Lec 9: Glucose regulation, Diabetes
1/78
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
79 Terms
what do endocrine organs do
synthesize & secrete hormones
endocrine=hormones released into bloodstream
paracrine=into adjacent tissue only ex histamine
many have a long half life (=> kinetics: likely highly PPB, ex T4 hormone)
what is endocrine secretion triggered by
concentration of specific substances ex glucose
neural stimulation ex SNS & epinephrine
endocrine sequences ex epinephrine => aldosterone
what is endocrine secretion regulated by
negative feedback mechanism
how can we test endocrine fx
hormone level or the affector-substance level
ex glucose (indirect test of insulin function), T4 (direct hormone level test)
what are the 2 diff dysfunctions of the endocrine system, why do they exist
hyposecretion or hypersecretion
d/t primary endocrine disorder, signaling disorder, sequence disorder
s&s will be directly related to excess or deficit of the expected hormone level
hyposecretion causes
congenital defect
disease/infection/inflammation
hypoperfusion
ageing
hypersecretion causes
genetic
tumours (hypo or hyper)
environmental stimuli
what are the primary energy sources of the body
glucose (readily distributed)
fatty acids (fat)
what is the most needy system for glucose
CNS (brain)
requires constant supply of glucose (broken down: CO2 & H2O)
cannot store it for later
what is extra glucose stored as
as glycogen (liver, muscles) & triglycerides (adipose cell)
if there is a fall in blood glucose (BG), what happens aka what are names of the processes of glucose formation/breakdown
=> glycogen breakdown via glycogenolysis (triggered by glucagon hormone)
formation of more glucose from other sources gluconeogenesis, released PRN
how are fatty acids distributed, who cant use it and what is it stored as
via lymph to circulation
CNS & RBCs cannot use fatty acids
extra FAs=stored as triglycerides
what are fatty acids broken down into
3 fatty acids & glycerol
glycerol can be broken down via glycolytic pathway into glucose
fatty acids are NOT converted into glucose - cant be used by the brain for energy
fatty acid metabolism in liver => ketone metabolites
what is insulin def
pancreatic hormone (endocrine)
synthesized in beta cells (Langerhans)
main action is to move glucose
what are the fxs of insulin
glucose cellular uptake
