Human Nutrition Unit 7
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
24 Terms
Compare fat-soluble vitamins with water-soluble vitamins
Fat-soluble vitamins (A, D, E, K) are stored in the body's fatty tissue and liver, while water-soluble vitamins (B-complex and C) are not stored and need to be consumed more regularly. Fat-soluble vitamins can accumulate to toxic levels, whereas water-soluble vitamins are excreted in urine if in excess.
Fat-soluble vitamins
A, D, E, K
Water-soluble vitamins
B-complex vitamins and vitamin C
Fat-soluble vs. water-soluble vitamins Chart
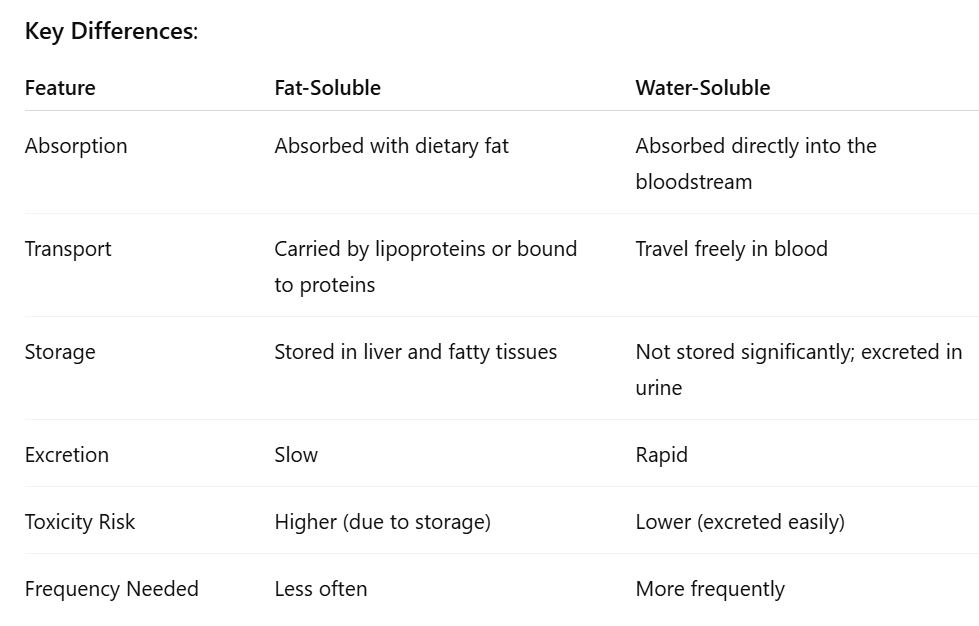
Absorption solubility effects
fat-soluble vitamins require bile and fat; water-soluble vitamins dissolve easily in water and are absorbed directly
Transport solubility effects
Fat-soluble vitamins use carriers or chylomicrons; water-soluble vitamins circulate freely.
Storage solubility effects
Fat-soluble vitamins are stored in the body's fatty tissues and liver, while water-soluble vitamins are not stored and excess amounts are excreted in urine.
Excretion solubility effects
fat-soluble vitamins are retained longer; water-soluble are readily excreted in urine
Toxicity solubility effects
fat-soluble vitamins are more prone to toxicity (A & D); water-soluble vitamins have low toxicity, though medadoses can still be harmful
Requirements of solubility
Refers to how the solubility of vitamins affects their absorption, storage, and excretion in the body, influencing overall nutritional needs. Water-soluble vitamins need regular replenishment; fat-soluble can be taken less frequently due to storage
Roles of vitamin A & consequences of deficiency
Functions: Vision (component of rhodopsin), immune function, skin health, reproduction, cellular growth and differentiation.
Deficiency Symptoms: Night blindness, dry eyes (xerophthalmia), impaired immunity, stunted growth in children, keratinization of epithelial tissues.
Global problems & interventions of vitamin A deficiency
Global issues include high rates of vision impairment and increased mortality in children. Interventions often involve supplementation programs, food fortification, and improving dietary diversity. This reduces child mortality and improves vision and immune health
Vitamin A Toxcicity
Excessive intake of vitamin A can lead to toxicity, causing symptoms such as nausea, headache, dizziness, and in severe cases, liver damage and intracranial pressure increases.
Acute toxicity: nausea, vomiting, headache, blurred vision, dizziness
Chronic toxicity: liver damage, bone pain, birth defects, dry skin, fatigue
Vitamin A recommendations and sources
RDA: 700ug/day for women, 900ug/day for men
Sources: liver, dairy, eggs, carrots, sweet potatoes, leafy greens
Suuplements vs. food: whole foods are safer due to lower toxicity risk, supplements can be helpful in deficiencies but pose risk when overused
Roles of Vitamin D
Bone health (enhances calcium and phosphorus absorption), immune regulation, cell growth and neuromuscular functionand reduction of inflammation.
