Ex 2; Peds Resp Assessment
1/28
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Most common cause of illness/hospitalizations in children
respiratory disorders
Upper respiratory tract
the nose or nostrils, nasal cavity, mouth, throat (pharynx), and voice box (larynx). The respiratory system is lined with a mucous membrane that secretes mucus.
Lower respiratory tract
consists of the trachea (windpipe), bronchial tubes, and lungs. The bronchial tubes carry air into the lungs and branch into smaller and smaller bronchioles. These end in alveoli (air sacs).
Pediatric Nose/Throat
Nose:
Newborns are obligatory nose breathers until at least 4-6 weeks of age.
Newborns produce very little upper airway mucus = more susceptible to infection
Newborns & infants have small nasal passageways = airway obstruction
Immature sinuses until 6-8 yrs
Newborns & infants are abdominal breathers.
Throat:
Tongue is proportionally larger.
Enlarged tonsil & adenoids until early school-age. = obstruction
Pediatric trachea
Airway diameter is smaller.
Muscles supporting the upper airway are less functional.
Mucus membranes less firmly attached.
Cricoid cartilage is underdeveloped until 10 years.
Larynx and glottis are located higher in the neck = risk for airway obstruction
Pediatric larynx
Larynx and glottis are located higher in the neck = risk for airway obstruction
Funnel-shaped larynx; narrower = risk for obstruction
Infant Chest Wall
flexible & does not support the lungs adequately.
Reduced functional capacity.
Lungs don’t recoil as well (air trapping).
Infants and toddlers are diaphragmatic breathers; If diaphragm movement is impaired (as in states of hyperinflation, such as asthma), the intercostal muscles cannot lift the chest wall and respiration is further compromised.
Lower respiratory characteristics
Bronchi and bronchioles are narrower.
Bifurcation of trachea is higher in children than in adults; This anatomic difference is important when suctioning children and when endotracheal intubation is required + increased risk for aspiration.
Fewer alveoli (reach adult number by 7 or 8 yrs) = greater risk of hypoxemia
Metabolic Rate & Oxygen Need
Higher metabolic rate than adults.
Resting respiratory rates are faster.
Demand for O2 is higher (6-8 L/min compared to adults 3-4 L/min).
Rapid development of hypoxia and distress .
Atopy
a predisposition to an immune response against diverse antigens and allergens, genetic tendency toward asthma, allergic rhinitis, or atopic dermatitis.
Respiratory Health History Questions
consists of the past medical history, family history, and history of present illness (when the symptoms started and how they have progressed), as well as treatments used at home.
Recurrent colds or sore throats? History of recurrent respiratory illnesses or chronic lung disease?
Atopy hx?
Prematurity? Respiratory dysfunction at birth?
Poor weight gain? Nutrition? Diapers?
Family hx of respiratory disorders? Exposure to second-hand smoke?
Onset and progression, fever, nasal congestion, noisy breathing, presence and description of cough; rapid respirations; increased work of breathing; ear, nose, sinus, or throat pain; ear pulling; headache; vomiting with coughing; poor feeding; and lethargy.
Pediatric Respiratory Assessment
Skin color (pink, warm, dry)
Rate and depth of rr
Nose and oral cavity; Note nasal drainage and redness or swelling in the nose. Note the color of the pharynx and tonsil size.
Cough and other airway Noises; cough wet or dry, stridor or wheezing, grunting?
Respiratory effort; labored?
Retractions; (the inward pulling of soft tissues with respiration) can occur in the intercostal, subcostal, substernal, supraclavicular, or suprasternal regions → mild, moderate, or severe.
Anxiety and restlessness
Clubbing; the result of increased capillary growth as the body attempts to supply more oxygen to distal body cells.
Hydration status; fontanele, skin turgor, mucous membranes, urine output, tearing
paradoxical breathing
lack of simultaneous chest and abdominal rise with the inspiratory phase.
respirations are very ineffective for ventilation (gas exchange) and oxygenation (binding of oxygen). The chest falls on inspiration and rises on expiration.