promotes storage formation (glycogen/triglyceride/protein synthesis)
prevents glycogen & fat lysis (in order to 1st use glucose) & protein lysis (to preserve tissues)
amino acid cellular uptake; triglyceride adipose cell uptake
where is glucagon synthesized
synthesized in alpha cells = opposite of Insulin
what are the fxs of glucagon
promotes mobilization of stores:
glycogenolysis (glycogen breakdown)
gluconeogenesis (amino acid conversion into glucose)
lipolysis (triglyceride breakdown)
what is glucagon triggered by
low plasma glucose levels (between meals, hypoglycemia)
=> mobilize stores and replenish blood glucose for cellular use
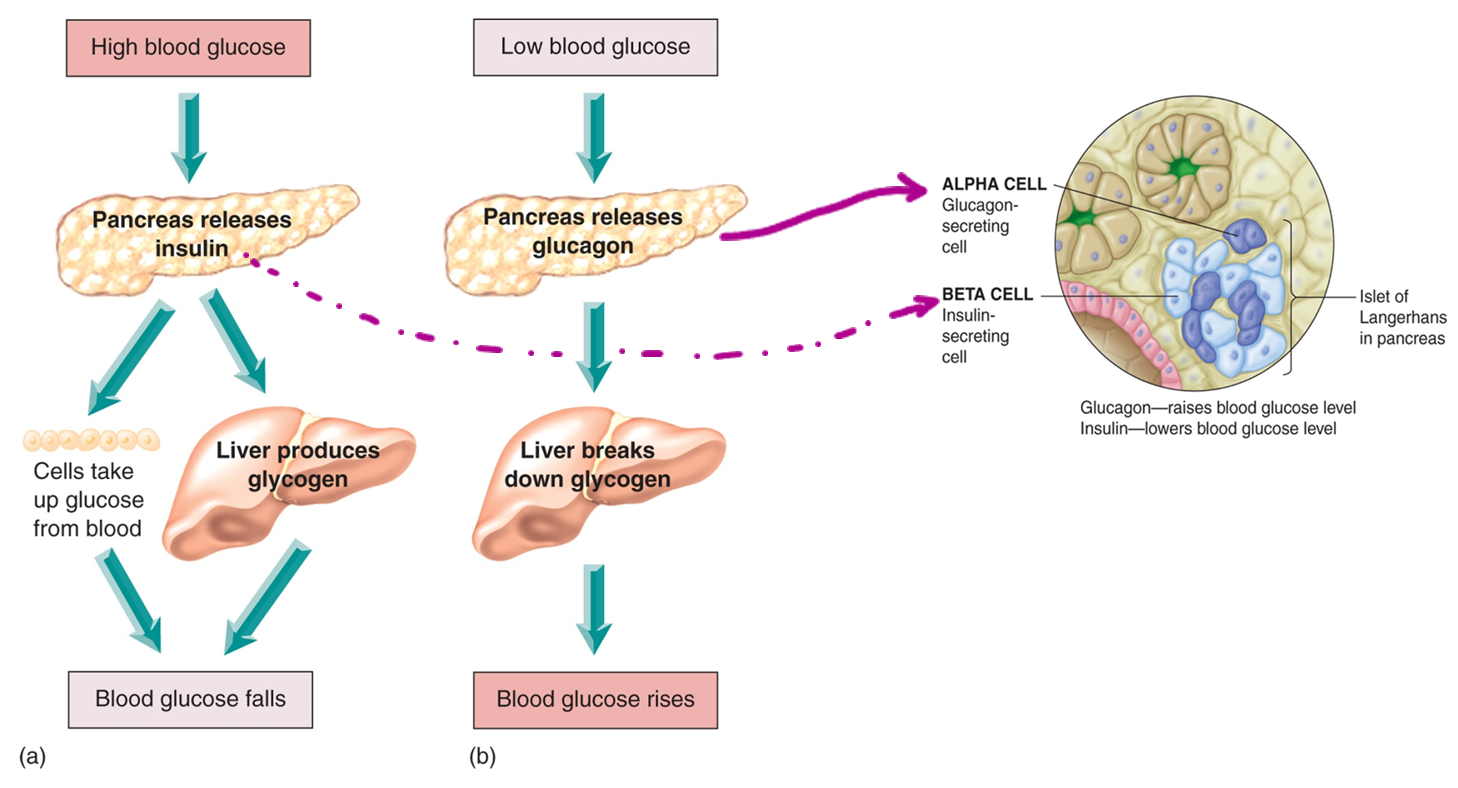
glycemic regulation for low BG and high BG
high BG=pancreas releases insulin, liver produces glycogen/cells take up glucose from blood=low BG
low BG=pancreas releases glucagon, liver breaks down glycogen=high BG

what is the simulant of insulin synthesis
high serum glucose
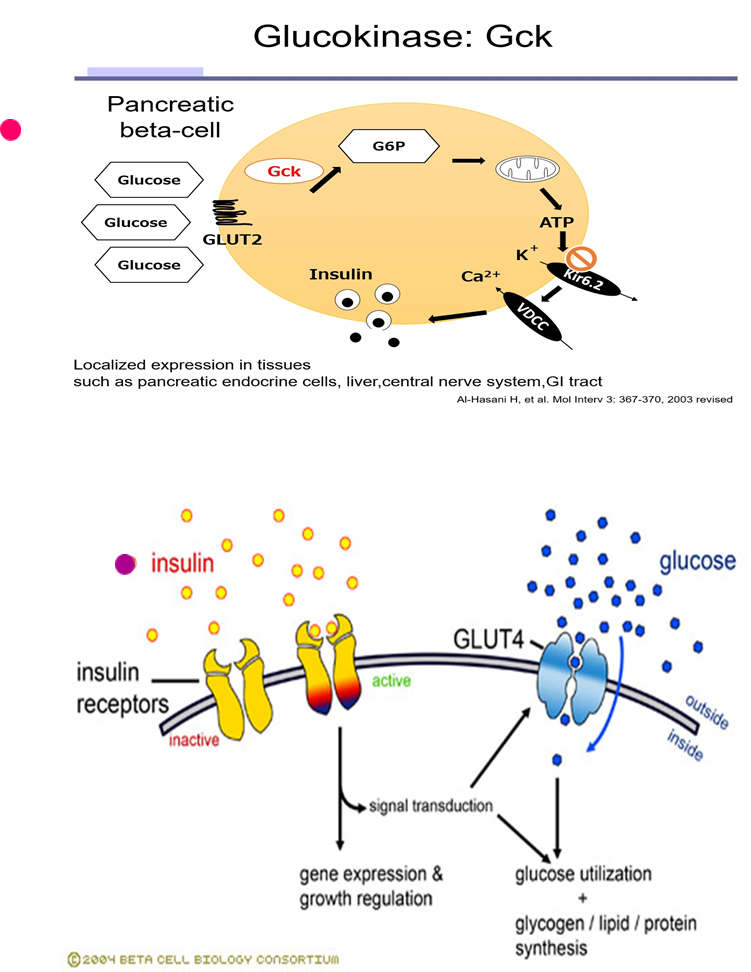
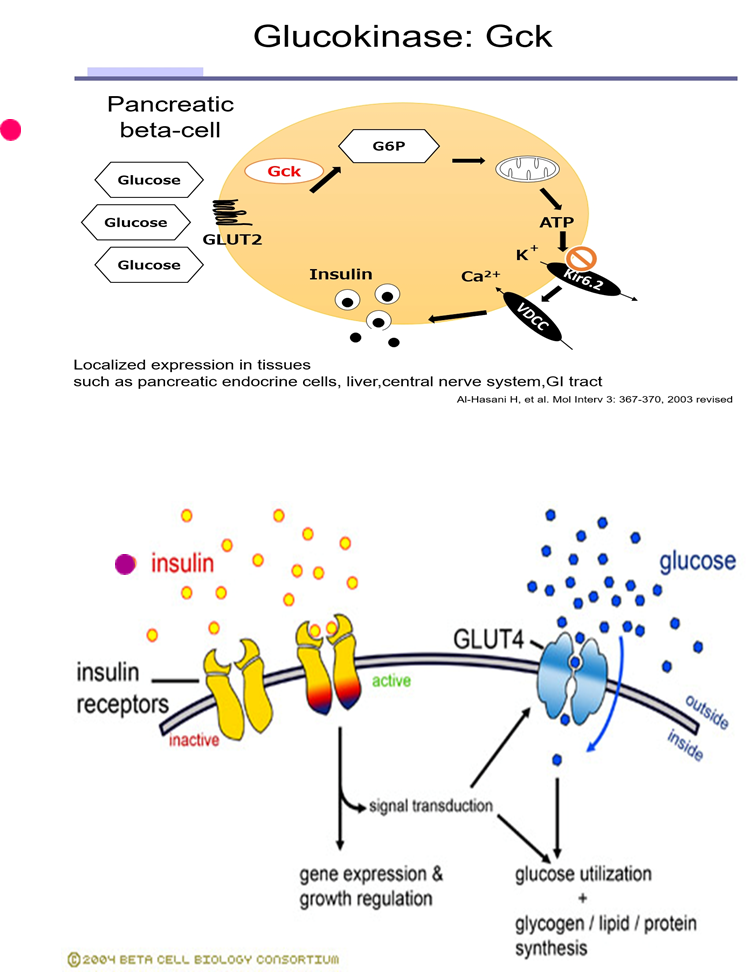
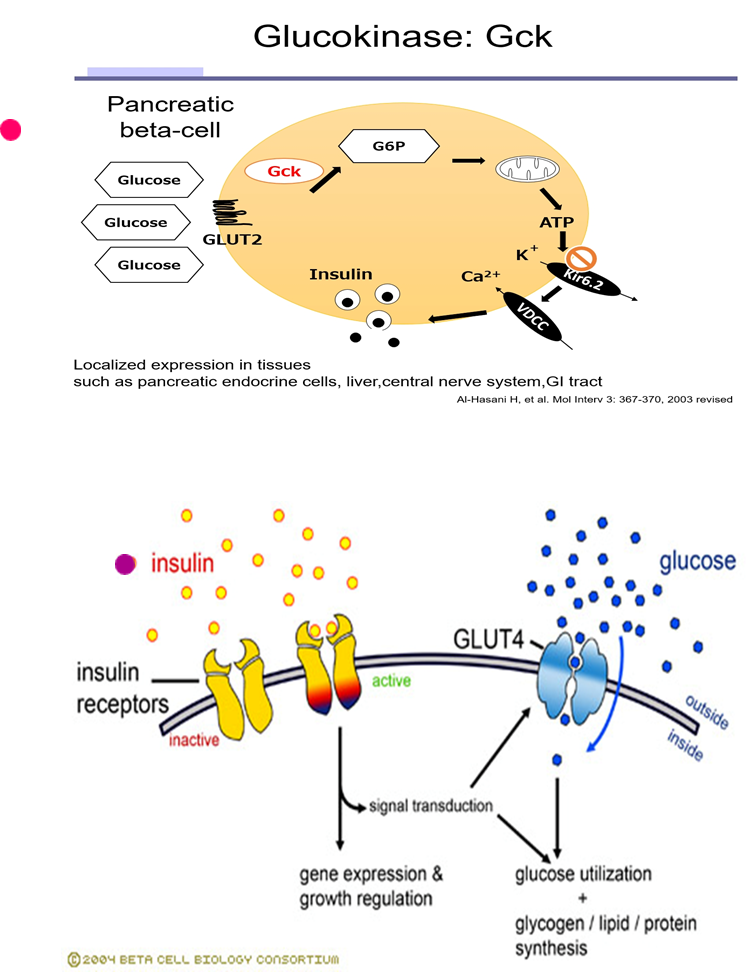
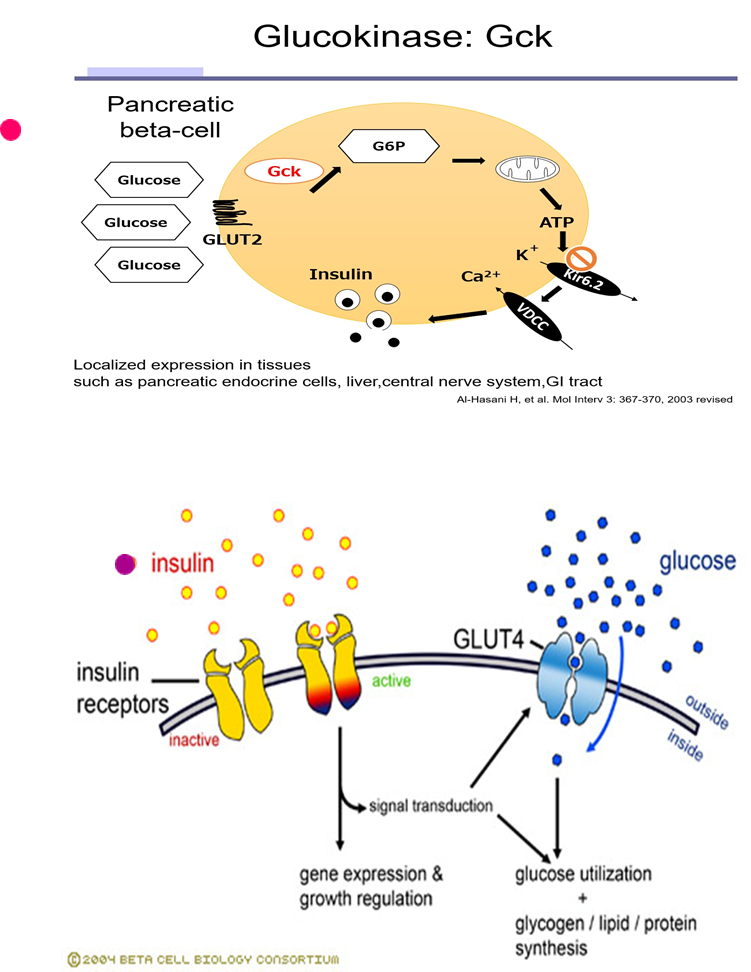
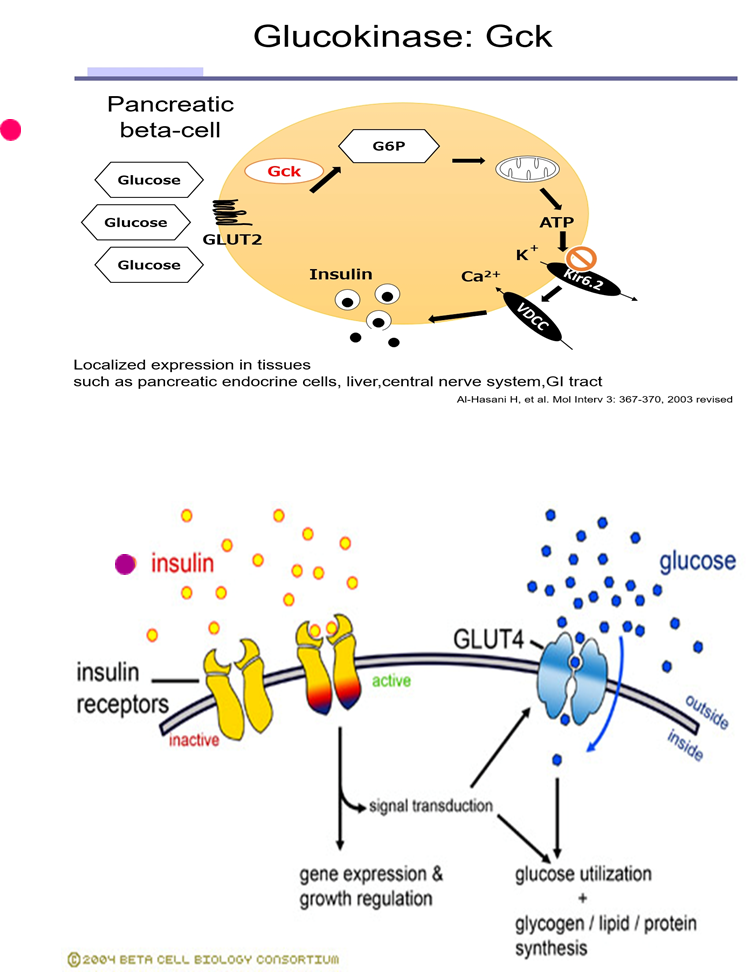
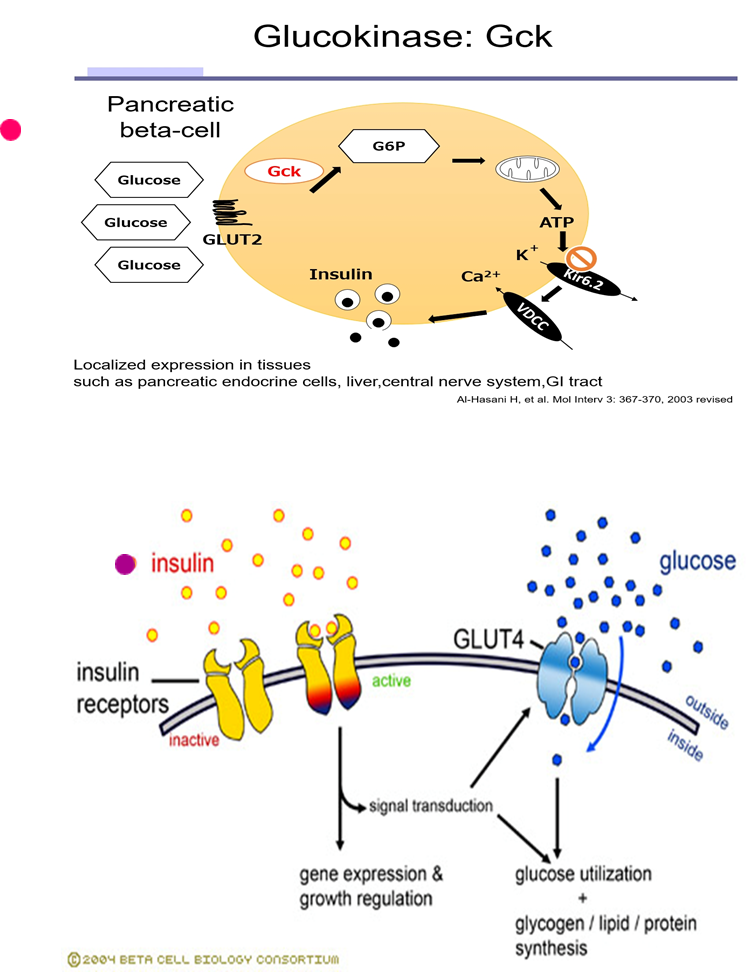
what is the pathophysiology pathway of insulin release
glucose enters pancreatic beta cell via glucose transporter => metabolized via glucokinase into ATP => closes K channels (on Beta cell) => depolarization => insulin secretion (from pancreas)
=> insulin from pancreas enters hepatic circulation => 50% 1st pass metabolized => metabolites re renally excreted
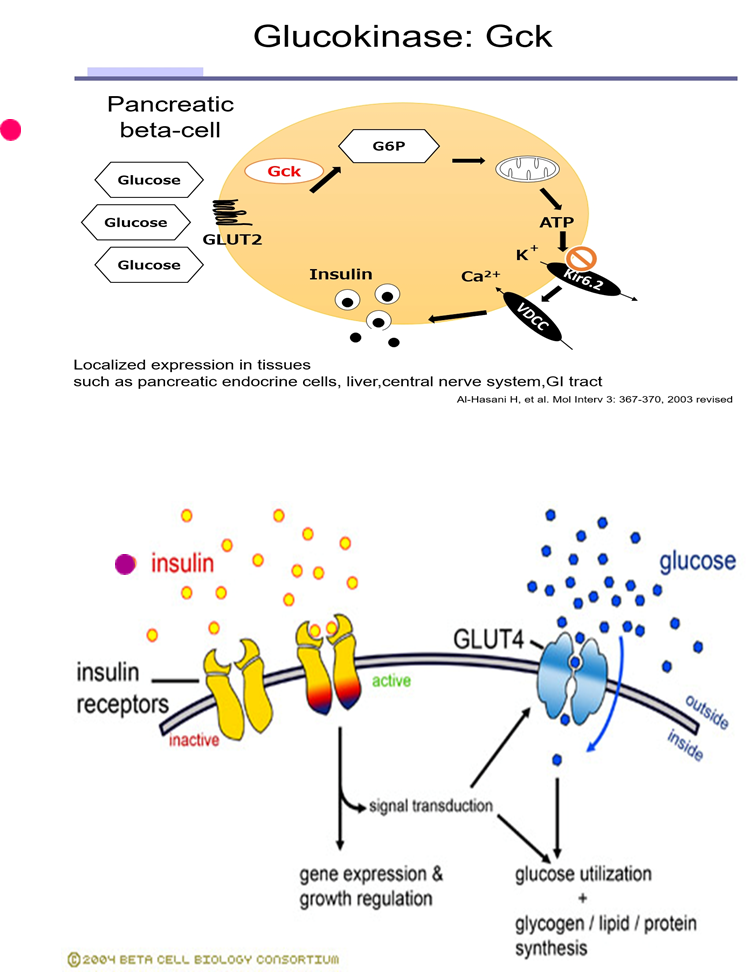
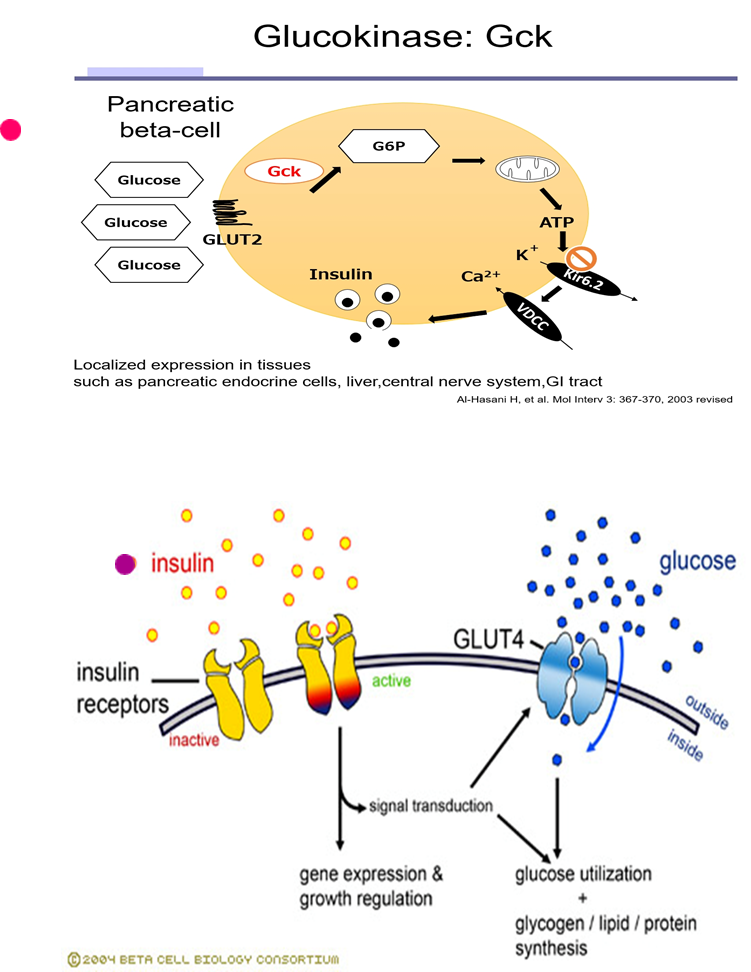
what is insulins action/what does it bind to
binds to cellular membrane receptor (tyrosine kinase) => activates kinase enzyme within cell => stimulates glucose transporter channels to open to glucose
what is insulins inhibition
somatostatin (D cell produced)
what are the immediate effects of beta cell destruction
disabled transport of glucose into cells => dysfunction of glucose, fat, and protein metabolism
Pathophysiology sequelae of beta cell destruction aka pathway
increased glucose in plasma (hyperglycemia) =>
high solute concentration (polydipsia/thirst stimulated) =>
osmotic shift of fluid into circulation (increased osmotic pressure)= cellular dehydration
high solute concentration in renal tubules
=> osmotic shift into filtrate = high urine production (polyuria stimulated)
