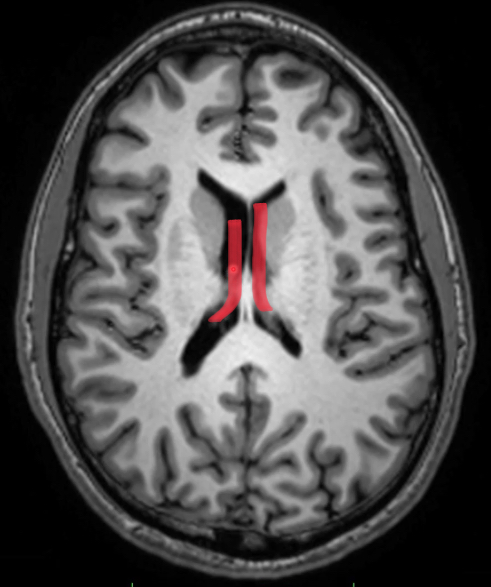
body of lateral ventricle
from interventricular foramen to splenium of corpus callosum
contains choroid plexus (gray stuff in the cavity)
posterior wall: splenium
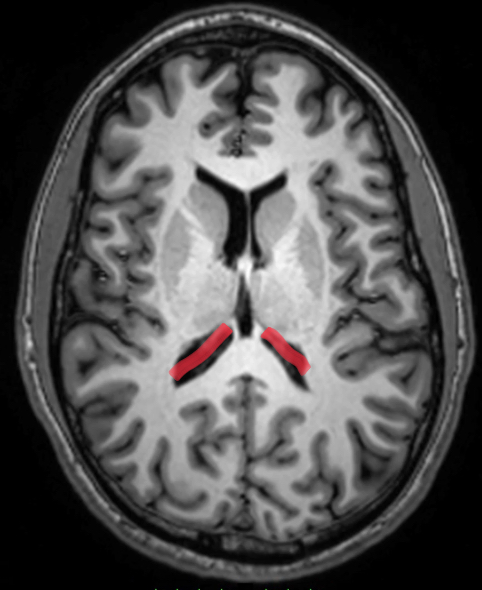
trigone of lateral ventricle
junction between body, occipital, temporal horns
contains choroid plexus (glomus)—large amount
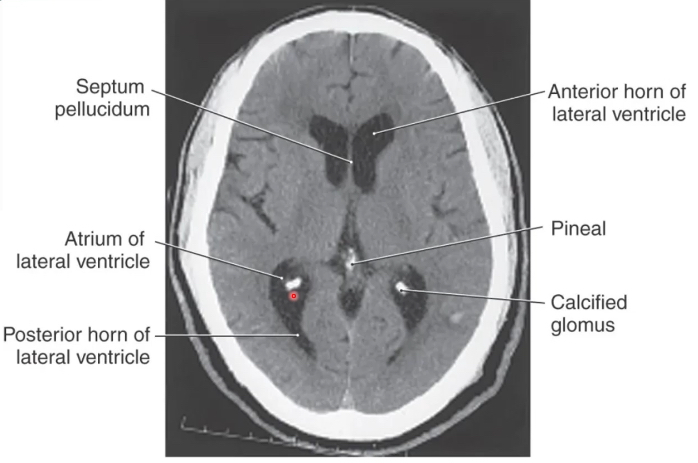
calcified glomus
occurs as we age (along w/ pineal gland)
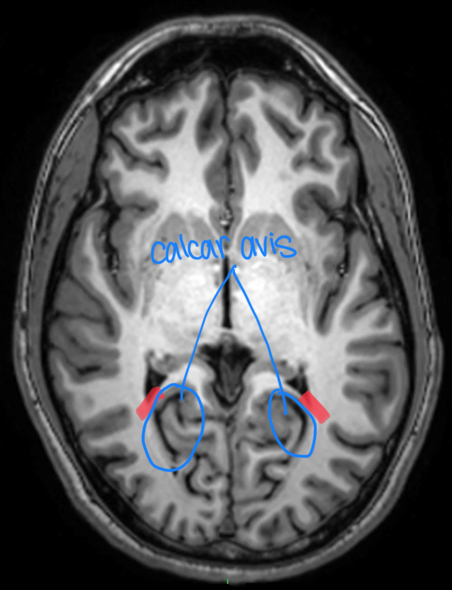
occipital horn of lateral ventricle
most variable part of ventricular system
medially: calcar avis, which bulges into horn
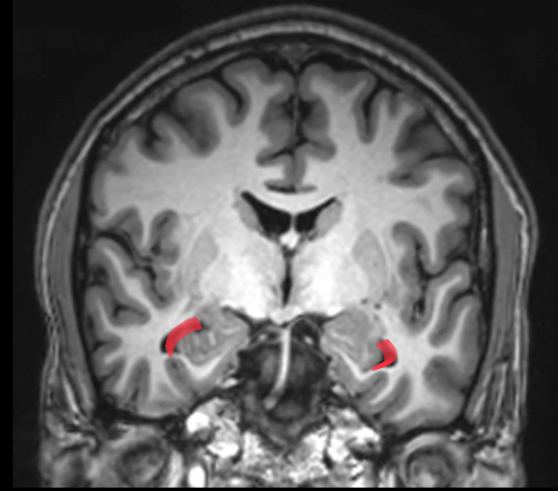
temporal horn of lateral ventricle
3cm to temporal pole (most anterior part of temporal lobe)
contains choroid plexus
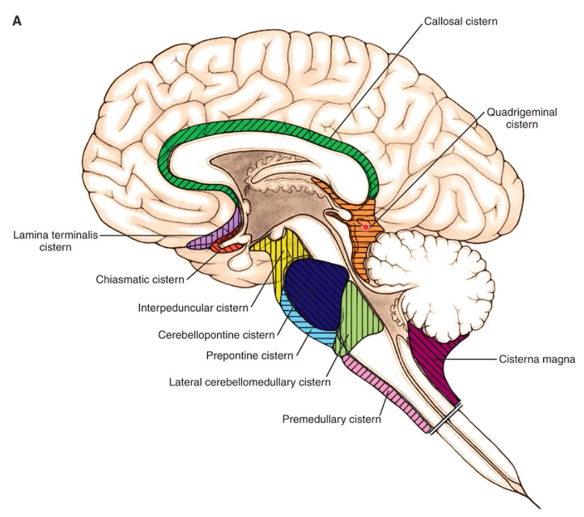
subarachnoid cisterns
areas of subarachnoid space that surround brainstem, cerebellum, medial brain
1st area: basal cistern, cisterna magna (receives CSF that leaves 4th ventricle)
continuous with subarachnoid space of spinal cord and lateral convexities of the brain