Vitamin D Deficiency Problems
can lead to rickets (bone softening, deformities) in children and osteomalacia (bone pain, muscle weakness) in adults, resulting in weakened bones, increased risk of fractures, and muscle weakness.
Vitamin D is fat-soluble
Essential for calcium metabolism, helping to maintain bone health and immune function.
Absorption: Requires dietary fat and bile.
Transport: Bound to vitamin D-binding protein in blood.
Storage: Stored in fat tissue and liver.
Excretion: Limited; retained longer.
Toxicity: Possible in excessive supplement use – symptoms include hypercalcemia, kidney stones, nausea, weakness.
Requirements: Less frequent due to storage. RDA: 600–800 IU/day (15–20 mcg).
Vitamin D Synthesis & Activation Process
The process by which the body produces vitamin D through skin exposure to sunlight, followed by conversion in the liver and kidneys to its active form, calcitriol. This process is crucial for calcium homeostasis and overall health. Some factors that affect synthesis is latitude, skin color, sunscreen use, clothing, age, and time of day/season
Sources and recommendation for Vitamin D
Include sunlight, fatty fish, fortified foods, and supplements. Recommended intake varies by age and exposure. Fatty fish (salmon), egg yolks, fortified milk and cereals. Sunlight 10 to 30 mins/day for lights skin; longer for darker skin to produce adequate levels of vitamin D. For supplements, the intake should be adjusted based on individual needs and health status.
Vitamin C (Ascorbic Acid)
A water-soluble vitamin that functions as an antioxidant, supports the immune system, aids in collagen synthesis, and enhances iron absorption from plant-based foods.
Deficiency: Scurvy – bleeding gums, fatigue, poor wound healing, joint pain.
Toxicity: Rare but high doses may cause diarrhea, kidney stones, GI distress.
DRI: 90 mg/day (men), 75 mg/day (women); smokers need +35 mg/day.
UL (Upper Limit): 2,000 mg/day.
Tower of Recommendations:
Base level: 75–90 mg/day (basic health)
Moderate: 200–500 mg/day (antioxidant function)
Upper limit: Up to 2,000 mg/day short term if needed, but not daily
Sources: Citrus fruits, strawberries, bell peppers, broccoli, kiwis.
Vitamin C Water-soluble
Vitamins that act as antioxidants, support immune health, and are essential for collagen production.
Absorption: Directly into bloodstream.
Transport: Freely in water-based blood plasma.
Storage: Minimal; not stored significantly.
Excretion: Rapid via urine.
Toxicity & Requirements: Low toxicity; frequent intake needed due to excretion.
Folate (vitamin B9)
A water-soluble B vitamin essential for DNA synthesis, repair, and methylation, as well as red blood cell formation. Folate is crucial during periods of rapid growth such as pregnancy and infancy.
Sources: Leafy greens, legumes, citrus fruits, fortified grains.
Roles: DNA synthesis, cell division, red blood cell formation, fetal neural tube development.
Deficiency: Neural tube defects, anemia, elevated homocysteine.
Toxicity: Can mask B12 deficiency symptoms.
DRI: 400 µg/day; 600 µg for pregnant women.
Fortification: Required in many countries to prevent birth defects—especially before and during early pregnancy.
Vitamin B12 (Cobalamin0
A water-soluble vitamin important for red blood cell formation, nerve function, and DNA synthesis. It is primarily found in animal products and is essential for maintaining healthy nerve cells.
Sources: Animal products (meat, dairy, eggs), fortified foods for vegans.
Roles: Red blood cell formation, nerve function, DNA synthesis.
Deficiency: Pernicious anemia, nerve damage, memory loss.
DRI: 2.4 µg/day.
Malabsorption Causes: Lack of intrinsic factor (autoimmune), gastric surgery, aging, vegan diet.
Folate-B12 Connection: Both work in DNA synthesis; B12 deficiency traps folate in inactive form, worsening anemia.
Vitamin B12 & Folate solubility
Both are water-soluble vitamins that play crucial roles in DNA synthesis, red blood cell formation, and overall cellular function.
Absorption:
Folate: absorbed in small intestine.
B12: requires intrinsic factor and stomach acid.
Transport: Freely (Folate), protein-bound (B12).
Storage: Folate – limited; B12 – stored in liver for years.
Excretion: Folate – urine; B12 – minimal excretion.
Toxicity Risk: Low for both, but high folate can hide B12 deficiency symptoms.