therefore=hyperglycemia, polydipsia, polyuria, glycosuria (glucose in urine)
after hyperglycemia; polydipsia; polyuria; glycosuria (glucose in urine) happens from beta cell destruction, what happens next
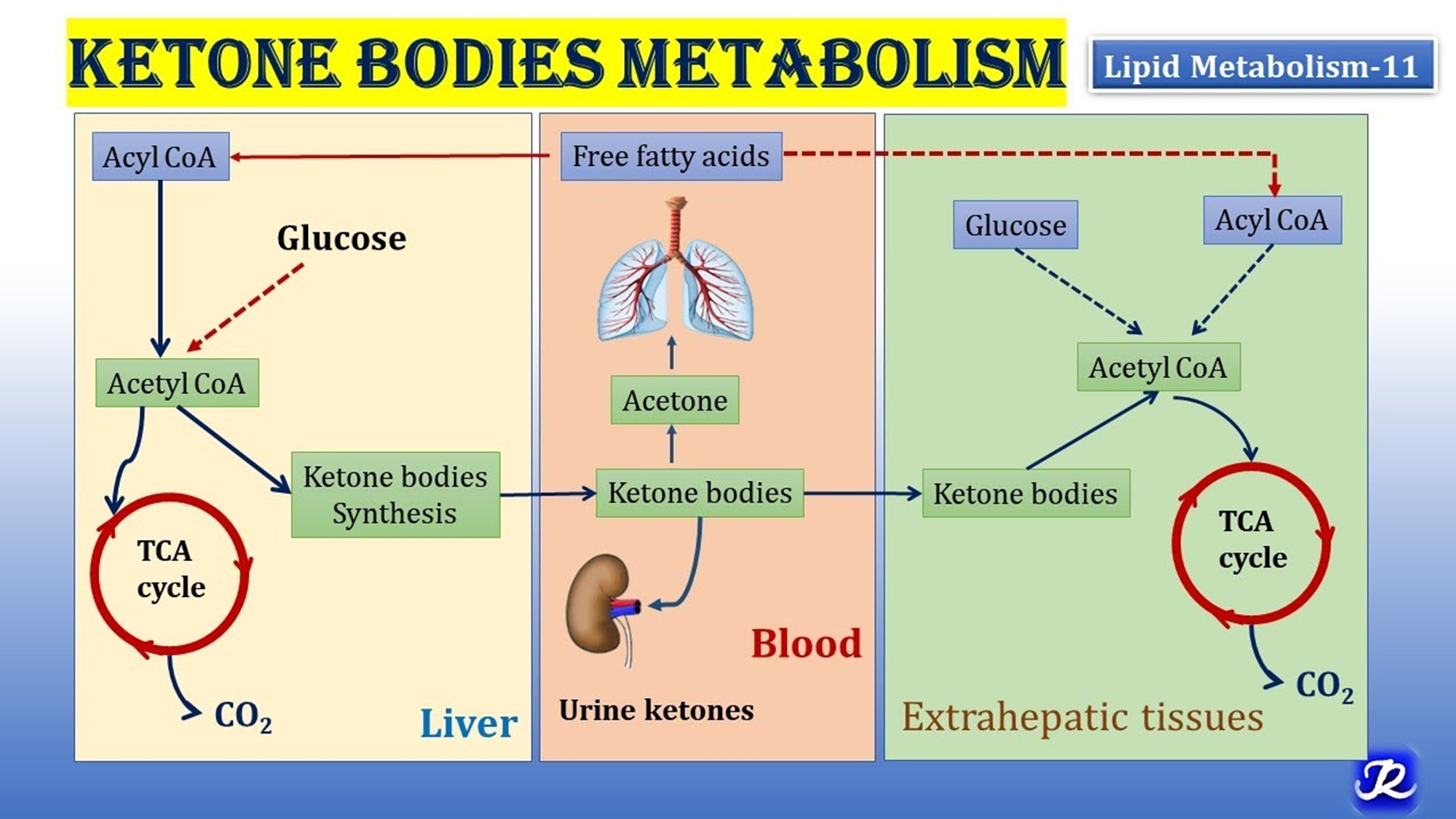
=> metabolic shift to use fat for energy = breakdown of triglycerides & glycerol
=> hepatic metabolism of fatty acids => ketones (ketone bodies) produced as byproduct
therefore=ketonuria, changes in LOC, acetone breath (sweet), metabolic acidosis, coma, death
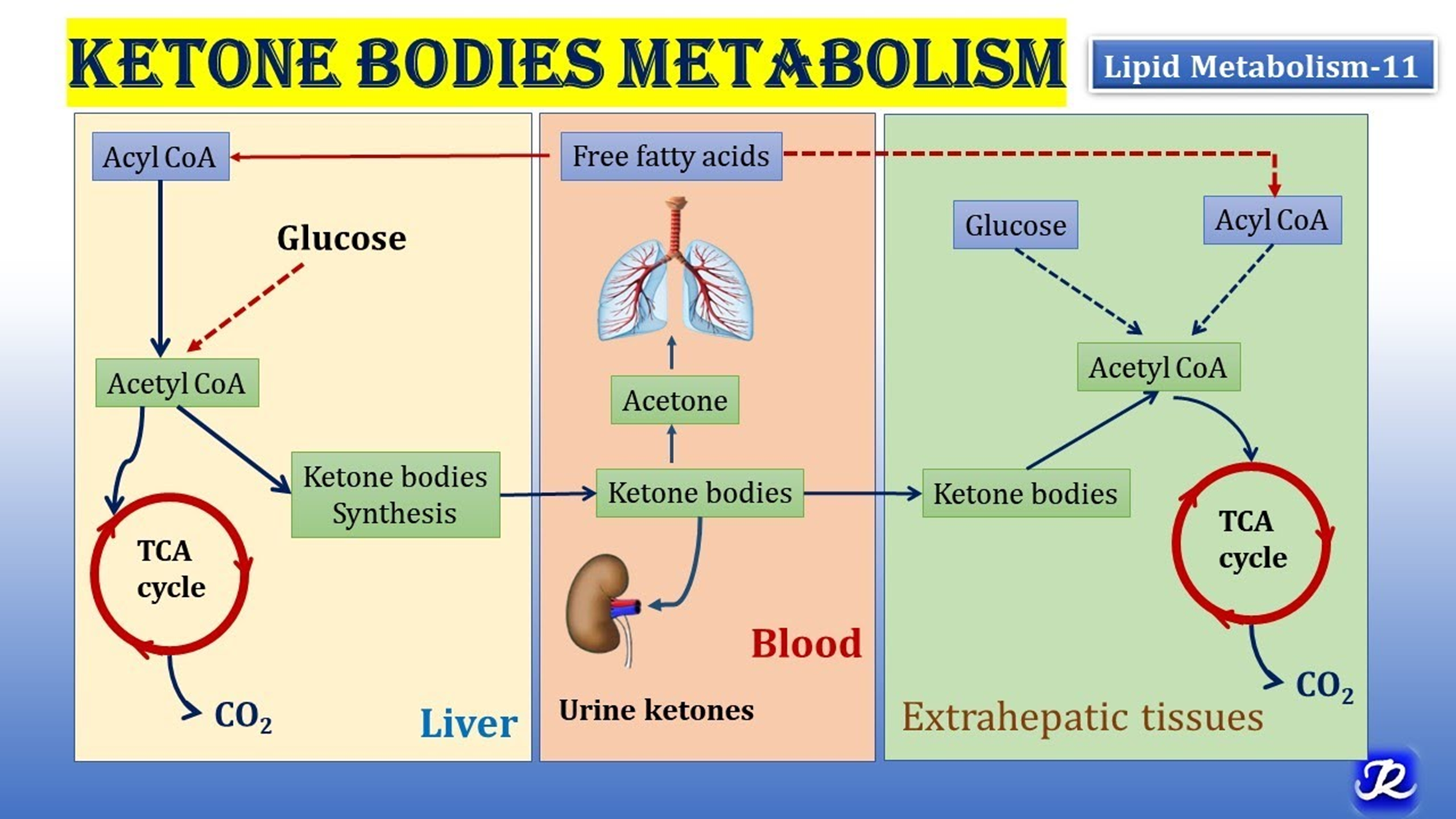
ketones consequences
are acidic => accumulation causes metabolic acidosis + metabolism produces acetone
=high blood glucose, drops pH of blood
what are the energy subsitutes when glucose uptake is reduces (consequences)
lipolysis (fatty acid breakdown)
liver metabolism fatty acids (fatty acid oxidation)= ketones & ketonuria
proteolysis (next phase)= weight loss & muscle wasting
what are all the altered cellular functions from reduced glucose uptake (consequences)
insulin resistance (when insulin given=no immediate results, takes a few hrs)
altered cellular repair
endothelial dysfunction + decreased angiogenesis
increased oxidative stress => inflammatory consequences, risk for clotting
organ injury=retinopathy, neuropathy, nephropathy (kidneys), CV
how do we diagnose diabetes mellituse, what is the normal range
fasting glucose
>7 mmol/L (normal <6)
dx usually pre-30 yrs of age (toddlers, teens)
what are the diff types of diabetes mellitus
type 1A
type 1B
type 1A diabetes mellitus causes
genetic predisposition + triggering event (ex infection, trauma) => immune reaction to beta cell antigens = autoimmune
most common
type 1B diabetes Mellitus causes
idiopathic (familial), rare
DM tx and ultimate effect
total destruction of beta cells: IDDM (insulin dependent), pt wont be able to make glucose
tx=insulin
if no tx=diabetic ketoacidosis = death
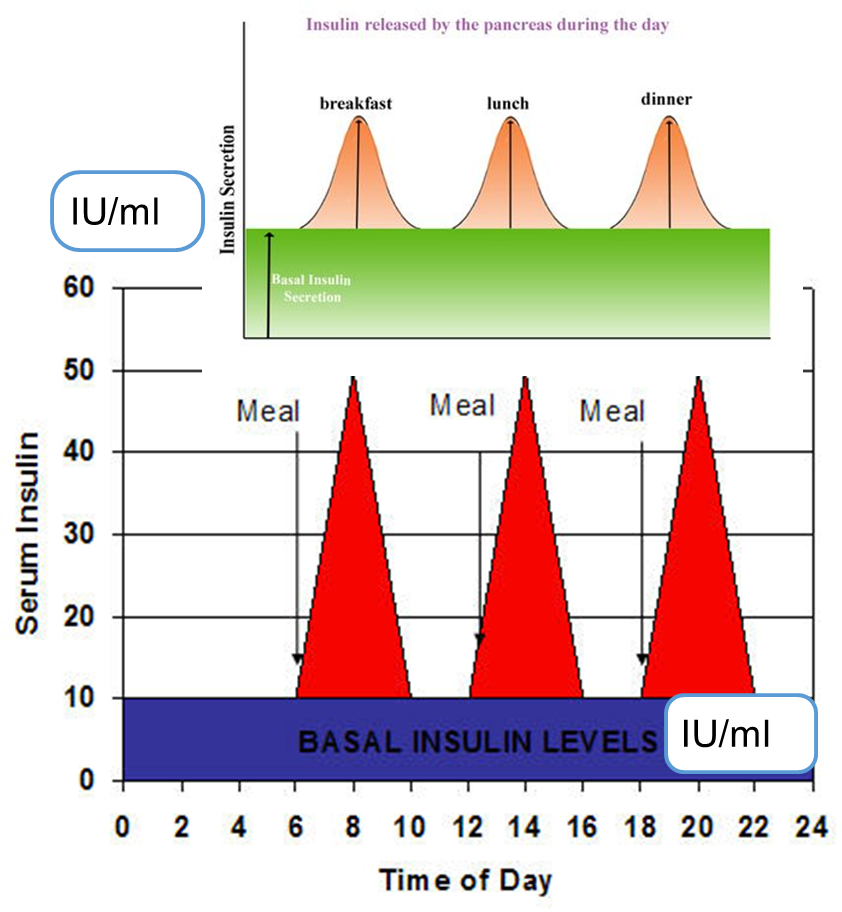
what is insulin always measured in
units (IU/ml)
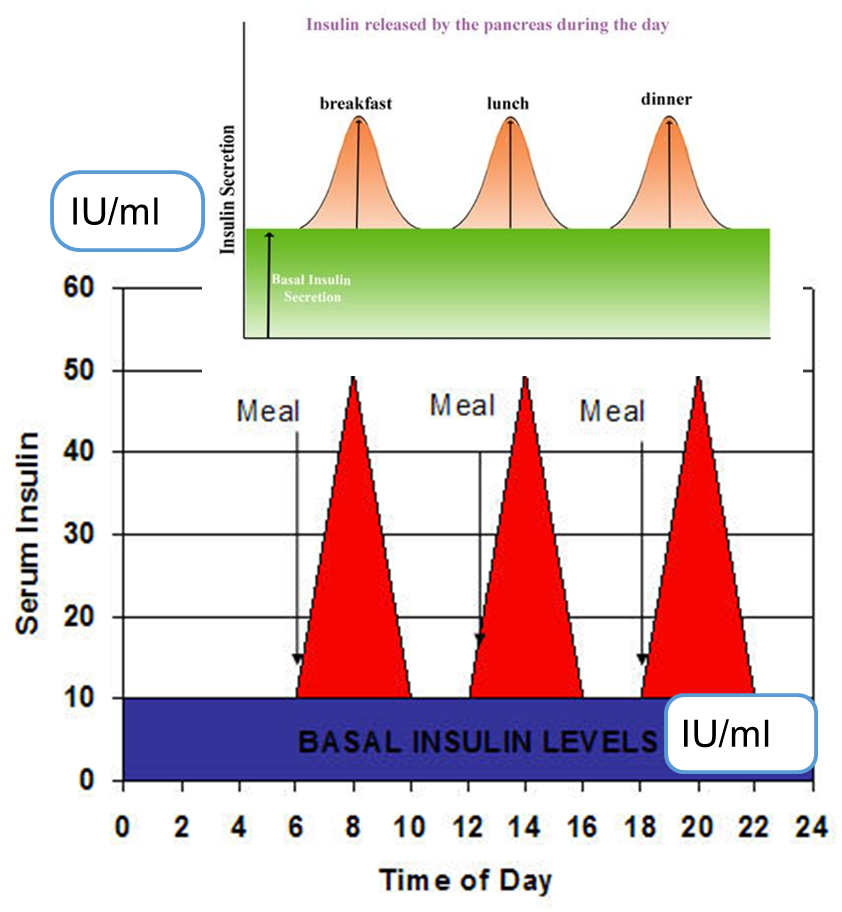
Endogenous insulin levels
basal level = 5-15 IU/mL aka cruise control
peak level = 60-90 IU/mL, booster at meals
clinically BG is measured, normal level = 4-8 mmol/L
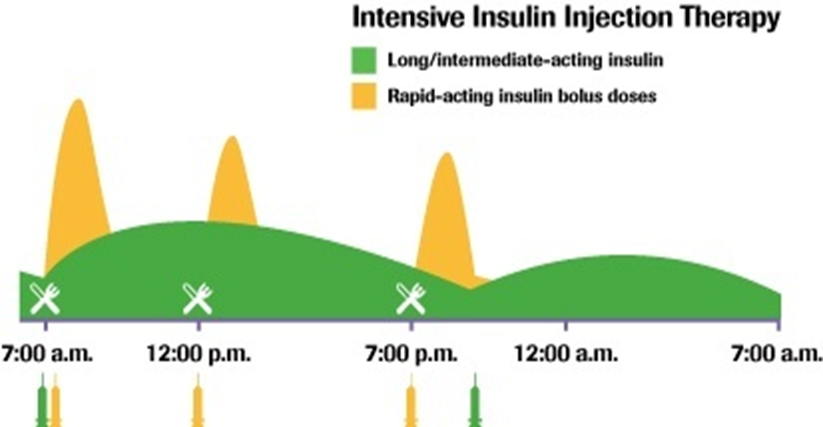
tx with exogenous insulin focuses on mimicking basal & peak
Tx with Insulin goal
restore normal glucose patterns
