Personality Disorders (L2)
5.0(1)
Card Sorting
1/36
There's no tags or description
Looks like no tags are added yet.
Study Analytics
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
37 Terms
1
New cards
What are personality disorders?
Deviations from "normal" on traits that everyone has (e.g. people who are high on distrustfulness might have paranoid PD)
2
New cards
What are criteria for personality disorders in general?
* Inflexible thoughts/feelings compared to normal personality
* Originates in early development
* Present in early adulthood
* Dysfunctional (sometimes only experienced by others as such)
* Related to high healthcare costs, healthcare consumptions, societal costs and low quality of life
* A way of "Who I am"
* Personality disorders are **ego-syntonic**
* Originates in early development
* Present in early adulthood
* Dysfunctional (sometimes only experienced by others as such)
* Related to high healthcare costs, healthcare consumptions, societal costs and low quality of life
* A way of "Who I am"
* Personality disorders are **ego-syntonic**
3
New cards
What did Ribot state about personality?
Three primary personality types, divided into subtypes along dimensions (normal and abnormal)
4
New cards
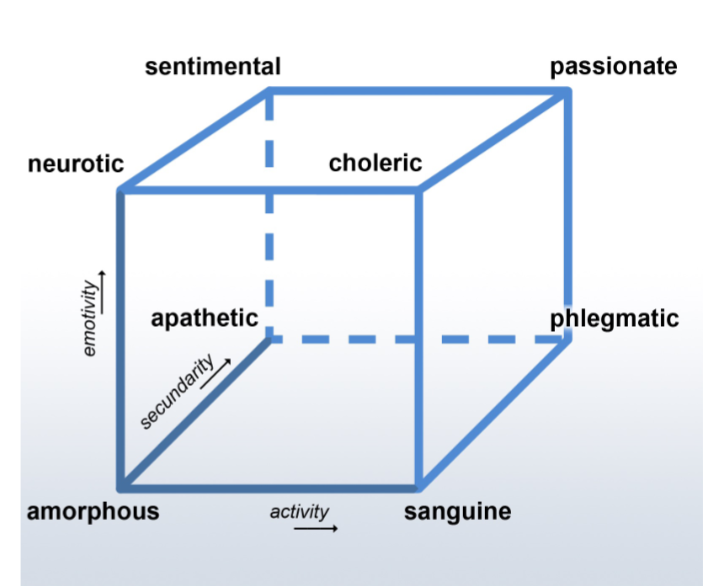
What is Heyman’s cube?
A dimensional model of personality
5
New cards
What did Kraeplin do?
Created psychopathic PD types. This was influential for DSM thinking - PDs are deviations from normality, not categorically different
6
New cards
What are the 3 P’s that need to be the case to classify something as a personality disorder?
* Persistent
Stable and long duration, since early adulthood
* Pathological
Problematic (causes distress towards you or someone else or impairment)
* Pervasive
Needs to be there in multiple domains
Stable and long duration, since early adulthood
* Pathological
Problematic (causes distress towards you or someone else or impairment)
* Pervasive
Needs to be there in multiple domains
7
New cards
What is “normal” personality?
* A habitual way of thinking, feeling and acting
Consistent(ish) across time, but situational variance is high
Consistent(ish) across time, but situational variance is high
8
New cards
Is personality stable over time?
Personality is not unchanging, but stabilizes with increasing age, with largest changes around 25- 30 because of increasing responsibilities and corrective feedback from the environment (conditioning)
9
New cards
What is the prevalence of having at least one personality disorder?
General population: 9-13%
Outpatient care: 30-50%
Inpatient care: 50-70%
Outpatient care: 30-50%
Inpatient care: 50-70%
10
New cards
Why are prevalence studies of personality disorders sometimes problematic?
* Almost no international studies
* Different sampling methods, study instruments
* Poor diagnostic reliability
* Different sampling methods, study instruments
* Poor diagnostic reliability
11
New cards
What tends to be the course of PDs?
Develops in adolescence \n • Improves during development \n • Not more chronic compared to chronic syndrome disorders (schizophrenia/ bipolar)
12
New cards
What is the monothetic vs polythetic view of personality disorders?
**Monothetic:** Members must met the same properties of criteria
**Polythetic:** There can be different ways to come up with a definition (some criteria must be met)
DSM is a polythetic system because you only need some criteria to have the disorder, but the criteria doesn't need to be the same for every person
13
New cards
How are most disorders, and how are disorders presented in the DSM?
