PCl218 final exam
1/175
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
176 Terms
Why must we learn about pharmacology when discussing Cannabis>
Important for grasping how cannabis interacts with the human body.
What is Homeostasis
The body’s ability to maintain internal stability in response to external conditions (ex. cannabis, stress, temperature)
What is Pharmacodynamics
What the drug does to the body, interactions between compounds (drugs) and receptors.
What is Pharmacokinetics
What the body does to the drug
What is the Lock and Key model of Pharmacodynamics?
Drug = key
Receptor = Lock
Binding the two causes a physiological response.
What are some examples of pharmacokinetics?
Absorption, distribution, metabolism and elimination
What are the 4 types of drug receptor interactions?
Natural agonist, natural product agonist, Synthetic agonist, antagonist
What does an Agonist do?
Activate receptors
What does an antagonist do?
Bind to receptors but they do not activate, thus preventing other compounds from binding
What is the difference between natural/endogenous, natural product/phytochemical and synthetic agonists?
The first is body produced, the second is from plants and the third is from a lab
What is adrenaline/epinephrine an example of?
A natural (endogenous) agonist released in fight or flight
What is ephedrine, a plant derived mimic of adrenaline an example of?
A natural product (phytochemical) agonist
What is Ventolin, an pharmaceutical mimic of adrenaline an example of?
A synthetic agonist
In the adrenaline system, what is propranolol, a substance used to treat high blood pressure from labs?
An antagonist
Describe the Opioid system in terms of agonists and antagonists?
Endorphins = natural agonists (natural opioids)
Morphine and heroin = natural plant agonists
Fentanyl: Synthetic agonists
Naloxone (to reverse overdoses): Antagonist
What is Tolerance?
The body reduces receptor availability to maintain balance (homeostasis) which means that more drug is needed for the same effect
What is Dependence?
Continued use of external compounds, replacing natural functions
What is Withdrawal?
When drug use stops, the downregulated natural system can't immediately compensate, causing symptoms.
T/F: Potency is how strongly drugs activate receptors
True
Rank these routes of drug administration from fastest (and highest risk of addiction) to lowest
Injection, inhalation, oral (edibles) and topical
How are drugs metabolized?
Most are through the liver by enzymes and excreted via kidneys, lungs or breast milk. If not done so properly, these compounds can add up, becoming toxic.
Explain risk to benefit ratio
Every drug use has some risks and benefits, they must be weighed.
For instance, fentanyl for end of life care has benefits of pain relief that may outweigh any cons.
Does natural mean safe?
No! Many dangerous drugs come from plants, like cocaine. They must be evaluated like lab made drugs - by mechanism, dose and effect.
What are the purposes of clinical trials?
To assess efficacy (if it works or not) and safety (is it harmful) of new drugs. They validate scientific claims and are required for regulatory approval ex. Health Canada
What are the phases of drug development?
Basic research (studying compounds in cell models or tissues)
Preclinical testing (toxicity scan, animal testing)
Clinical trials (testing in humans, takes 6-12 years and costs millions)
Approval (does benefits > risk)
Post market monitoring (tracking long term safety issues that might emerge later)
T/F When a drug is approved, it is approved for general use
False. It is only approved for a specific condition ex. pain. You may still use it but it lacks the same evidence. Approval considers:
Severity of illness (risk benefit ratio)
Existing treatments
Vulnerable populations
What are the phases of clinical trials?
Healthy volunteers
This assess safety, dosing and how the drug and body interact with each other. It can detect red flags earlier like toxicity.
Small group with illness
Tests if it works and any side effects, justifying a larger experiment.
Large, diverse group
Confirm if it works and compare with the standard.
Post market
Monitor long term effects past the 6-12 years
T/F Dosing decisions are precisely studied, relying on pharmacokinetics and effectiveness
True
What challenges do clinical trials for Cannabis face?
High cost and lots of regulations
Product is already used and many self-medicate
Some products have dosage and formulation inconsistency which makes it hard to study them
T/F Historically, negative trials were not reported/underreported and this skewed the perception of drug effectiveness
True, they may be biased to do so. However, WHO guidelines say clinical trials must be registered and published now, and in Canada CIHR requires trial results to be made public within 12 months of study completion.
As well, the media attention favours positive results.