mimic basal & peak endogenous levels
minimize risk of hypoglycemia
what are the 4 diff preparation categories for insulin
rapid acting
long acting
short acting (regular)
intermediate acting (NPH)
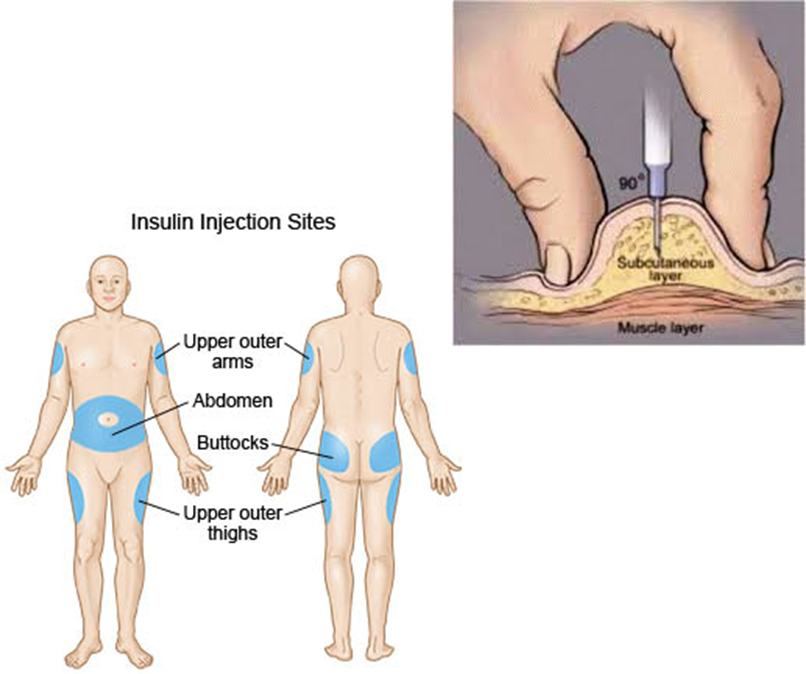
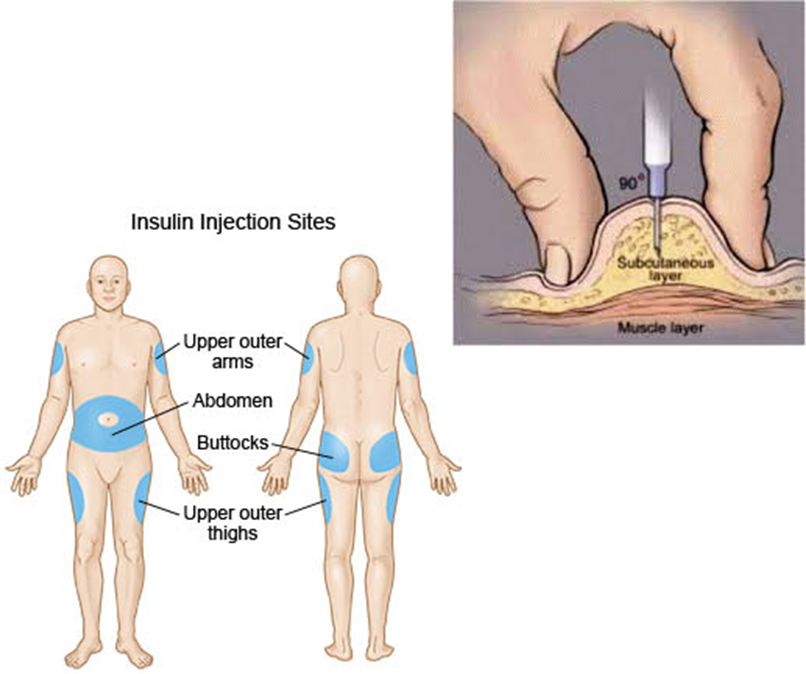
insulin administration methods
SC (into hypodermis)
SC needle injections
portable pen injectors (usually for pt, we dont use it)
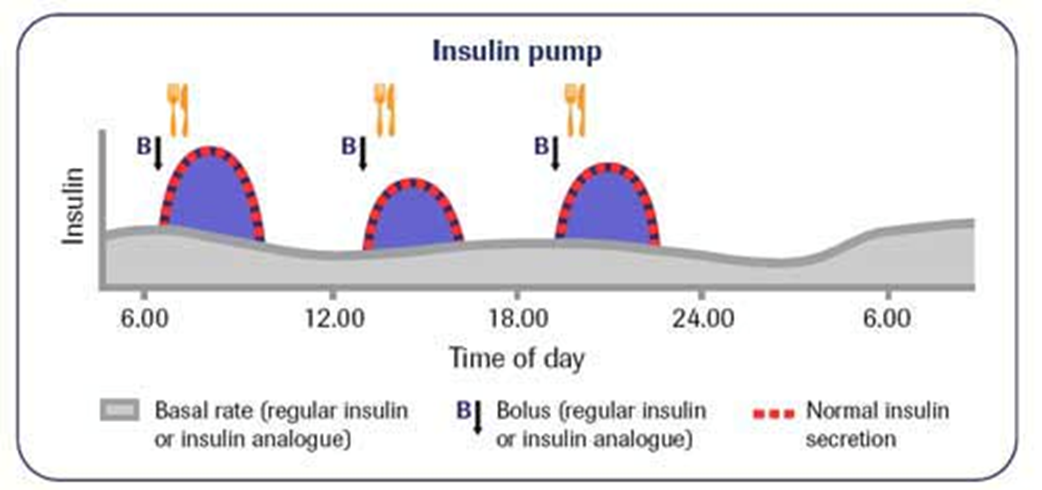
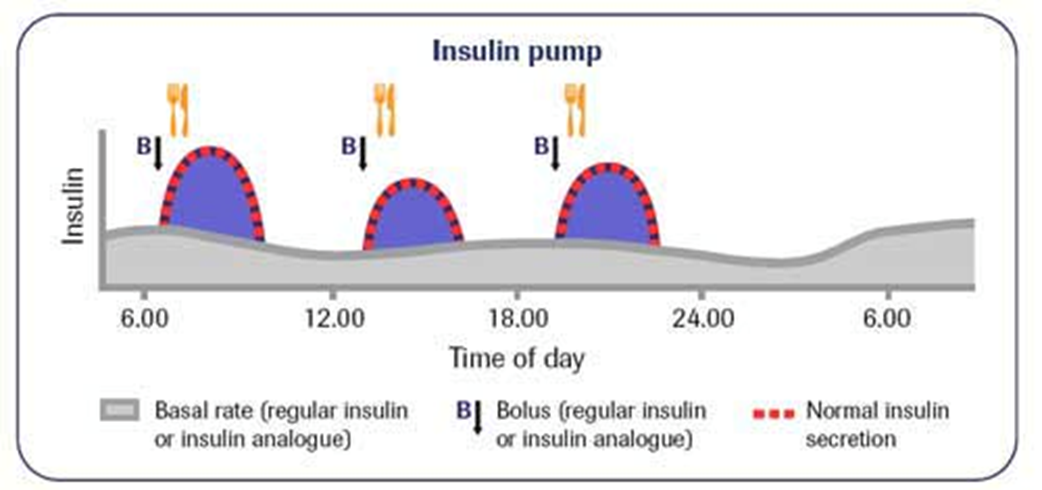
insulin pumps – basal & bolus delivery
IV=utilized in critically ill patients
rapid acting insulin qualities
onset=10-15 mins
peak=1-2 hr
duration=3-5 hrs
rapid acting insulin, who is it used for
meal-time bolus, pt eats right away! (food tray ready); the insulin for insulin pumps
not given IV
dose per carbohydrate content + BG pre-meal
check BG 1-2 hr post (to check peak)
give glucose IV if pt cant eat
list drugs of the rapid acting insulin
humalog (Lispro)
novorapid (Aspart)
apidra (Glulisine)
fiasp (Aspart) more fast acting/4 min
‘Rapid acting’ insulin in pumps: meal time boluses requirements
per carbohydrate content
check BG pre-meal
check BG 1-2 hr post
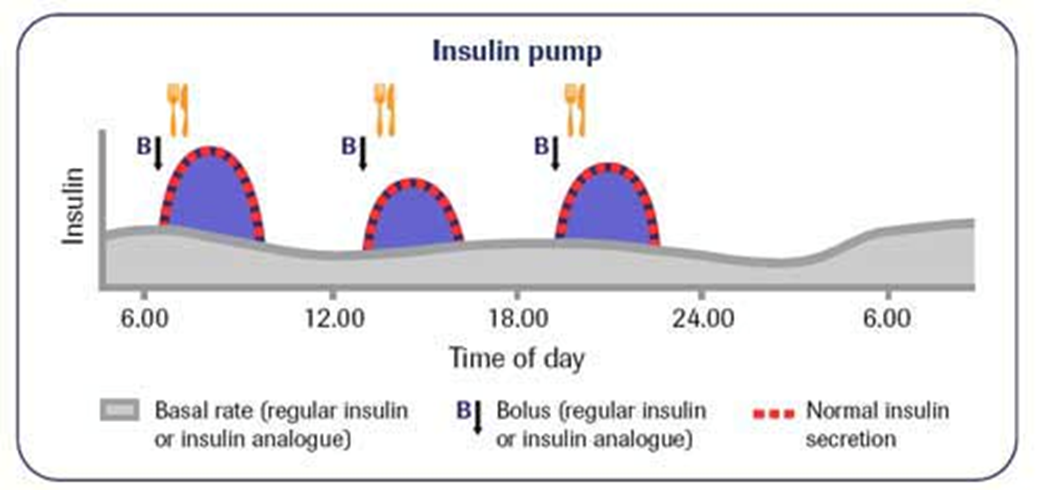
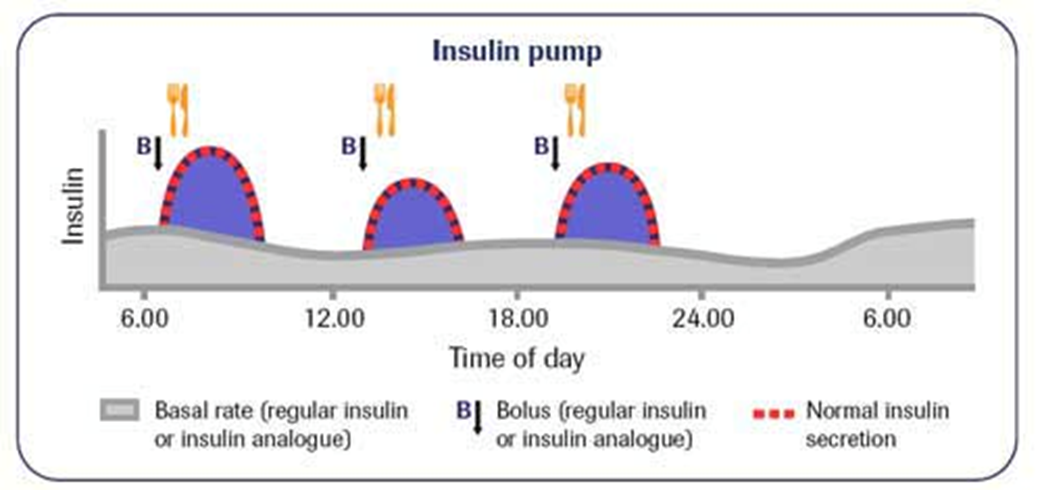
‘Rapid acting’ insulin in pumps: basal insulin requirements
continuous, slow infusion of rapid acting insulin over 24 hrs
check bedtime BG (usually tells us if too much or little)
IF BG rises too much overnight => risk of nighttime hypoglycaemia= adjust basal insulin dose
Long acting Insulin qualities and use
onset 90 min
plateaus for up to 24 hrs
ideal for background, admin, 1-2 x daily (consistency is important)
never IV
adjust dose according to bedtime BG level
list long acting insulin drugs
levemir (Detemir)
lantus (Glargine)
tresiba (Degludec) ultra-long acting, 30hrs
Short acting Insulin (‘regular’) qualities
onset 30 minutes
peak 2-3 hr
duration 6.5 hrs (dose dependent!)
short acting insulin use
ideal for meals (must be 30-45 min pre-meal!) BUT issues with hypoglycemia & balancing dose w intake (peak is later)=ensure pt eats (proteins and fats)
used IV if ketoacidosis, new dx, stabilizing pt in hospital
list short acting insulin drugs
novolin ge Toronto
Humulin R
Entuzity (KwikPen) 5x more concentrated
intermediate acting insulin qualities
onset 1-3 hrs
peak 5-8 hrs
duration up to 18 hrs (dose dependent!)