moves in a superior direction into superior sagittal sinus from arachnoid villi
lumbar cistern
L1-L5 aka caudal dural sac after SC ends (conus medullaris btwn L1 and L2)
this is where CSF can be drawn for analysis
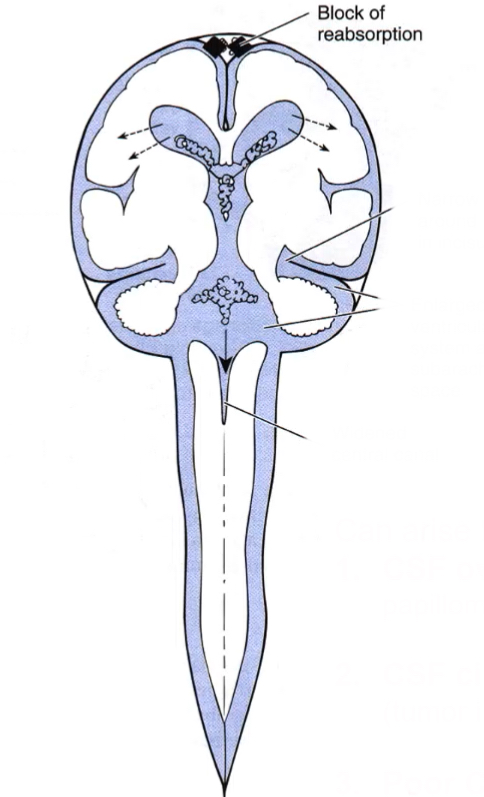
hydrocephalus
enlargement of ventricles due to increase in volume of CSF
caused by CSF flow obstruction/impaired absorption
causes CSF to permeate through ependymal lining into periventricular white matter→raised ICP, white matter damage, gliotic scarring, CSF absorption via periventricular blood vessels
hydrocephalus acute onset in infants and young children
irritability, impaired conscious level and vomiting
gradual onset hydrocephalus in infants and young children
failure to thrive
clinical features of hydrocephalus in infants and young children
bulging or tense anterior fontanelle (soft spot)
cracked pot sound on skull percussion
increased skull circumference (compared to normal growth curves)
lid retraction, impaired upward gaze: due to pressure on midbrain (vertical gaze center!)