* Most disorders are dimensional (exceptions: schizotypal, autism, SUDs)
* DSM is categorical, arbitrary cut-off
* Dimensional diagnosis is very difficult because people naturally think in different categories
* DSM is categorical, arbitrary cut-off
* Dimensional diagnosis is very difficult because people naturally think in different categories
14
New cards
What is Cluster A of PDs and what disorders are included in it?
Bizarre (variant psychosis)
* Paranoid PD (Distrust)
* Schizotypal (Ideas of reference, psychotic fear)
* Schizoid PD (isolation; no desires or flattened affectivity)
* Paranoid PD (Distrust)
* Schizotypal (Ideas of reference, psychotic fear)
* Schizoid PD (isolation; no desires or flattened affectivity)
15
New cards
What is Cluster B of PDs and what disorders are included in it?
Dramatic, emotional, impulsive
* Histrionic (theatrical, attention seeking)
* Narcissistic (superiority, wanting to be around high-status people)
* Borderline (emotional instability)
* Criminal behaviour (no conformation norms, criminal)
* Histrionic (theatrical, attention seeking)
* Narcissistic (superiority, wanting to be around high-status people)
* Borderline (emotional instability)
* Criminal behaviour (no conformation norms, criminal)
16
New cards
What is Cluster C of PDs and what disorders are included in it?
Internalizing (anxious, fearful)
* Avoidant PD (Avoiding for fear of negative evaluation)
* Dependent PD (Clinging to a helper, feel that they cannot make decisions on their own)
* Obsessive-compulsive PD: odd one out lol
* Avoidant PD (Avoiding for fear of negative evaluation)
* Dependent PD (Clinging to a helper, feel that they cannot make decisions on their own)
* Obsessive-compulsive PD: odd one out lol
17
New cards
What other personality disorders can exist apart from the clusters?
Personality Change due to another medical condition (Stroke, brain trauma)
Other specified personality disorder
* Satisfies multiple criteria of various PDs, but does not satisfy criteria for 1 single PD
* Non-DSM PDs
* **Most commonly diagnosed**
Unspecified PD
Other specified personality disorder
* Satisfies multiple criteria of various PDs, but does not satisfy criteria for 1 single PD
* Non-DSM PDs
* **Most commonly diagnosed**
Unspecified PD
18
New cards
What comorbidities often exist in personality disorders with other personality disorders?
* Rule rather than exception
Within PDs
Often:
* Cluster C (avoidant and obsessive-compulsive)
* Cluster B (antisocial and borderline)
* Between clusters (borderline and avoidant)
Within PDs
Often:
* Cluster C (avoidant and obsessive-compulsive)
* Cluster B (antisocial and borderline)
* Between clusters (borderline and avoidant)
19
New cards
What comorbidities often exist in personality disorders with syndrome disorders?
* Avoidant PD and depression
* OCPD and burnout/depression
* Borderline PD and PTSD
* General comorbidity: PDs with anxiety, depression and addiction (SUDs)
* OCPD and burnout/depression
* Borderline PD and PTSD
* General comorbidity: PDs with anxiety, depression and addiction (SUDs)
20
New cards
What is the life expectancy of someone with a personality disorder and why is that the case?
On average, 18 years shorter
Risk highest before 44 years (10x mortality rate)
Because of stress, medication
Risk of cardiovascular diseases
Risk of intergenerational transmission
Risk highest before 44 years (10x mortality rate)
Because of stress, medication
Risk of cardiovascular diseases
Risk of intergenerational transmission
21
New cards
What is important when classifying and diagnosing personality disorders?
To also assess comorbid syndrome disorders
To use a semi-structured interview (diagnoses based on clinical expertise have low reliability)
To beware of stigma (to not over- or underdiagnose something because of the client belonging to a certain group)
To use a semi-structured interview (diagnoses based on clinical expertise have low reliability)
To beware of stigma (to not over- or underdiagnose something because of the client belonging to a certain group)
22
New cards
What types of stigma exist for personality disorders?
* Internalized (blaming self for all problems, leads to low self-esteem and/or depression)
* Discrimination (in housing, jobs, etc)
* Seeing the person as a danger or blaming them for all their problems
\
Often in BPD and APD
* Discrimination (in housing, jobs, etc)
* Seeing the person as a danger or blaming them for all their problems
\
Often in BPD and APD
23
New cards
What works best for treatment of PDs and what doesn’t work as well?
Specialized psychotherapy (treatments developed to treat PDs) work best.