intermediate acting insulin use
ideal for background replacement, admin, 1-2x daily, if pt on steroids
can match sugar peaks, monitor for night hypoglycemia!!! (evening snack important)
never IV
list intermediate acting insulin drugs
humulin N
novolin ge NPH
intensive insulin Tx requirements, general guide: for Insulin Therapy & Insulin dosing for DM I: (what is the daily insulin requirements)
estimated daily insulin req (U) = 0.55 (U) x pt wt (kg)
estimate=does not factor in BMR, activity/stress, food, is a starting point only
approx 40% of estimate=basal
other 60% estimate=boluses (meal time)
what is the bolus insulin dosage based on when treating DM
BG (pre-meal level)
carbohydrate content/meal
what is the basal insulin dosage based on when treating DM
estimate
bedtime BG level
am administration preferred, avoids nighttime hypoglycaemia
similar amount each day, as long as the bedtime BG is normal
given even if pt NPO
IF pt on insulin pump, the basal dose is continuously delivered (fast acting insulin)

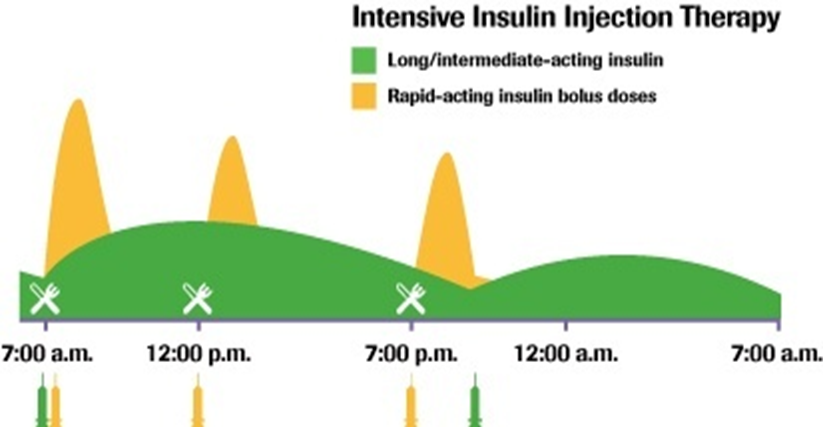
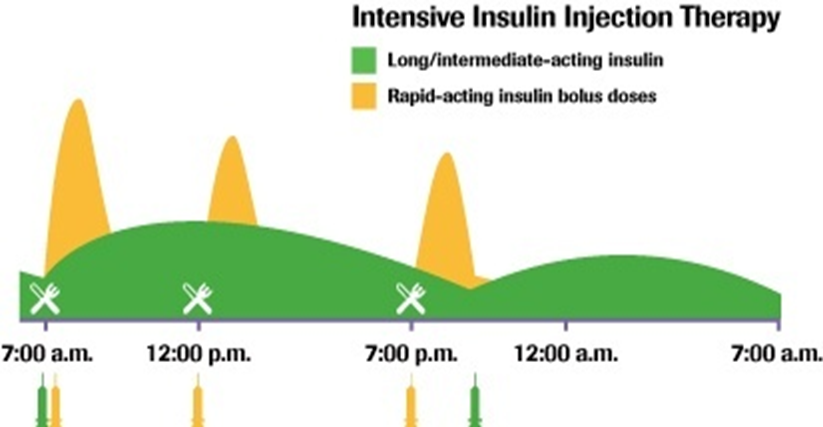
Daily routine: BG monitoring & Insulin administration, what does BBIT stand for
B=basal (long acting insulin) in am
B=bolus (short/rapid acting insulin) @ meals
I=insulin correction (short/rapid acting) if necessary (based on BG post-meal)
T=titrate doses to achieve glucose levels 4-8 mmol/L (monitor glucose throughout the day)
what times do we check blood glucose levels
pre-each MEAL
post-meals 1-2 hrs (new dx!)
at bedtime