T/F Randomized controlled trials are the gold standard for clinical testing
True
What is a randomized control trial?
Participants are randomly assigned to new drug, placebo or standard treatment. It is double blind so neither side knows the groups, avoiding bias.
What is a placebo?
An inactive substance that still produces perceived benefits. This arises from expectations, emotions, trust and context.
What is the Nocebo effect?
Negative outcomes from expecting harm, driven by anxiety, mistrust, prior experiences or social influence.
It may shape perception of side effects.
Why is placebo relevant to cannabis?
Significant in cannabis trials, especially for pain due to media hype.
What does endogenous mean?
Coming from within the body
T/F All compounds are produced by the body in response to stimuli (ex. stress or fear), acting on receptors via lock-and-key mechanism
False, only endogenous/natural agonists do that.
What is the endocannabinoid system? (ECS)
A regulatory system present from early development and existing in all people (including non-cannabis users).
Explains how THC works and has a role in tuning many cognitive and physiological processes
What is an endocannabinoid?
A part of ECS that is an natural agonist (ex. anandamide and 2-AG)
What are enymzes in ECS?
They break down and synethesize endocannabinoids (ex. FAAH)
What are the receptors in ECS?
CB1 (mostly brain) and CB2 (mostly immune system)
T/F Transporters are part of the ECS but not covered in the course
True
Where are CB1 receptors?
Widespread - brain, liver, lungs, skin, kidney, heart
Where are CB2 receptors?
Immune system
In the brain, what is CB1 involved in?
Cortex (cognition, attention)
Hippocampus (memory)
Hypothalamus (appetite, metabolism)
Amygdala (mood, emotion)
Brainstem/spinal cord (pain, vomiting)
How do encocannabinoids act to release neurotransmitters?
They act locally at synapses
T/F: Activation of CB1 receptors can reduce GABA, which increases dopamine.
True, but this is not the only function, CB1 receptors are on many different types of neurons.
When are endocannabinoids produced?
To relieve Stress or Pain
Different times of day to regulate sleep and appetite (encourage hunger)
Exercise (improving mood)
T/F the ECS can help manage pain and stress, with some evidence pointing to helping with memory and regulating distressing ones.
True
T/F ECS increases before meals and an overactive one promotes weight gain
True
Given that an overactive ECS contributes to obesity, Rimonabant (CB1 antagonist) was studied as an aid. Why is it withdrawn after post-market surveillance.
Side effects of depression and suicidal thoughts. ECS is too integrated to just block globally.
If there was acute stress or pain, what would ECS do?
Increase to protect and relieve
If there was chronic stress, obesity or disease, what would ECS do?
ECS may become dysregulated or overactive
T/F the ECS can only be modulated through pharmaceuticals
False, lifestyle changes like exercise and genetic differences (FAAH gene) also have a role.
What are the two main ECS enzymes?
FAAH: breaks down anandamide (an endocannabinoid)
MAGL: breaks down 2-AG. (also one)
What would FAAH inhibitors do?
Blocking FAAH → more anandamide available → prolonged ECS activation.
There are potentially anti-stress and anxiety effects (like social anxiety)
What is FAAH polymorphism?
Some people have a different FAAH gene (38% of Europeans) that results in reduced FAAH activity → more anadamide
This leads to things like lower stress/anxiety, less pain senstitivity, increased reward sensitivity, impaired short-term memory and better PTSD treatment.
The case study of a “pain free” Scottish woman showed this, although she had 2 of these mutations. This offered insights on new pain medications.
What are the major milestones of cannabis?
Cannabis use dates back to ancient history, but research began in 1800s.
From 1960-90, there was the discovery of cannabinoid structures, as well as receptors (CB1 and CB2)
From 90s to 2000s, endocannabinoids (ex. anandamide) were discovered as well as the FAAh enzyme.
T/F: THC and CBD are Phytocannabinoids (natural plant agonist)
True
T/F: anandamide and 2-AG are endogenous (natural agonist)
True
T/F Some synthetic cannabinoids are agonists and some are antagonists, but they are always lab made
True
What receptor does THC work with and what does it do?
THC activates the CB1 receptor, affecting brain and body functions by mimicing endocannaboids but it is non-selective.
This mean it floods the whole system instead of just operating where needed.
