Looks like no one added any tags here yet for you.
Urethral Caruncle
Eversion of a portion of the distal urethra, usually at posterior aspect in postmenopausal AFAB
S/S: chronic inflammation of exposed mucosa may lead to enlargement, bleeding, necrosis
Tx: Topical estrogen
Urethral Prolapse
Circumferential eversion of the urethral mucosa around the urethral meatus, usually in prepubertal females 2-10 yo
Tx: short-course Topical Estrogen, sitz baths
**Refer to Urology if not improved in a few weeks
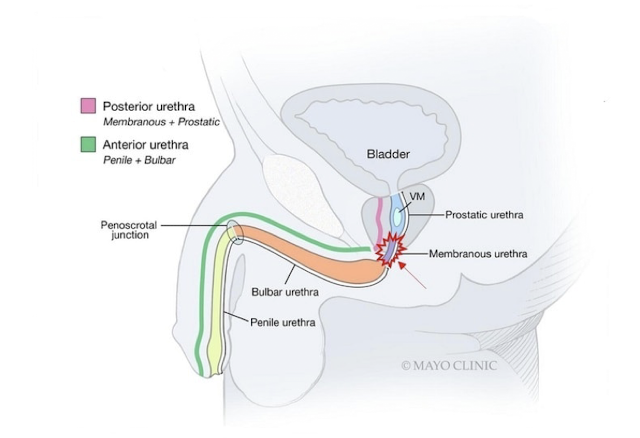
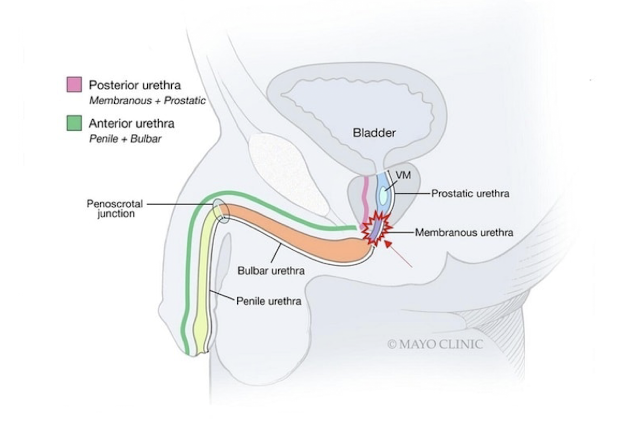
Urethral Stricture
Abnormal tissue that narrows the lumen of the urethra, may be limited to mucosa or involve deep tissue layers, can be singular or multifocal
- typically affecting AMAB; idiopathic, iatrogenic, inflammatory causes
- anything inserted into the urethra (rigid camera, rigid catheterization) radiation therapy, STIs
S/S:
- Acute/chronic weak urine stream
- Have to push or strain to maintain urine stream
- Urine "sprays/splits"
± acute urinary retention, recurrent UTIs
Urethral Stricture
Dx: H&P (trauma, insertions, urinary symptoms, inspect urethral meatus)
- Uroflow
- PVR
-Refer to Urology if imaging is needed (retrograde urethrogram)
Tx:
- Cystoscopy
- Dilation: cystoscopy or intraoperatively
- maintenance with clean intermittent catheterization (CIC) at home
- Surgery
*often recurring issue
Urethritis
Inflammation of the urethra, mainly infectious (STIs most common)
Risk factors: AMAB, young (mid 20s), sexually active, multiple partners, no condoms
Gonococcal or non-gonococcal (Chlamydia trachomatis, Mycoplasma genitalium, Trichomonas vaginalis)
Urethritis
S/S:
- Dysuria
- Urethral discharge (typically purulent in gonorrhea, thin/mucoid in chlamydia)
Dx: Urine NAAT, H&P, Gram Stain*, urinalysis
Tx:
- Gonorrhea: Ceftriaxone IM x1 (500 mg if <150 kg or 1 g if ≥150 kg)
- Chlamydia: Doxycycline 100 mg BID x7 days
Balanitis
Inflammation of the glans of the penis
-can involve foreskin & glans
-infectious & non-infectious causes
Risk factors: lack of circumcision (smegma), diabetes mellitus, obesity
Dx: clinical diagnosis: H&P, suspected etiology
Tx: general hygiene: retract foreskin to clean, wash with saline BID, wear loose fitting underwear undergarments
- Fungal: Clotrimazole 1% or Miconazole 2% cream BID 7-14 days
**If not improved: hydrocortisone 1% BID 7 days, or Refer to Derm or Urology
Phimosis
Difficulty or inability to retract the foreskin
- Present in almost all newborn males due to adhesions
Risk Factors: UTI, balanitis, paraphimosis
S/S: Difficultly with hygiene/urination
Tx:
- Gentle retraction
- Topical steroids|
- Dorsal slit or circumcision
Paraphimosis
Inability to protract the foreskin once it has been retracted
Risk factors: GU procedures (catheterization), sexual activity, phimosis
Tx: Manual Reduction; ice, compression, analgesia (2% lidocaine), urology consult, inspect the glans for necrosis (firm, black/blue color)
** If you retract foreskin, put it back
Hypospadias
Urethral meatus opens “below” normal/expected anatomical location (ventral aspect)
-relatively common, genetic + environmental (androgen disruption)
S/S: cosmetically bothersome or interferes with urination
Tx: no treatment, surgical management if needed
Epispadias
Urethral meatus opens “above” normal/expected anatomic location (dorsal aspect)
-relatively uncommon
S/S: more likely associated with other abnormalities of GU tract and difficulties with urination (bladder exstrophy)