4x per day is minimum requirement
8x for newly diagnosed pts (pre+post meals; bedtime; nighttime)
Diet in DM matters for accurate bolus dosing, what do we measure
carbohydrate intake counting:
carb counting, average 45-60 g/meal
carb total - fibre = total count (fibre isnt absorbed=no glucose)
15 g of carbohydrate=1 unit rapid acting insulin (on average across lifespan)
Regular meals & snacks are key to steady BG, what are the recommended strategies/foods
low GI foods, balanced diet with protein intake
bedtime snack to avoid night time hypoglycaemia
regular activity/exercise
insulin bolus recommendations pre meal
rapid or short acting insulin pre-meals (3x per day)
know the approx estimate from original calculation
pre-meal BG level
carb-count for this meal
BOLUS in IU (units) - administer before eating
what is the important rule for pre meals insulin bolus,
1 IU Insulin decreases BG by approx 2-5 mmol/L
on average by 2.5 mmol/L
used to decrease high BG, give at same time as normal dose
what do we do after administering insulin for a meal
check BG 1-2 hrs post-meal (at peak action), goal=4-8 mmol/L = normal
insulin correction & titrate:
10 mmol/L = require additional insulin
<4 = too much insulin, require additional sugar
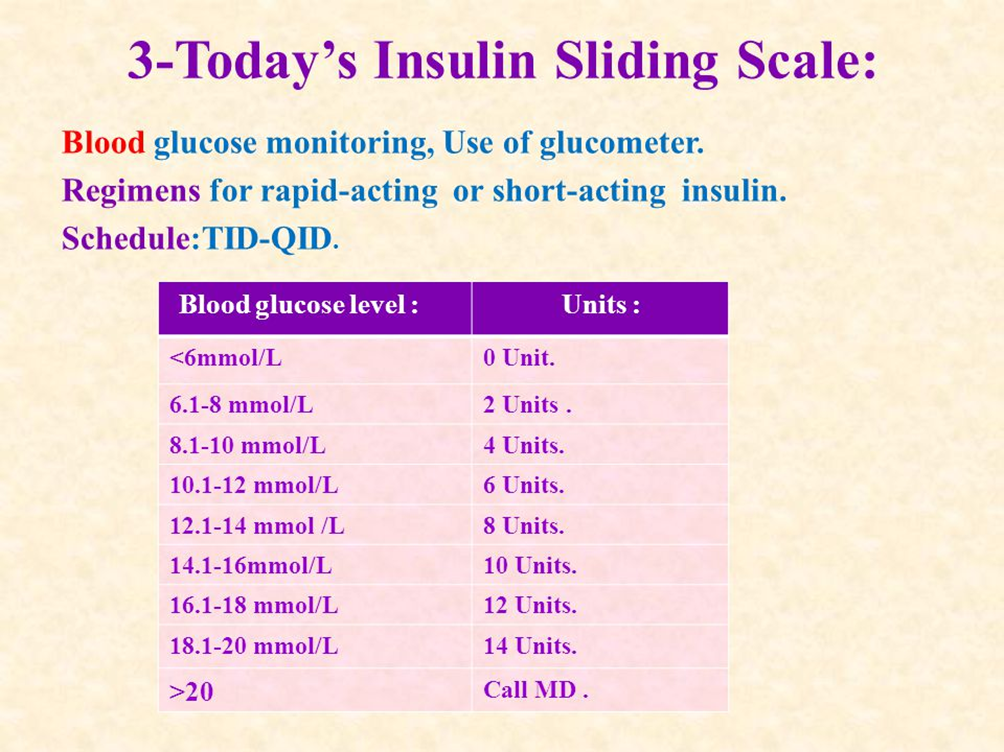
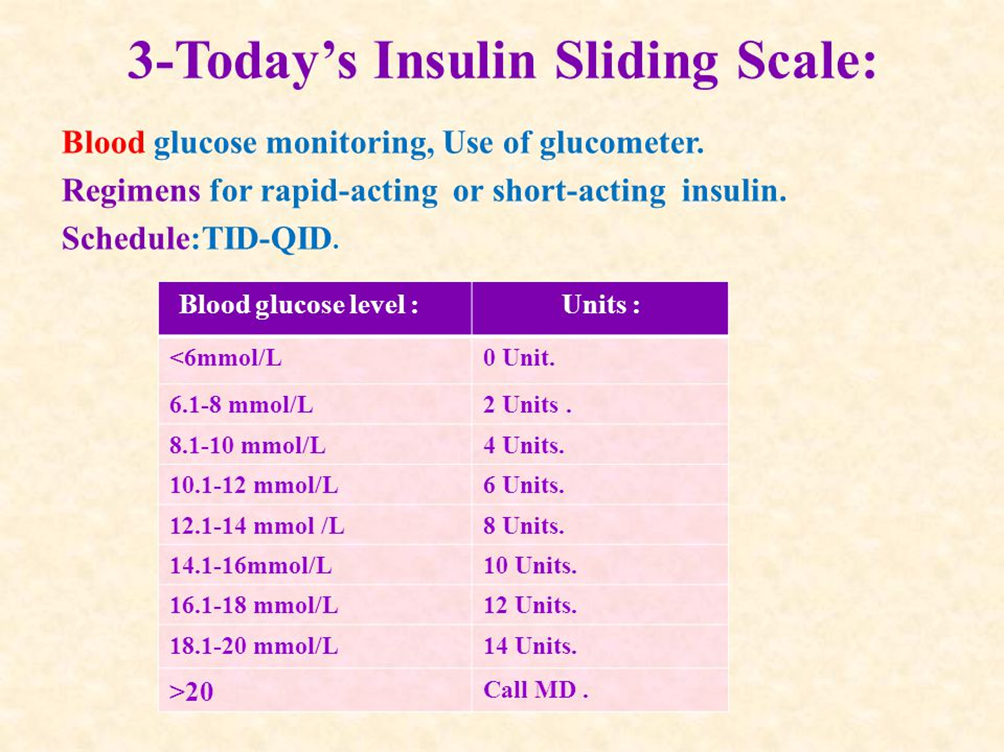
Rx of Insulin: the ‘Sliding scale’
frequently used in hospitals, rural settings
an outline of BG level results & Insulin dose based on it
in pt’s chart
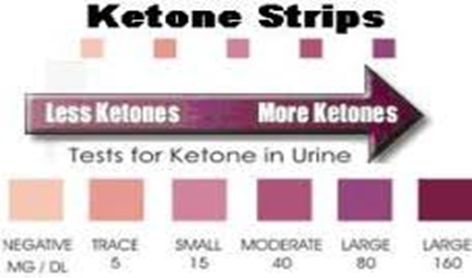