What are some acute effects of THC
Euphoria, increased appetite, pain relief, possible anxiety/paranoia
What is a chronic effect of THC
Can cause tolerance (downregulation of CB1) → requires more THC for same effect
How are endocannaboids and THC different?
Endocannaboids: Triggered by environmental cues (right place, right time) and are rapidly inactivated when not needed
THC: Triggered by intake and comes all at once, very variable and hard to predict.
What does the desensitization of CB1 receptors do (caused by repeated THC use)
Reduced ECS response → lower dopamine → Functional brain changes (ex. learning, memory, motivation)
T/F Once CB1 density drops with chronic use, it cannot be recovered
No, scans show otherwise
What is Cannabis Use Disorder (CUD)
A condition characterized by an individual's inability to stop using cannabis despite negative consequences, leading to significant impairment in personal, social, and occupational functioning.
Around 10% of users develop CUD, higher risk is associated with
Early use, heavy/frequent use, high THC potency products
Symptoms of CUD?
Tolerance, withdrawal, difficulty cutting down, disruption of daily function
Those with the different FAAH gene may feel less pain and stress, but be more or less at risk for CUD?
More at risk
Why is the existence of pharmacokinetics important
It prevents harmful accumulation of compounds like drugs
What is the role of the liver in pharmacokinetics?
Metabolism, by containing cytochrome P450 enzymes (CYPs). These enzymes chemically modify substances (like THC) to make them more water soluble.
Then, they can be excreted through lungs (ex. alcohol via breath), urine (via kidneys) and breast milk.
What is a metabolite?
Substance formed when the body breaks down (metabolizes) a drug or compound.
They are usually found in the liver and can be active or inactive.
What psychoactive (but not the strongest) metabolite is produced when THC is first inhaled/ingested?
Delta-9-THC, produces a high
What psychoactive metabolite is produced after liver conversion and produces a stronger high
11-Hydroxy-THC, produces a stronger high
What inactive metabolite is produced after the furthest metabolism
Carboxy-THC, inactive ansd used in urine testing
___ THC has a faster onset and lower 11-Hydroxy-THC (strong high) and has a shorter effect than ____
Inhaled, ingested
T/F it is harder to judge dose of ingested edibles
True, because onset takes much longer and peak effects are after 4 hours.
The duration is also up to 12 hours, and more potent metabolite (11-hydroxy-THC) can build up!
The delayed onset can lead users to take more, but recommend is to wait at least 4 hours before doing that.
T/F THC blood concentration correlates reliably with how impaired someone is (in the care of impaired driving)
False, some users may be newer or more experienced with the drug, so they may take the same dose (same THC level) but have differing impairment.
THC impairment also last longer than blood levels suggest. THC thresholds exist for driving but are controversial.
Describe genetic variation in THC metabolism
The enzyme CYP2C9 is responsible for converting THC to inactive carboxy-THC. Some people have variant alleles, meaning they have a slower metabolism.
This leads to THC staying in body longer → more effects.
What variables may make cannabis response different case-by-case?
Dose/frequency → affects intensity and duration
Rouse of use (inhaled or ingested)
Sex, age, genetics (influences metabolism, tolerance and sensitivity)
Tolerance due to use (less CB1 receptors)
T/F THC is lipid soluable, meaning it is stored in fat tissue
True, this results in a slow release and extended effects
How does THC (or CBD) affect prescription drugs?
They inhibit some enzymes, raising the blood levels of other drugs.
This causes more effects and also misinterpreted therapeutic effects (from increased concentration of the other drug)
Why is it important to inform doctors of cannabis use?
They can affect other drugs, making them more potent through inhibiting some enzymes.
Why are natural products like cannabis more uncertain in dosing and safety, compared to prescription drugs?
There is less testing on how much is safe/effect as well as how fast the drug is metabolized and eliminated.
T/F Grapefruit juice can also inhibit CYP enzymes like THC/CBD
True!
What is a meta analysis?
Statistical analysis of results from multiple studies.
What is a systematic review?
A comprehensive structured literature review using predefined methods
T/F Meta-analyses are at the same level on the evidence pyramid as individual randomized control trials
False, they are at the top
What is the point of meta analyses and systematic reviews?
Summarize results on a specific clinical question
Minimize bias and determine whether evidence is trustworthy
What is the difference between narrative reviews and systematic reviews?
