Lecture 17: Corpus Callosum and split-brain continued
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
16 Terms
Effect of Age:
Callosotomies done in younger individuals:
disconnection syndromes seen in adult split-brain patients NOT OBSERVED
some deficits at first but they improve with time (especially when less than 13yo)
immature brain has potential for adaptation (PLASTICITY)
some problems persist like pragmatic language deficits.
Development of commissural fibres
Anterior Commissure develops at 10th week
CC develops at week 12 until 6th or 7th month. Rostro-caudal development, myelinisation continues after birth. earlier problem occurs, more agenesis
Agenesis of CC
defect before week 10: no AC and no CC
between week 10 and 12: no CC
between week 12 and 20: partial agenesis of CC
What happens when born without a CC?
sometimes nothing! disconnection syndrome not observed, normal IQ in 2/3 of cases. different outcomes when isolated vs associated with other malformations.
Some deficits with agenesis:
motor coordination, emotional, social, pragmatic language
possible adaptation mechanism: bilateral language functions (each hemisphere is able), but! amytal sodium studies say this is not the case (not all brains are the same).
residual commissures + sub-cortical commissures
compensation, especially to transfer visual info
ipsilateral tactile information: normally eliminated in normal development, each hemisphere has a bilateral representation.
Kim Peek:
agenesis of CC and other abnormalities, autism (unsure, but he had autistic traits that could’ve been due to abnormalities), low IQ, incredible memories, able to read left and right page simultaneously.
Agenesis of CC and autism:
motor, language, emotional and social deficits are similar to characteristics of individuals on the autistic spectrum
in autism: major characteristic is volumetric and microstructure reductions in CC.
between 10 and 30% of agenesis cases also have an autism spectrum diagnosis or marked autistic traits
anatomical connectivity and autism:
some evidence shows that autism is caused by disconnections… white matter differences (esp. frontal, temporal and parietal)
link between white matter alterations and function?
processing speed of the brain, motor deficits, sensori-motor integration
autistics have reduced CC but there is no deficit that is 100% associated with that. does it affect the brain or behaviour? no clear evidence
corpus callosum in autism: reductions in volume, microstructural alterations (seen in diffusion imaging), SUGGESTS ALTERED INTERHEMISPHERIC COMMUNICATION
Study objectives:
relate CC structure (MRI) with function and interhemispheric transfer
measured interhemispheric transfer time via visuo-motor task (Poffenberger)
measure bimanual coordination (Purdue pegboard task)
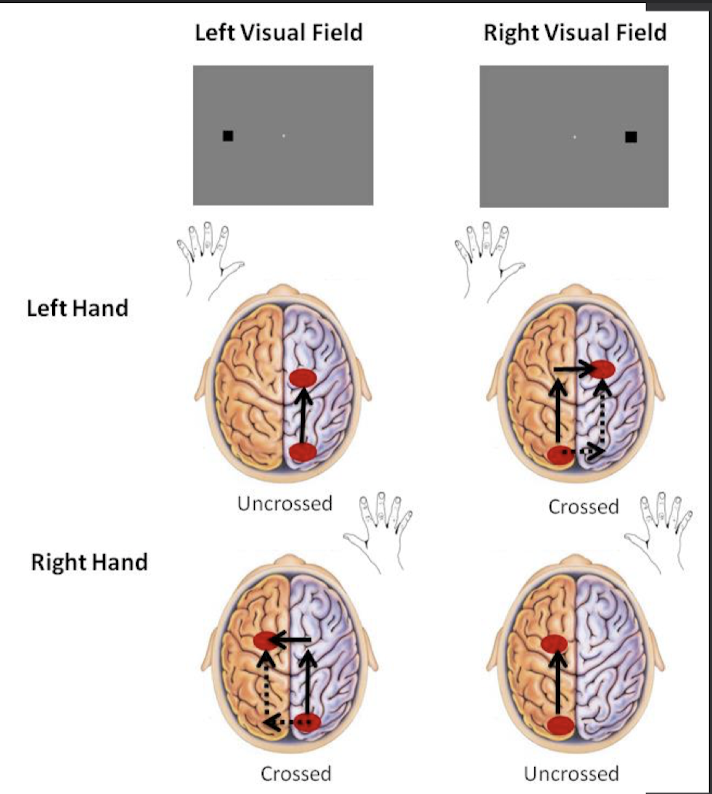
Poffenberger paradigm
used to measure interhemispheric transfer time (IHTT)
where does the transfer occur in the CC?
at visual level via splenium of CC
at motor level
do trials with both hands and both visual fields (cross vs uncrossed trials) enough times, compare cross vs uncrossed to get the IHTT.
manipulate motor and visual aspects in turn and see which affects the transfer tine
localized CC lesions
Transfer is faster at the motor level
CC structure results:
results: TYP > AUT frontal and parietal
motor frontal areas and posterior parietal areas of the CC were reduced.
Behavioural results of Poffenberger:
no difference in terms of interhemispheric communication:
IHTT and bimanual coordination showed no reduction in transfer time.
Structure- function relationship
correlations between between behavioural measures and CC:
IHTT and bimanual coordination associated with different parts of the CC in each group
faster performance times related to bigger or better CC in subsections of motor and parietal areas in typical. motor CC is involved in transfer times in typical individuals. in autistics: related to larger splenium of the CC. some type of reorganization that despite reduction in overall size of the CC, autistics rely more on visual transfers.
Conclusion of IHTT and bimanual:
despite structural reductions in the CC:
intact information transfer (seen with no behavioural differences in typical vs autistics
transfer at the visual level rather than at the motor level (bigger splenium vs smaller posterior middy and rostral body
shows consistency with literature: AUT have more occipital activations
modified structure-function relationship associated with equal performance (reallocation) using different neuronal trajectories
Motor deficits:
AUT are slower for unimanual conditions:
reaction times: execution speed, anticipation, preparation of movement
EX: Purdue pegboard test, slower at clicking button in general, not necessarily related to CC but more due to intrahemispheric communication
Intra-hemispheric connectivity:
deficits in: using spatial representation and integration of visual info essential to plan and execute movements
white matter abnormalities at intrahemispheric levels; motor deficits not due to CC bc IHTT has no deficits. due to when you have to use visual info to guide motor actions
role of the parietal lobe: visuomotor integration, directed actions, imitation, plan and control of action.
agrees with: reduced intrahemispheric connectivity between frontal and parietal areas in autism
atypical visual input and integration during motor action have been related with atypical connectivity between parietal and motor areas.