what results in high ketones
insufficient insulin-glucose transport = fatty acid breakdown into ketones for energy
if rising ketones = intervention!
high ketones seen in ketoacidosis (diabetic ketoacidosis = DKA)
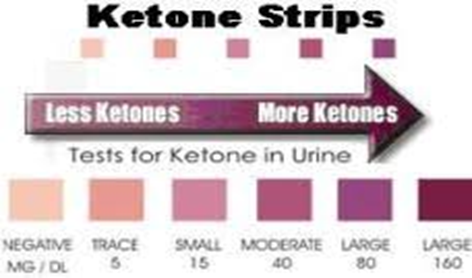
how do we monitor ketones
measured in urine
urine ketone strip
monitor levels
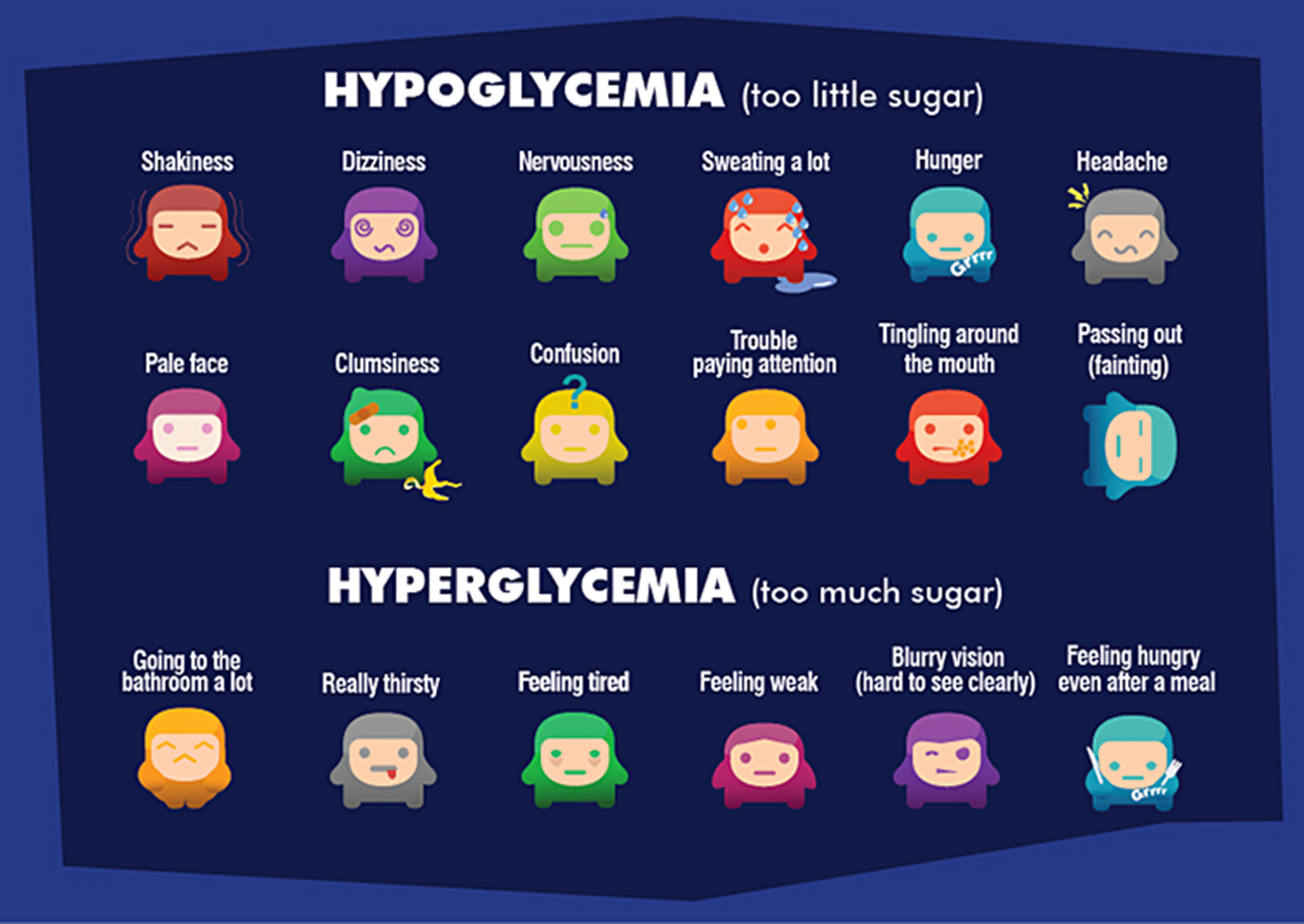
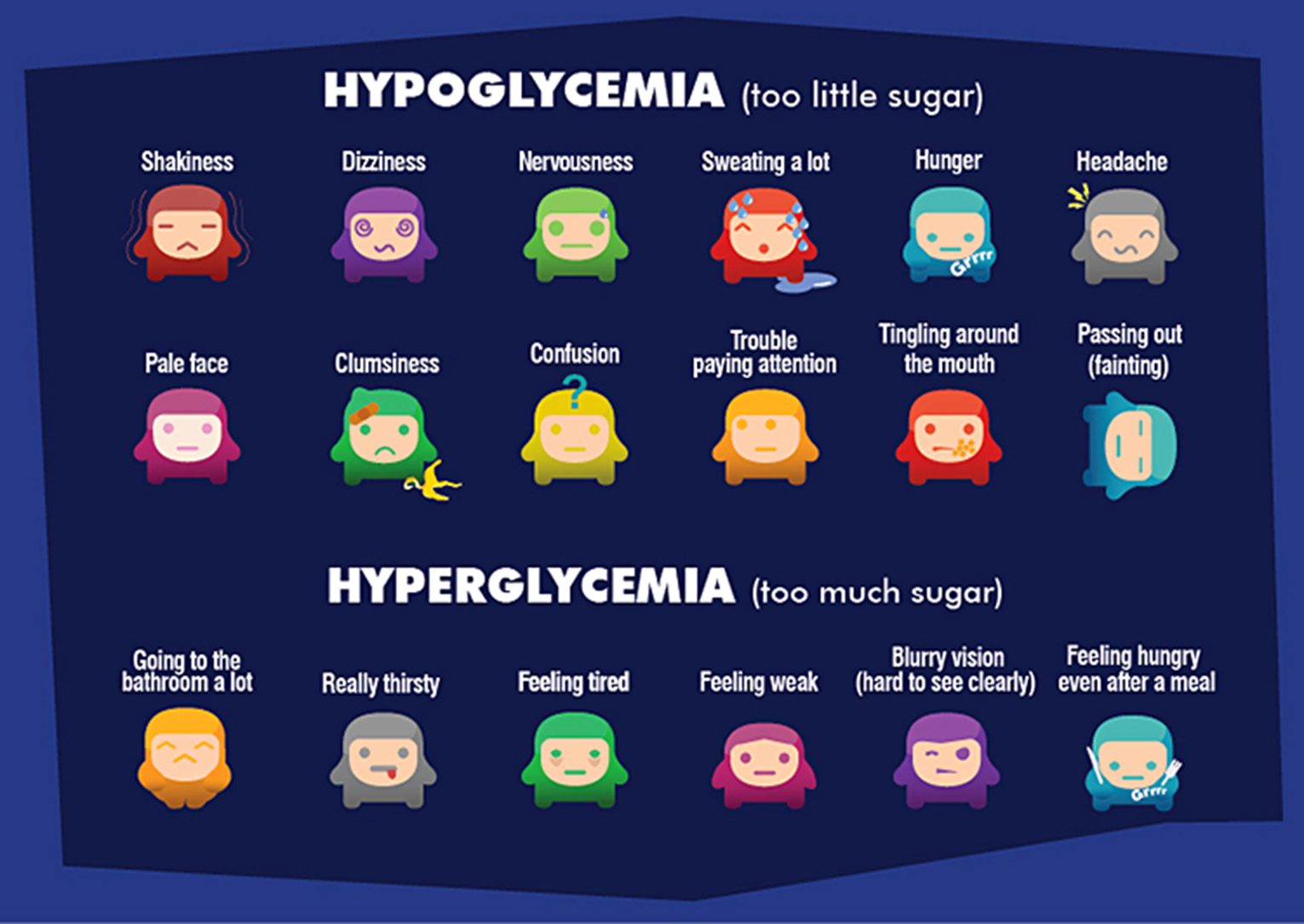
hyperglycemia onset of symptoms (most telling signs of trouble)
takes a while for S&S, dangerous longterm
thirst
fatigue
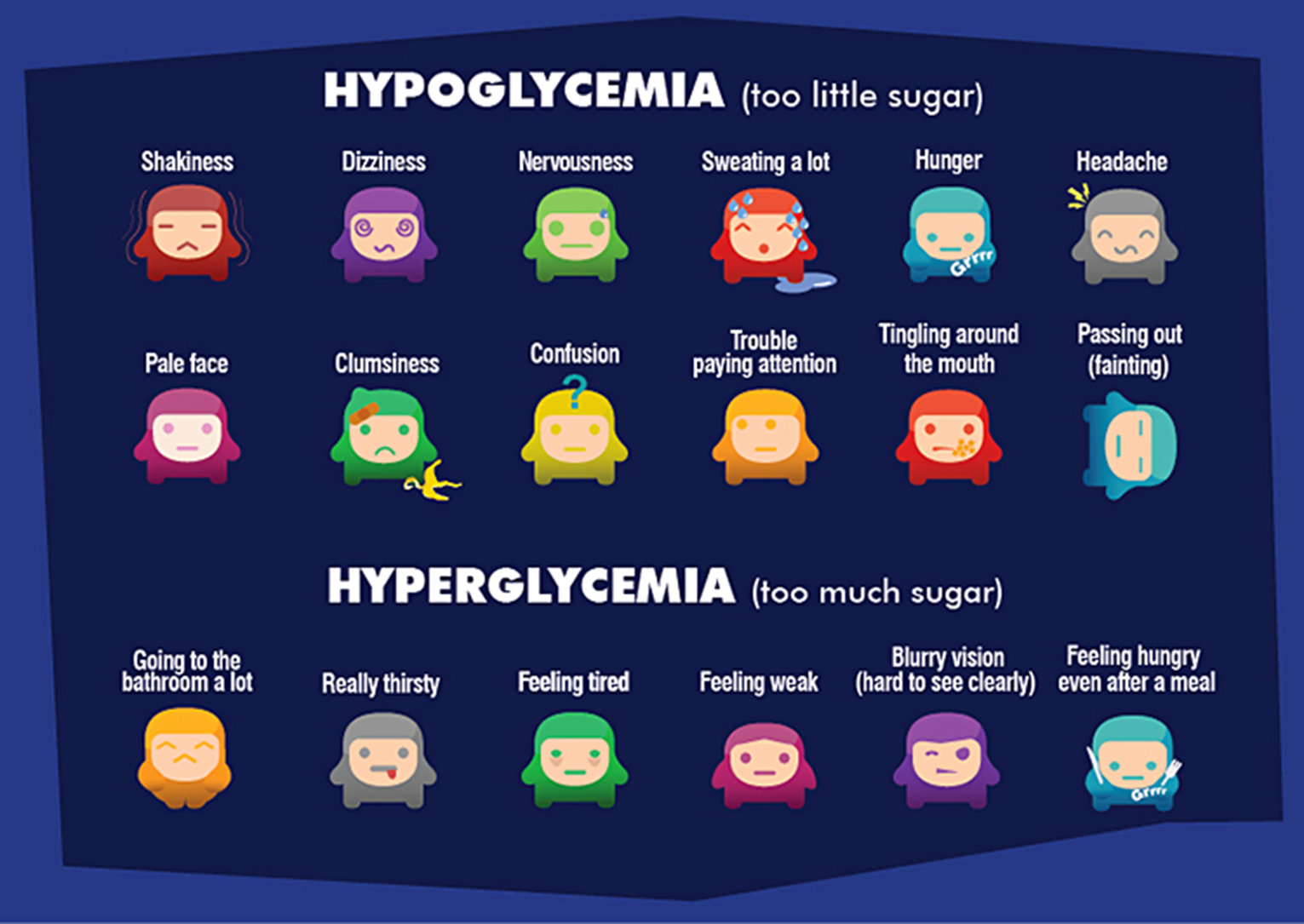
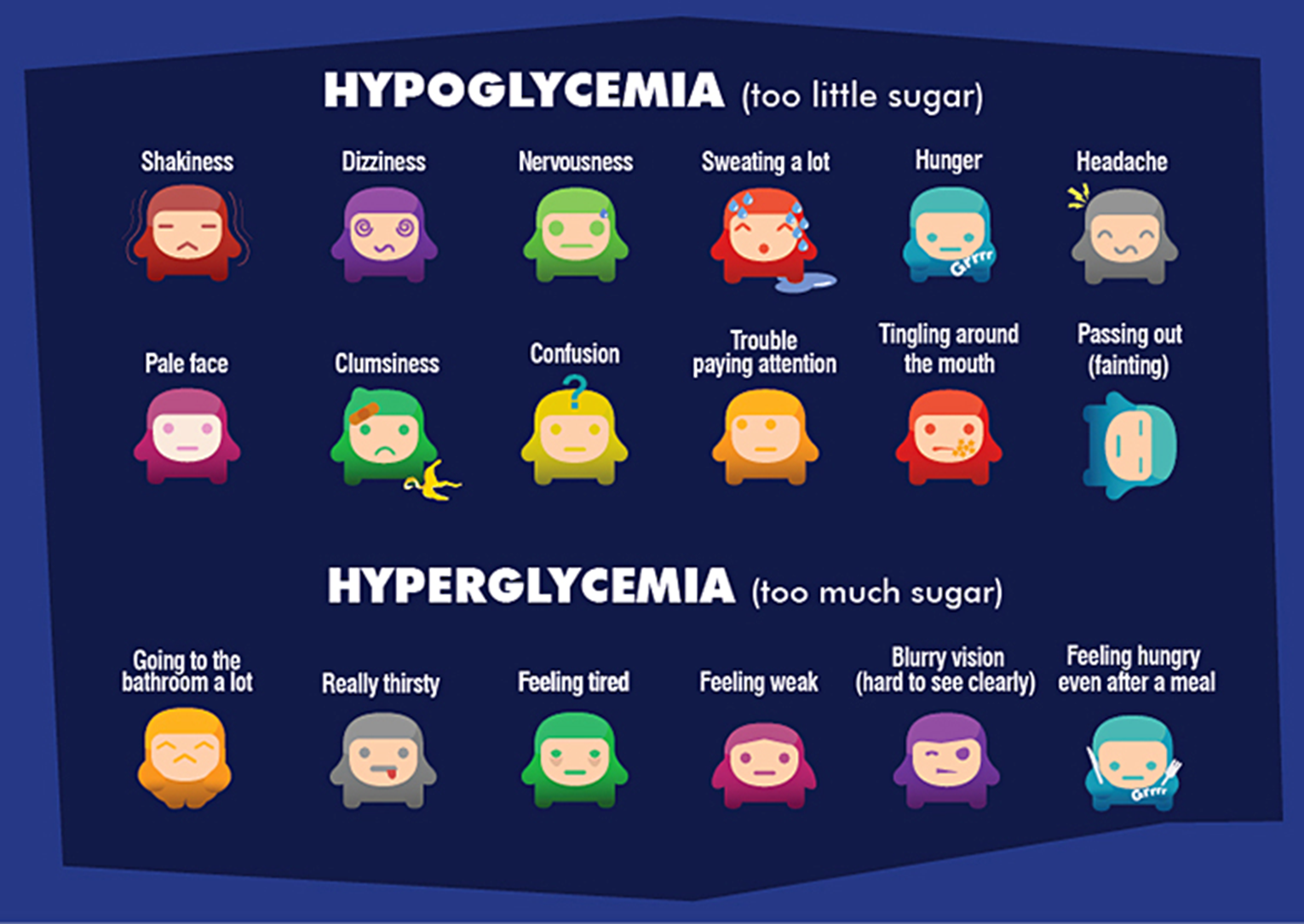
hypoglycemia onset of symptoms (most telling signs of trouble)
rapid onset of S&S
loss of focus
nervousness
shakiness
if your pt seems off= check BG level
hyperglycemia pathophysiology
high BG (high osmolality) => cellular dehydration & polyuria=overall dehydration
shift of potassium out of cells => ECF => excreted
low cellular function
metabolic shift & ketone accumulation
progression to => DKA
s&s of hyperglycemia
high BG, high urine ketones + glucose in urine, high serum lactate (metabolic acidosis),
changes in LOC, N&V, kussmaul respirations, acetone (fruity) breath
eventually hypokalemia
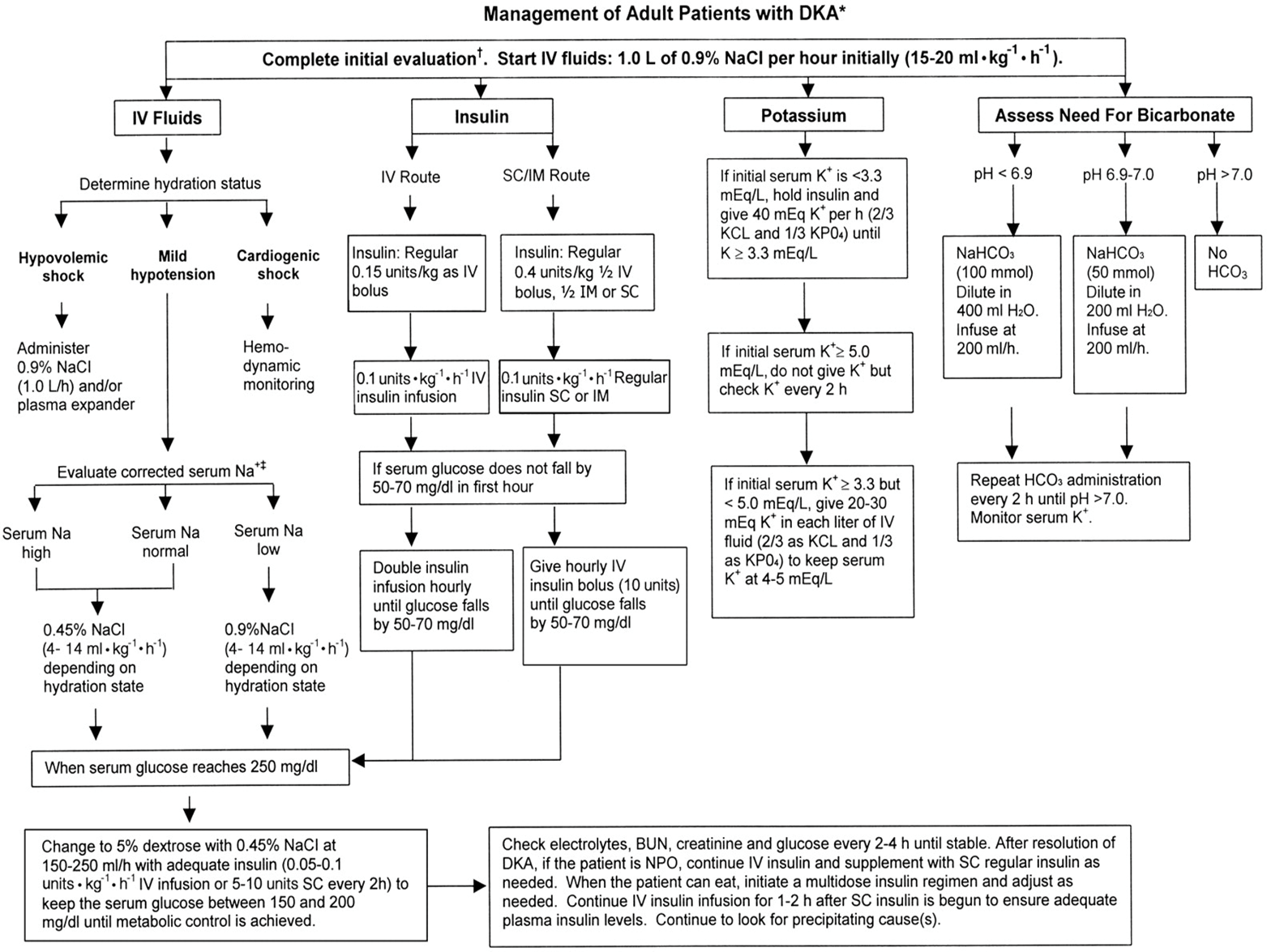
tx of hyperglycemia
regular Insulin IV, IV fluids, KCl, close monitoring ex BG q1h
neutralize metabolic acidosis=sodium bicarbonate
correction of fluids is 1st
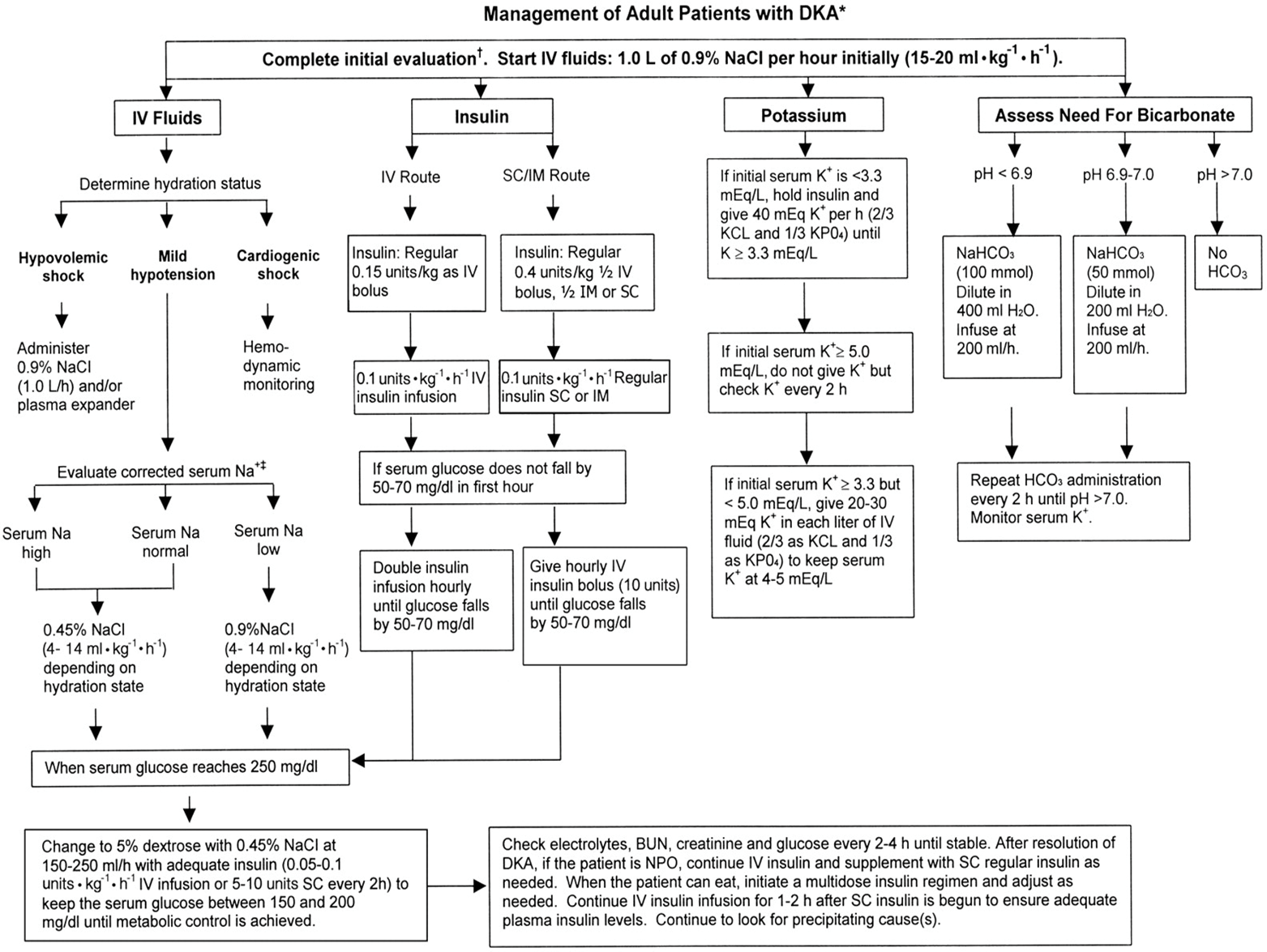
management of adults with DKS pic
using NS or RL to restore fluids back into cells, IV