thin scalp w/ dilated veins

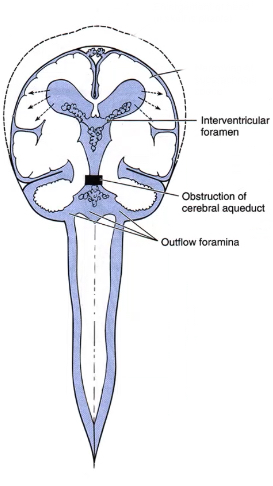
non-communicating hydrocephalus (obstructive)
typically due to congenital aqueductal stenosis/blockage of ventricular system
structures superior to blockage dilate (and skull in infants bc it isn’t fully calcified yet)
enlarged head (if skull is pliable)
narrowing of subarachnoid space
communicating hydrocephalus
can arise from 3 causes: CSF oversecretion (choroid papilloma), CSF circulation blockage (subarachnoid space tumor), poor CSF absorption (meningitis)
blockage of CSF flow outside of ventricular system
narrow space around midbrain in incisura
enlarged ventricular system and subarachnoid space
widened central canal
normal-pressure hydrocephalus (NPH)
chronic form of communicating hydrocephalus with equilibrium of CSF formation and absorption
SYMPTOM TRIAD: due to stretching of white matter from lateral ventricle dilation
progressive dementia (WACKY)
ataxic gait (WOBBLY)
urinary incontinence (WET)
typically seen in elders
ex vacuo ventriculomegaly or hydrocephalus ex vacuo
appearance of increased CSF on imaging but is due to decreased brain tissue and neuronal atrophy
found in individuals with alzheimer’s disease, dementia, huntington’s disease
hydrocephalus mimics this (due to both having ventricles that appear to be larger than normal)

ventriculoperitoneal shunt
most common treatment for hydrocephalus
cannula typically placed in frontal horn of lateral ventricle (due to lack of choroid) of non-dominant hemisphere (to avoid harming Broca’s area) to divert CSF into peritoneal cavity to be absorbed
over time, ventricles return to normal size and if used in children, head returns to normal size
endoscopic 3rd ventriculostomy
creating a foramina at the base of 3rd ventricle
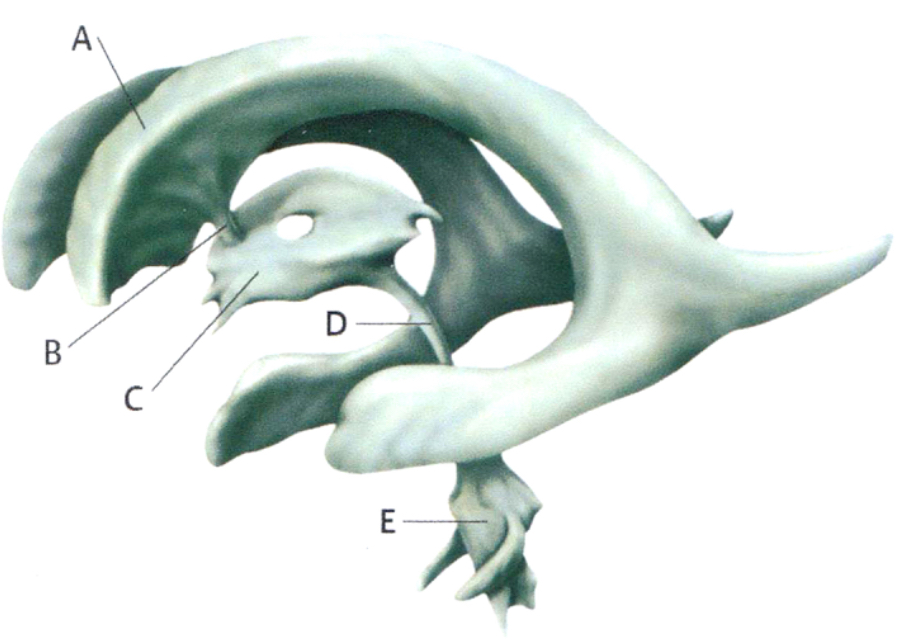
PI: CSF circulates within the ventricles and exits the ventricular system through 3 openings. which of the following labeled regions contains the three openings through which CSF leaves the ventricular system?
A
B
C
D
E
5
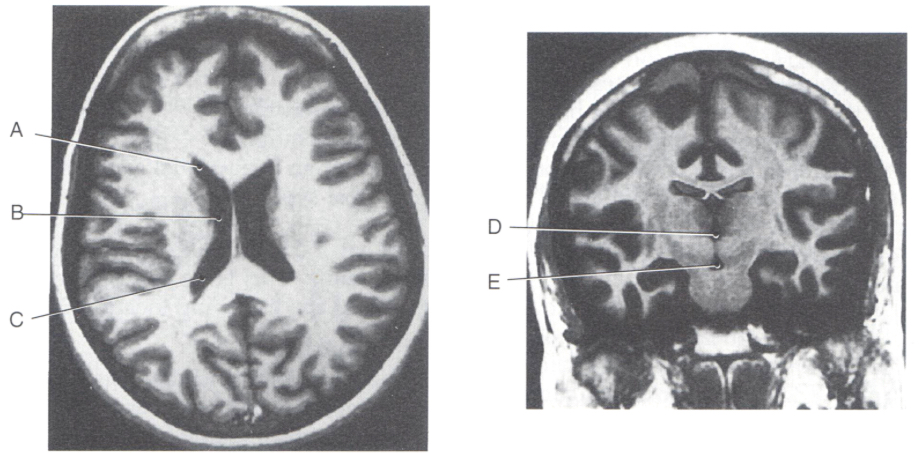
PI: a 43 y/o woman presents with headache and signs of increased ICP. MRI reveals a tumor in the body of the lateral ventricle. which of the following labeled areas most closely represents this part of the ventricular system?