Erectile Dysfunction (ED)
The consistent or recurrent inability to acquire or sustain an erection of sufficient rigidity and duration for sexual intercourse
Risk factors: cardiovascular disease (CVD), diabetes mellitus, hypertension, obesity, dyslipidemia, hypogonadism, smoking, depression, medication use
Erectile Dysfunction (ED)
S/S: inability to maintain an erection, nocturnal erections (common)
Dx: H&P, Sexual Health Inventory for Men (SHIM) / Internal Index of Erectile Dysfunction (IIEF): high score = good
Tx: Modify risk factors (smoking cessation, weight loss, counseling)
-PDE-5 inhibitors are first-line medical therapy (oral, urethral suppository, injectable forms)
-Mechanical: ring, vacuum pump, VED
-Surgery: penile prosthesis
Function of Penis
_________:
- Elimination of urine
- Delivery of genetic material for fertilization
*urine and sperm exit through urethral meatus
PDE-5 inhibitors
Which medication class is contraindicated in men taking nitrates, causing severe hypotension?
Drugs: Sildenafil (Viagra), Tadalafil (Cialis), Vardenafil (Levitra), Avanafil (Stendra)
Peyronie Disease
Acquired localized fibrotic disorder of the tunica albuginea resulting in penile deformity, mass, pain, potential erectile dysfunction
Risk Factors: Dupuytren's contracture, injury or trauma to penis, connective tissue disorder, increasing age, family history
Peyronie Disease
S/S:
- Painful erection
- Penile deformity during erection
- Erectile dysfunction (20-50%)
Dx:
PE: non-tender plaques/indurations on shaft of penis (dorsal aspect most common)
-Ultrasound
Tx:
- Oral Pentoxifylline
- Intralesional injections (collagenase)
- Surgery (but may recur)
Priapism
Persistent and painful erection for at least 4 hours not associated with sexual stimulation or desire
-unknown etiology, bimodal distribution (5-10yo - 20-50yo)
-Sickle cell disease (most common in kids)
-Inappropriate use of erectile medications/intercavernosal injections (most common in adults)
Pathophysiology:
1. Ischemic (veno-occlusive or low flow, more common, MEDICAL EMERGENCY)
2. Nonischemic (arterial or high flow), less common, usually due to trauma, not an emergency, usually resolves spontaneously
Priapism
S/S:
- Sustained painful/rigid erection
- Penile necrosis, gangrene
- Corpus spongiosum and glans are often flaccid
Dx: Cavernosal Blood Gas Analysis (to distinguish ischemic/nonischemic); Doppler US
Tx: Remove excess blood
<4 hrs (intracavernosal injection of sympathomimetic drug (Phenylephrine)
>4 hrs (Aspiration, +/- irrigation, phenylephrine)
**ISCHEMIC IS MEDICAL EMERGENCY
Priapism
Kids with sickle cell disease may present with the ischemic form of which penile condition (MEDICAL EMERGENCY)?
Penile Cancer
very rare malignancy
Risk Factors:
-Presence of foreskin (uncircumcised - greatest risk factor!)
-Chronic inflammation (phimosis, poor hygiene)
-increasing age (>50yo)
-HPV infection (HPV-16)
-Smoking
-HIV infection (immunosuppression, STIs)
Penile Cancer
S/S: Non-healing penile lesions >6 weeks on glans, corona, prepuce, often ulcerative, can be nodular
- May be painful, typically painless
- Inguinal lymphadenopathy (sign of advanced disease)
Dx:
- PE: non-healing penile lesion >6 weeks
- Biopsy (derm or urology) followed by CT/MRI (check for metastasis)
Tx:
-surgical amputation of primary tumor (definitive for SCC)
-topical Fluorouracil or laser for carcinoma in situ
-Lymphadenectomy, chemotherapy and/or radiation
Penile Cancer
What rare penile disorder is typically squamous cell carcinoma (SCC)?