Physical Assessment Abnormals
Retractions
Tachypnea
Nasal flaring
Head bobbing
Noisy breathing
Grunting
Cough
Hypotonia
Lethargy
Cyanosis
First sign of respiratory Illness in Infants
tachypnea (increased respiratory rate for age).
Respiratory Assessment: Auscultation
Listen over anterior AND posterior chest, as well as axillary areas.
Inspiratory phase is usually softer & longer than expiratory phase.
Always auscultate again after a cough, nasal clearing or suctioning.
Respiratory Assessment: Percussion (tapping)
Abnormals:
flat,
dull,
tympany,
hyperresonance
Respiratory System: Palpation
Sinuses for tenderness in the older child
Enlargement of lymph nodes
Tactile fremitus (pneumonia or pleural effusion)
Central and peripheral pulses (quality and rate)
Capillary refill
Immature nervous system
predisposes to airway complications
Parasympathetic Tone
hypoxia causes bradycardia
bradycardia causes hypotension
bradycardia worsens hypoxia
Scared Children Cry resulting in
increased secretions
increased airway irritability
increased risk of larygnospasm
increased risk of wheezing
increased risk of airway edema
Stress
increases metabolic rate; increases WOB, HR, BP, temperature
Children are Easily Sedated because
immature neurons
less myelinization
weak blood-brain barrier
little prior exposure to drugs
increased risk of respiratory depression
Arterial blood gases (ABGs)
Invasive method (requires blood sampling) of measuring arterial pH, partial pressure of oxygen and carbon dioxide, and base excess in blood.
Nursing Implications:
Hold pressure for several minutes after a peripheral arterial stick to avoid bleeding.
Radial arterial sticks are common and can be very painful.
Note if the child is crying excessively during the blood draw, as this affects the carbon
Fluoroscopy
Radiographic examination that uses a fluorescent screen—“real-time” imaging for the identification of masses/abcesses
Nursing implications:
Requires the child to lie still.
Equipment can be frightening.
Children may respond better to presence of parent or familiar adult.
Peak expiratory flow
Measures the maximum flow of air (in L/s) that can be forcefully exhaled in 1 second; Daily use can indicate adequacy of asthma control.
Nursing implications:
It is important to establish the child’s “personal best” by taking twice-daily readings over a 2-week period while well.
The average of these is termed “personal best.”
Charts based on height and age are also available to determine expected peak expiratory flow.
Pulmonary function tests
Measure respiratory flow and lung volumes; used for Asthma, cystic fibrosis, chronic lung disease.
Nursing implications:
Usually performed by a respiratory therapist trained to do the full spectrum of tests.
Spirometry can be obtained by the trained nurse in the outpatient setting
Sweat chloride test
Collection of sweat on filter paper after stimulation of skin with pilocarpine. Measures concentration of chloride in the sweat. Indicated for for cystic fibrosis.
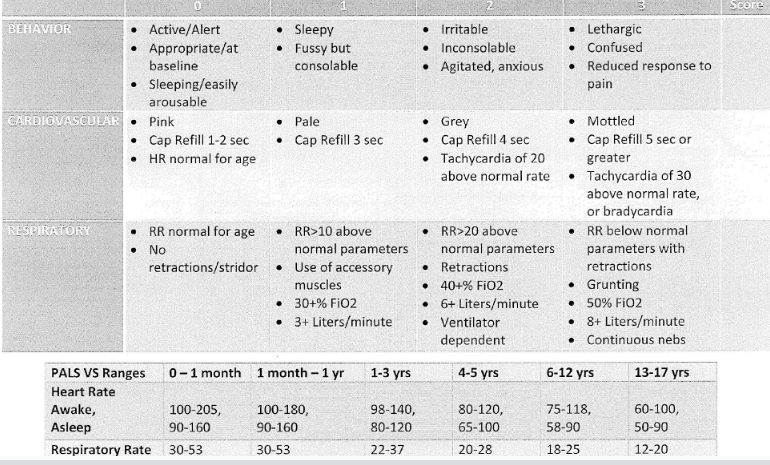
Pediatric Early Warning Score (PEWS)