Narrative reviews are a summary based on author opinion.
Systematic reviews are an exhaustive search with defined methods, it is also reproducible.
What is the difference between meta-analysis and systematic review?
All meta-analyses involve a systematic review, but not all systematic reviews involve a meta-analysis.
Meta-analysis = systematic review (qualitative and empirical) + quantitative analysis of data
T/F: Should a 53-year-old woman with HIV-related polyneuropathy and moderate-severe pain use cannabis for pain relief, compared to traditional options? is an example of a clinical question
True.
Patient: 53-year-old woman with HIV-related polyneuropathy
Intervention: cannabis for pain
Comparator: standard medications
Outcome: pain relief
What are the steps of a systematic review?
Define a focused question using PICO (Patient, intervention, comparator, outcome)
Conduct an exhaustive literature search
Use MeSH terms (Medical Subject Headings)
Use boolean logic to optimize database searches
Apply criteria such as RCTs only, treatment > 1 month
Extract data from the papers and assess risk of bias
Analyze data
Summarize narratively or proceed to meta analysis
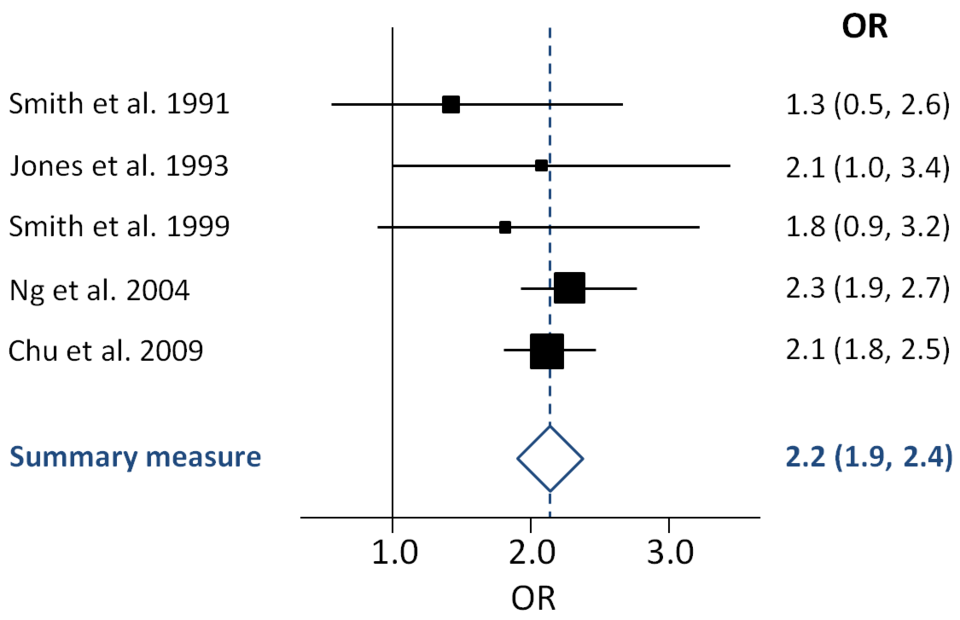
What is a forest plot?
Each study = one line on the plot with a square (effect size) and horizontal bar (95% CI/confidence interval).
Diamond at the bottom = pooled result of all studies.
Diamond crossing "no effect" line → not statistically significant.
I^2 < 50% = low heterogeneity; I^2 > 75% = high heterogeneity (less confidence in pooled result).
What are the steps of a meta analysis
Define a focused question using PICO (Patient, intervention, comparator, outcome)
Determine research protocol
Conduct an exhaustive literature search
Use MeSH terms (Medical Subject Headings)
Use boolean logic to optimize database searches
Apply inclusion/exclusion criteria such as RCTs only, treatment > 1 month
Extract data from the papers
Assess risk of bias
Analyze data
Summarize narratively or proceed to meta analysis
What does Risk Difference (RD) mean?
Risk in treatment minus risk in control.
If it is positive, outcome is more likely with treatment
What does Number Needed to Treat (NNT) mean?
NNT = 1/risk difference (for good event)
Lower = better efficacy
What does Number Needed to Harm (NNH) mean?
NNH = 1 / risk difference (for adverse event).
Higher = safer drug.