A
B
C
D
E
2
PI: a first-year resident in radiology expresses concern over a mass lying within a ventricle. he is convinced that it is a tumor, which is filling up the ventricle and is encroaching on its lateral walls. to his surprise, e finds the patient has no neurological symptoms that can be correlated to a tumor. the attending, from his experience and location of the structure, explains that it could be the glomus of the choroid plexus. which of the following locations for the structure would confirm its diagnosis as the glomus?
anterior horn of lateral ventricle
body of lateral ventricle
trigone of lateral ventricle
inferior horn of lateral ventricle
roof of 3rd ventricle
3
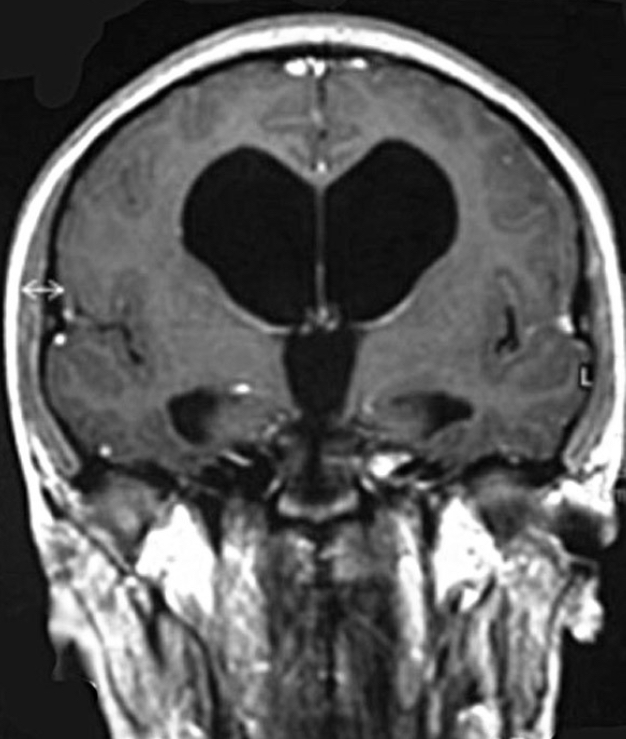
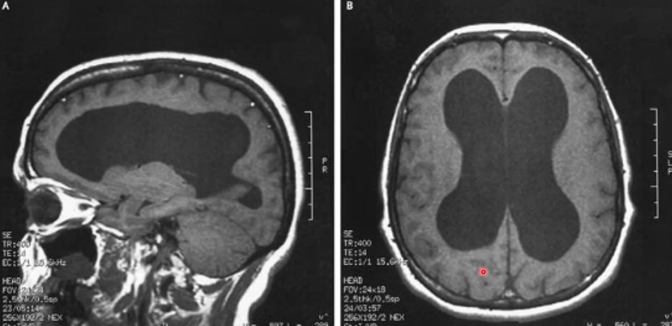
PI: a 24 y/o man becomes acutely ill and presents to the ER in a depressed level of consciousness. MRI of his brain reveals enlarged ventricles as shown here, the fourth ventricle appears normal.
right interventricular foramen
left interventricular foramen
both interventricular foramina
cerebral aqueduct
foramen of magendie
both foramen of luschka
4
PI: a 77 y/o man presents with gait disturbance, urinary incontinence, and dementia. MRI reveals that the ventricles are somewhat, and uniformly, enlarged, and lumbar puncture reveals the CSF pressure is within the normal range within the subarachnoid space. this man is most likely suffering from which of the following?
aqueductal stenosis
communicating hydrocephalus
noncommunicating hydrocephalus
normal pressure hydrocephalus
obstructive hydrocephalus
4
PI: an 18 y/o female was brought to the ER following a day of worsening headache, fever, periods of confusion, stiff neck. the patient’s roommate reported that she awoke at 3am with chills and body aches. by 11am, she was breathing quickly and had nausea and vomiting. a lumbar puncture was performed, and CSF analysis showed elevated white blood cells indicating meningitis. a subsequent scan revealed dilated ventricles. she is diagnosed with which of the following?
communicating hydrocephalus
noncommunicating hydrocephalus
normal pressure hydrocephalus
obstructive hydrocephalus
1