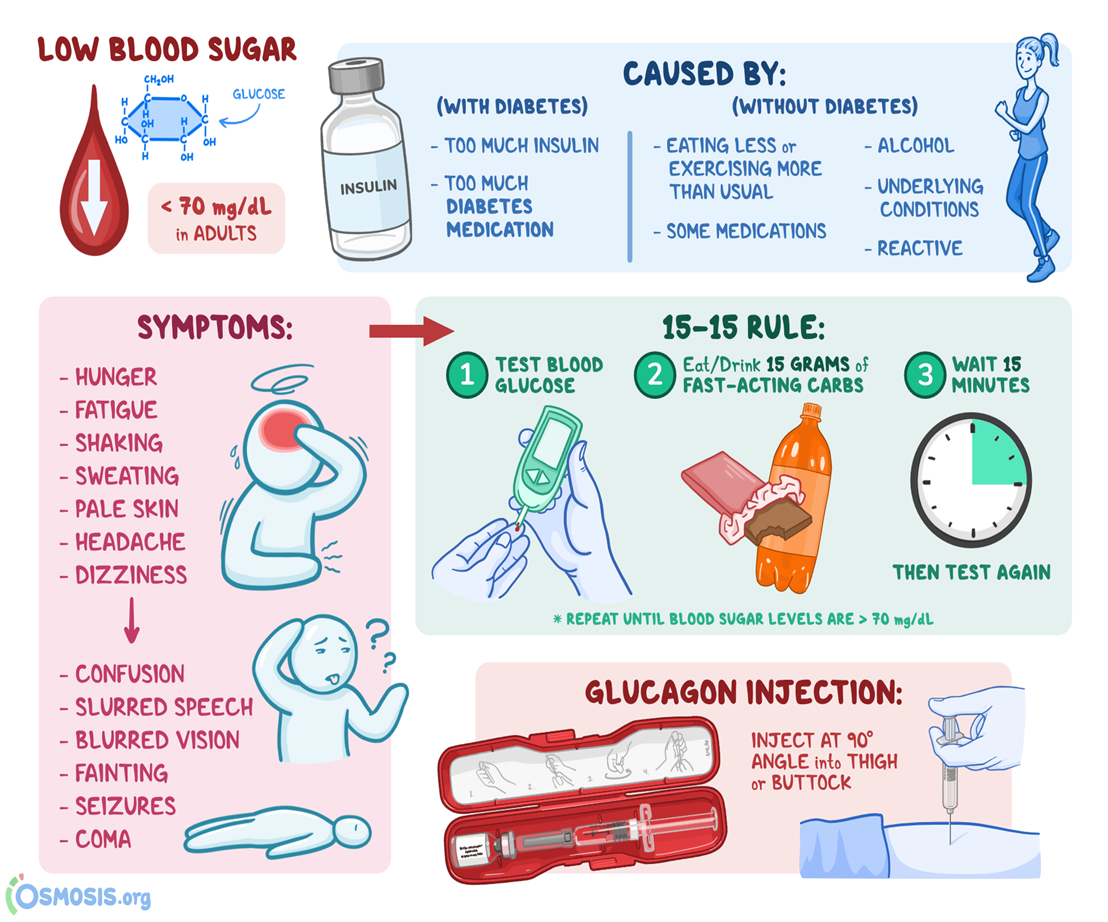
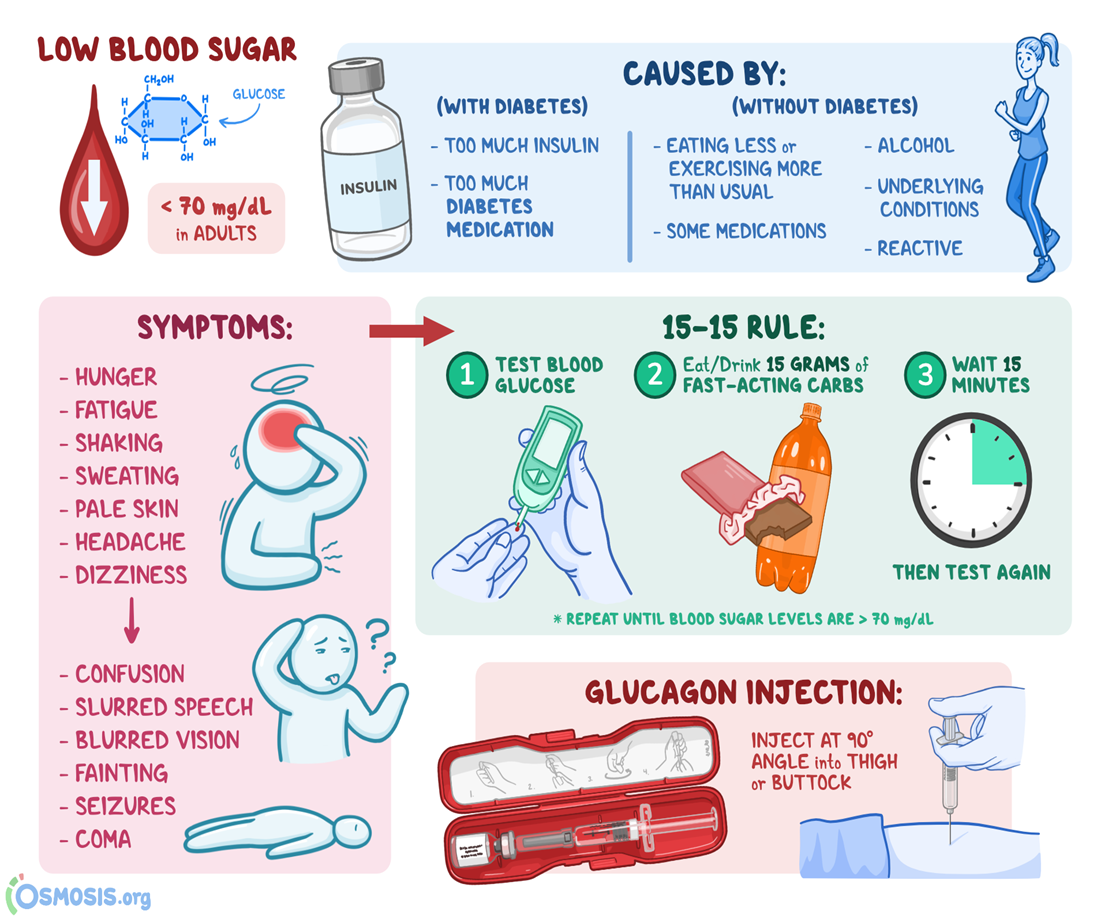
hypogylcemia causes and s&s
diet change, activity (higher than anticipated), insulin (too much)
S&S=BG <4 mmol/L
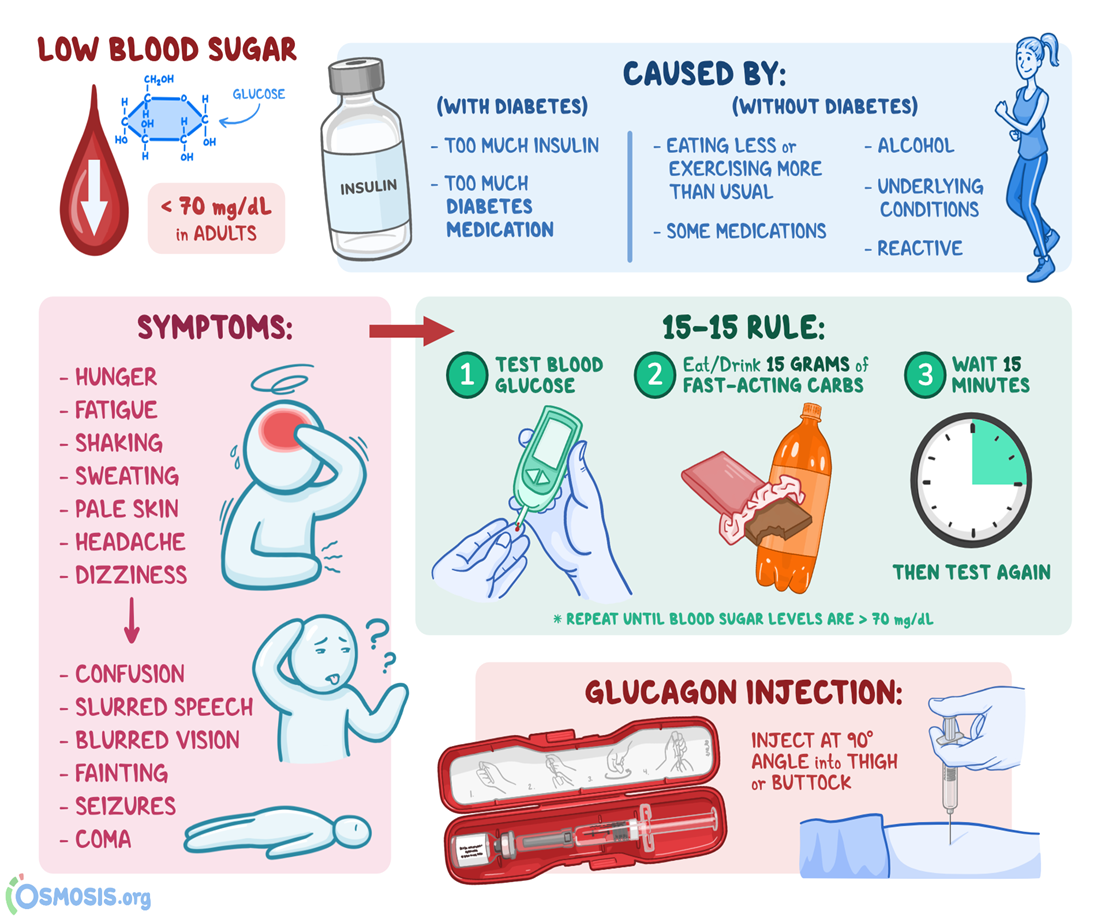
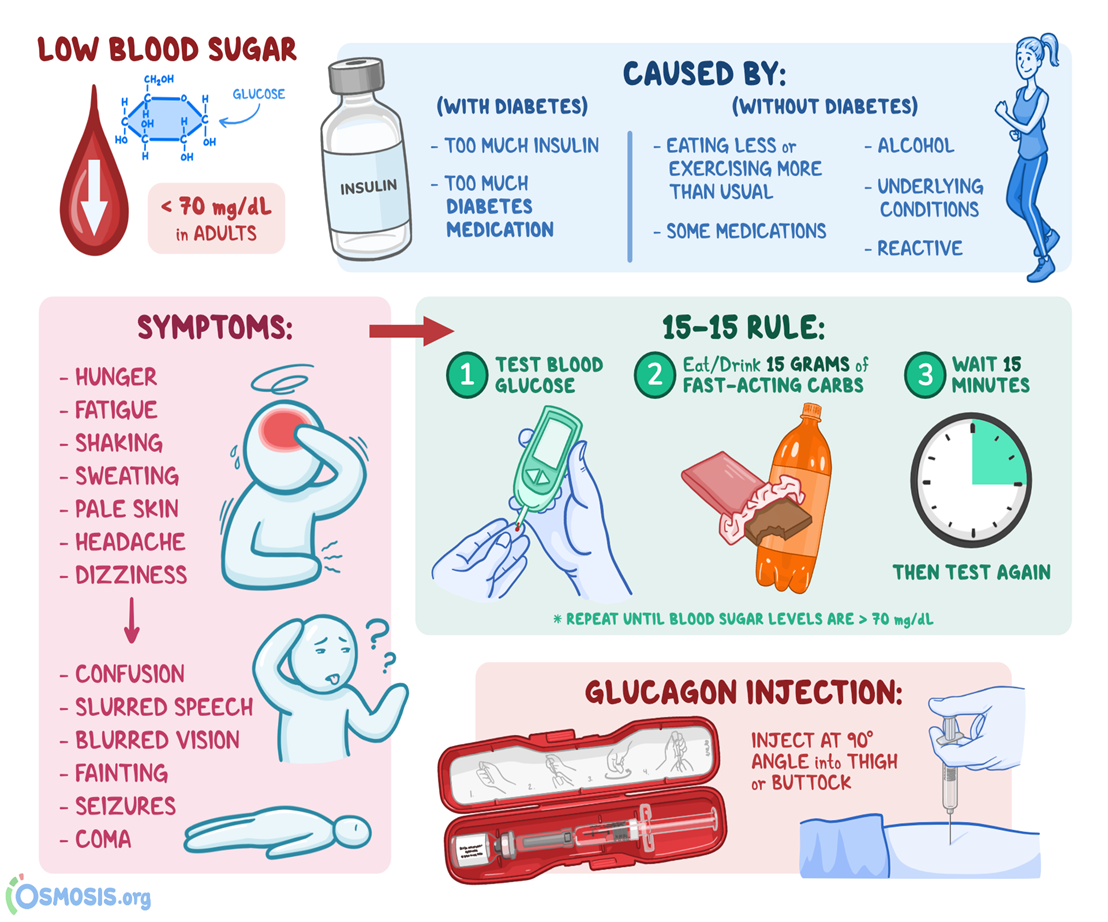
Hypoglycemia protocol: 15-15 rule (tx)
conscious or unconscious?
conscious=glucose PO; 15 g, ex glucose tablets, honey, apple juice
unconscious= glucagon IM, D50W IV
reassess q 15 min
what does BG balance influence
illness
exercise
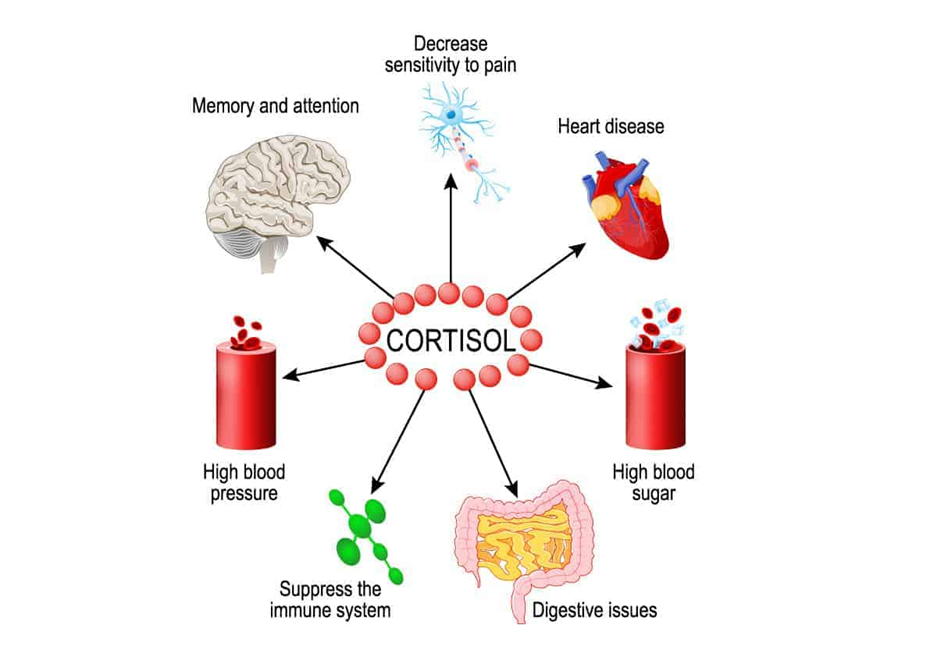
how does illness influence BG balance… require more monitoring
increased BG d/t cortisol release
increased BG d/t SNS stimulation (epi, norepi)
increased BMR => demand on resources d/t fever, processes ex inflammation, repair
decreased appetite, may include N&V
how does exercise influence BG balance… require more monitoring
decreases BG
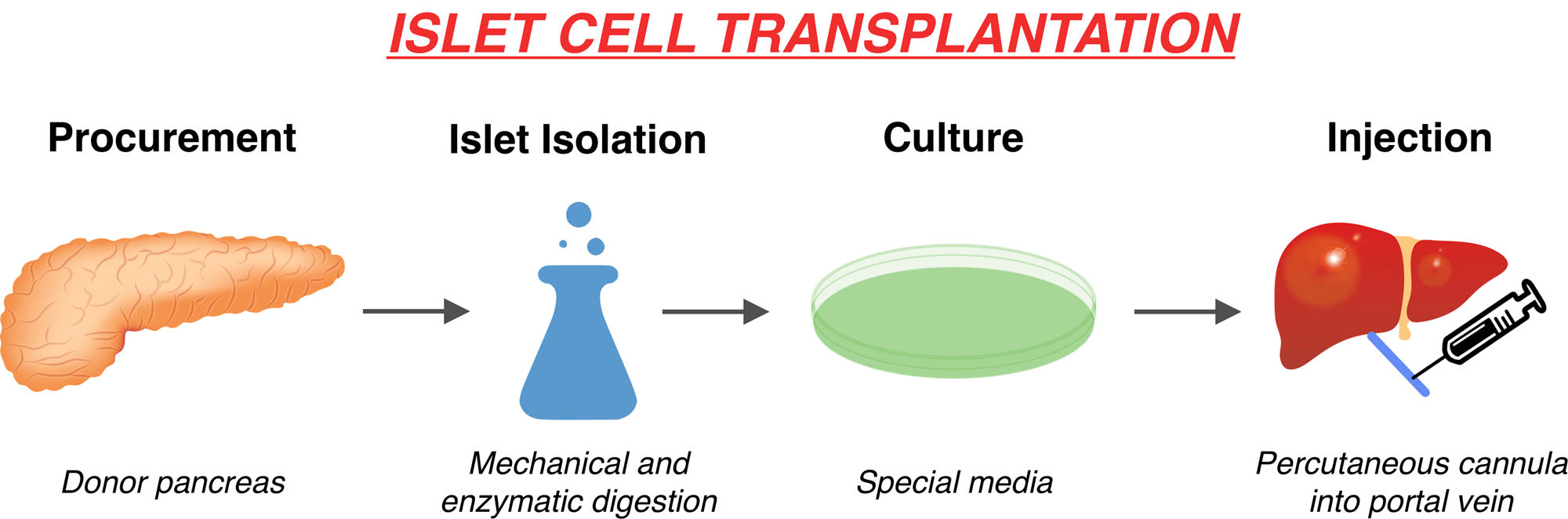
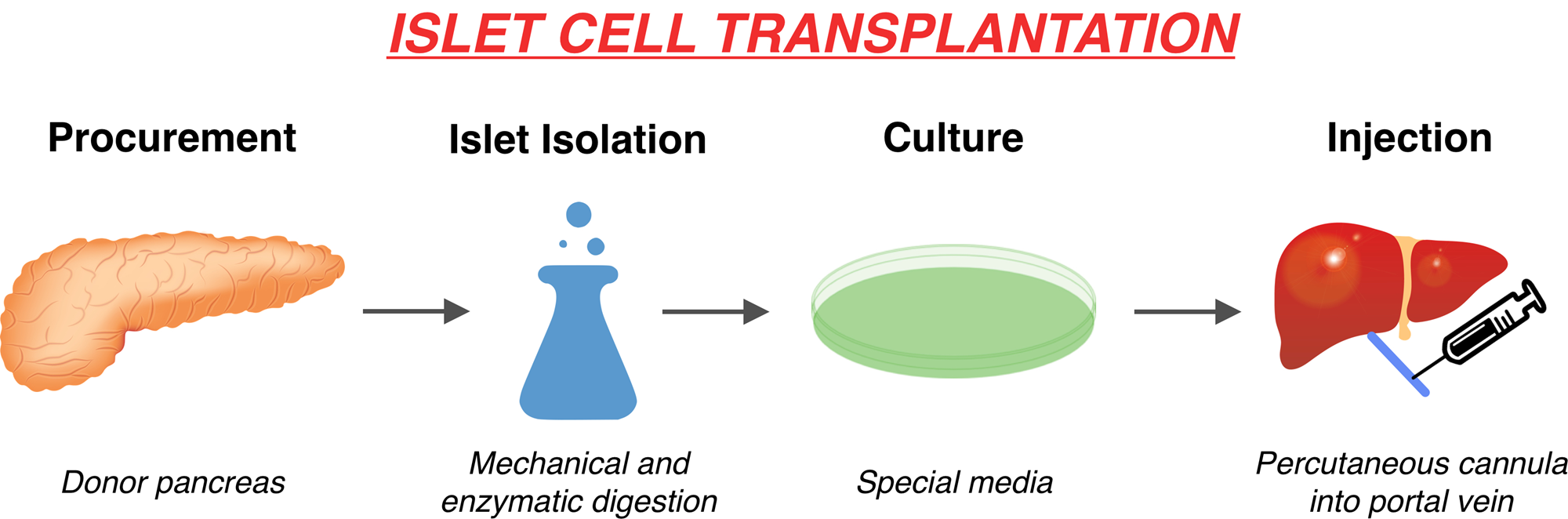
DM I other tx choices
tx=beta cell transplant + immunosuppressant drugs forever ex tacrolimus (T-cell suppression)
2-3 infusions of islet cells required (over time)
challenges=donor numbers, chronic immunosuppression
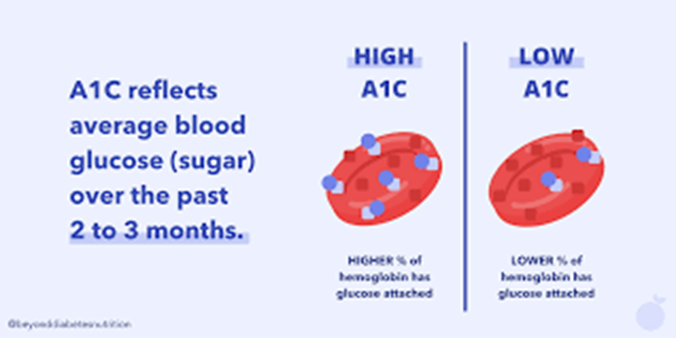
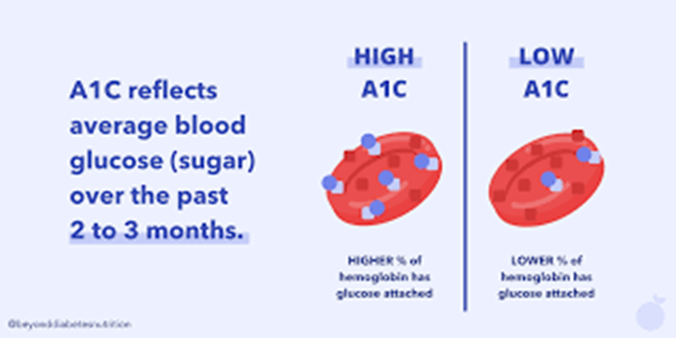
Keeping blood glucose levels even in daily life, what tests can we use
glycohemoglobin (A1c hemoglobin)
serum test of glucose bound hgb
assessment of longterm glucose control (ex over 3 months)
a tool to monitor DM pts & dx pts at risk for DM