Additional treatment can be effective (e.g. for PTSD or phobias)
* Needs to be sufficient motivation
* Social psychiatric treatment (if first choice is not possible, lack of motivation)
* Pharmacological treatment **cannot treat personality disorders, only other symptoms that arise from them**
There is an exception for this of BPD, but it’s important to consider
Additional treatment can be effective (e.g. for PTSD or phobias)
* Needs to be sufficient motivation
* Social psychiatric treatment (if first choice is not possible, lack of motivation)
* Pharmacological treatment **cannot treat personality disorders, only other symptoms that arise from them**
There is an exception for this of BPD, but it’s important to consider
24
New cards
What types of abuse and neglect exist?
Emotional, sexual, physical abuse
Emotional and physical neglect
Emotional and physical neglect
25
New cards
What are the rates for abuse in people with PDs and what does that lead to?
Between 11% sexual abuse, 26.7% emotional abuse
Leads to:
* Poorer mental health
* PTSD
* Physical diseases
* Personality disorders
Leads to:
* Poorer mental health
* PTSD
* Physical diseases
* Personality disorders
26
New cards
What forms of abuse are especially common in what disorders?
Borderline very associated w sexual abuse, Antisocial PD with physical abuse
Emotional abuse associated with Cluster C disorders (inconsistent parental reinforcement)
Emotional abuse associated with Cluster C disorders (inconsistent parental reinforcement)
27
New cards
Why does abuse lead to PDs?
**Attachment:**
(insecure attachment and distrust of others)
* Approach-avoidance
Emotion regulation
* Coping
* Negative self-views
* Memory encoding
28
New cards
What did the study on problematic parenting show?
Study: Amount of problematic parenting behaviours positively correlated with the probability of child developing a PD
29
New cards
Mediation model
Problematic parenting behaviour mediates the model - it doesn't matter if parents have disorders as long as they are good parents
30
New cards
What treatment models are offered for comorbid disorders with PDs?
Psychodynamic model: every syndrome disorder is the result of underlying personality problems, so treatment should focus on the personality disorder.
CBT model: (initially) denied the existence of personality disorders, so treatment should focus solely on the syndrome disorder.
• Parallel treatment: rarely, highly specialized treatments parallel treatments are offered.
• Stepped care: currently, (presumed) syndrome disorders are usually treated first. Only when this does not provide sufficient improvement, patients are offered a treatment for the specific PD. In few cases where personality problems are so pronounced that they overshadow any syndrome disorder (often in borderline PD), treatment is directly aimed at PD.
CBT model: (initially) denied the existence of personality disorders, so treatment should focus solely on the syndrome disorder.
• Parallel treatment: rarely, highly specialized treatments parallel treatments are offered.
• Stepped care: currently, (presumed) syndrome disorders are usually treated first. Only when this does not provide sufficient improvement, patients are offered a treatment for the specific PD. In few cases where personality problems are so pronounced that they overshadow any syndrome disorder (often in borderline PD), treatment is directly aimed at PD.
31
New cards
In the case of comorbid PD and syndrome disorders, what is treated first?
Whichever disorder is the primary disorder (aka which problem is the most serious/urgent)
32
New cards
If the syndrome disorder is the primary disorder, what is the treatment?
In general, psychosocial treatments can be used when a syndrome disorder is the primary disorder. However, it is recommended that this treatment does not continue for too long: if unsuccessful, the problem might not be sufficiently independent of PD.
33
New cards
If the personality disorder is the primary disorder, what is the treatment?
When PD is the main focus, specialized psychotherapy is the treatment of choice. These therapies are based on specific theories about the development and maintenance of PDs.
For borderline PD, these treatments include a) dialectical behavior therapy (DBT), b) schema therapy (ST), c) transference-focused therapy (TFP), and d) mentalization-based treatment (MBT). For the other PDs, they include ST, and specialized types of CBT and psychodynamic psychotherapy.
For borderline PD, these treatments include a) dialectical behavior therapy (DBT), b) schema therapy (ST), c) transference-focused therapy (TFP), and d) mentalization-based treatment (MBT). For the other PDs, they include ST, and specialized types of CBT and psychodynamic psychotherapy.
34
New cards
What is the best treatment for PDs?
Specialized psychotherapies for PDs systematically outperform treatment as usual, while more generic treatments do not
35
New cards
Is there any evidence for a negative impact of comorbid PD on the effects of treatment for syndrome disorders?
No, but individuals with comorbid PDs may experience more severe problems
36
New cards
How does one diagnose personality disorders?
Because there are no detection instruments, the clinician has to pay attention to long-lasting dysfunctional patterns of cognitions, emotions and behaviour.
37
New cards
When should you prioritize treatment of the PD, even when it’s not necessarily the primary disorder?
When there are strong beliefs related to mistrust, magical thinking, need for control, avoidance of emotions, dependence or hopelessness.