Fundamentals of Posterior Tooth Restoration (2)
1/12
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
13 Terms
class II direct restorations
-special care must be taken when restoring the proximal surfaces of posterior teeth
-careful attention must be given to establishing proper interproximal contact and contour
-an open or irregular interproximal contact can have severe consequences including debris and food impaction, persistent gingival inflammation, bone loss, recurrent caries, and potential tooth loss
-an open contact is NOT the same as a diastema (naturally occurring space between teeth)
gingival overhang
-created when excess restorative material extends past the gingival cavosurface margin of a preparation
-restoration with gingival overhang can lead to persistent gingival inflammation, bone loss, recurrent caries, and potential tooth loss
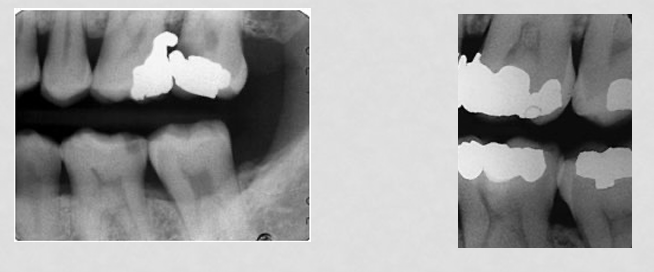
potential problem: open contact
-past challenge: producing strong contact areas on a predictable basis; conventional amalgam matrices and wedges were once used; as a result, a high percentage of restoration had flat proximal surfaces and open contact areas
-current solution: sectional matrices; have excellent reliability in achieving closed, properly contoured contacts
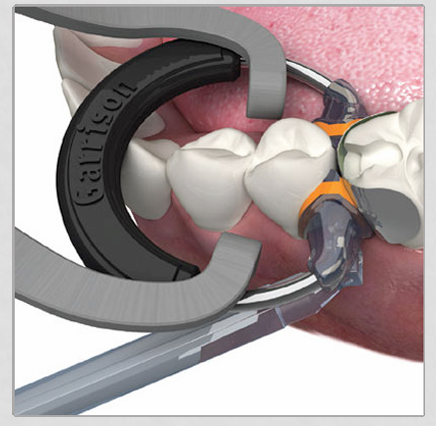
proper proximal contact and contour
-created through the use of matrix bands and wedges
-matrix bands help create proper contour and create a contact between two teeth that is closed, but able to be flossed through

wedges
-seal the gingival embrasure in order to prevent overhang

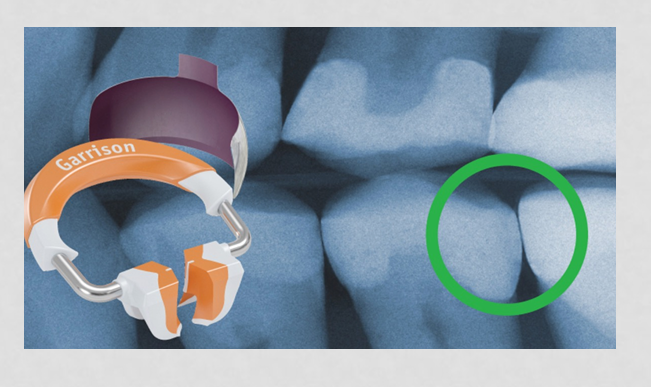
ring
-used to hold the matrix band in place, and create proper proximal contours
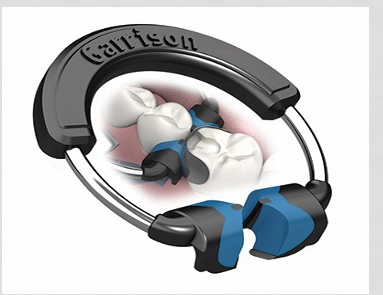
composi-tight system
potential problem: post-operative sensitivity
-past challenge: postoperative tooth sensitivity has been one of the most serious challenges in class II composites
-in the past, patients could receive simple class I or II restoration and experienced lingering, painful postoperative tooth sensitivity
potential problem: post-operative sensitivity, current solutions
1) use glass ionomer (such as Vitrebond) as a thin (approximately 0.5-mm) liner before etching and placing the dentin bonding agent; technique greatly reduced postoperative tooth sensitivity
2) place a dentin bonding agent and then a thin (approximately 0.5mm) layer of flowable resin-based composite over the bonding agent before placing the restorative resin
3) use a desensitizing agent or bonding agent with desensitizer
4) using self-etching bonding systems
potential sensitivity with composites
-without proper use of dentin bonding/sealing materials, class I and II resin-based composite restorations cause postoperative tooth sensitivity and potential pulpal death
-cause of pulpal death appears to be decreasing in incidence because more practitioners are using desensitizing liquid containing glutaraldehyde or hydroxyethyl methacrylate, resin-modified glass ionomer liners and self-etching primers instead of total-etch primers
-materials seal dentinal canals by impregnating them with resin or coagulate or physically seal dentin
-still resistance to using restorative material in posterior teeth instead of conventional amalgam because of resin-based composite’s known ability to irritate the pulp
-resin-based composite can be used without pulpal sensitivity and subsequent pulpal death when proper bonding agents, liners, and desensitizing solutions are used
use of a desensitizing agent
-gluma ingredients: 2-hydroxyethylmethacrylate (HEMA), glutardialdehyde, purified water
-works through coagulation of plasma proteins which reduces dentinal permeability and occludes peripheral dentinal tubules
-inhibits the flow of fluid through the tubules
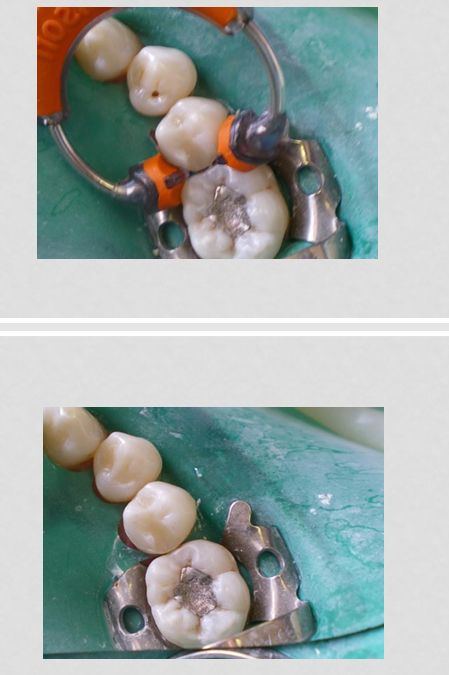
class II clinical example
-matrix band should be approximately 0.5mm higher than the marginal ridge and should be burnished to create ideal contour and contact
composite placement evaluation
-contact must be present (dental floss must snap through) and located in the correct area
-contour should replicate that of natural tooth structure
-occlusal and gingival embrasures must be present and free of overhang
-composite should be smooth and free of voids after placement
-original anatomy should be replicated including central groove, cuspal inclines, marginal ridge, and triangular fossae with proper occlusion established
-material should stay within confines of preparation and not extend beyond the cavosurface margin
-margins should be smooth and free of catches when tested with an explorer