Lower Extremity Arterial Testing and Evaluation
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
98 Terms
What is a basal state?
Steady state in metabolism of systemic blood pressure
What is an ABI?
Ankle to brachial index
What are segmental pressures?
Blood pressures obtained from cuffs placed around ankles, calves, and thighs
What is infrainguinal?
Below groin
What are the indirect physiologic tests?
Pressure assessment
Plethysmography
Doppler waveform analysis
Exercise stress test
What is a pressure assessment?
ABI
Segmental pressures
What is plethysmography?
Pulse volume recording (PVR)
Photoplethysmography (PPG)
What are the different bruit grades?
Grade 1+: Mild
Grade 2+: Moderate
Grade 3+: Severe
What is considered to be a “severe" bruit?
Abnormal blood flow that extends throughout diastole
What is the proper technique for Doppler waveform analysis of the lower arteries?
Patient in basal state or warm room
High frequency CW transducer
Transducer at 40-60 degree angle to skin
Obtain clean waveforms
What is analog analysis?
Use of zero crossing frequency meter to display waveforms on a graph or strip chart
What are the disadvantages of analog analysis?
Noise
Overestimates high frequencies
Underestimates low frequencies
Angle of insonation is operator dependent
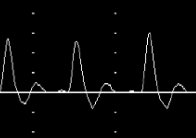
Identify this image.
Analog zero-crossing detector
What is spectral analysis?
Use of FFT to display velocities or frequencies and amplitudes of backscattered signals
What is an advantage of spectral analysis?
Increased sensitivity to display multiple frequencies at once
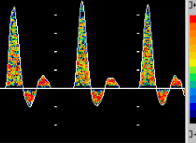
Identify this image.
FFT color spectrum analyzer
Doppler analysis is…
Qualitative
What is happens to the acceleration time (AT) if there is an obstruction proximal to the probe?
Increased AT or tardus parvus waveform
What is happens to the acceleration time (AT) if there is an obstruction distal to the probe?
No change in AT
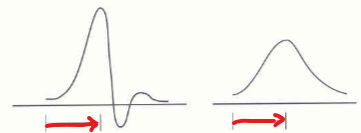
Identify this image?
Acceleration time (AT)
(T/F) Degree of obstruction cannot be determined on the basis of waveforms alone.
True; Collateralization of occlusions can restore flow distal to an occluded vessel
(T/F) Monophasic waveforms can only be obtained distal to an obstruction.
False; Monophasic waveforms can be obtained proximal AND distal to an obstruction
What is the segmental pressure principle?
Normal individuals in supine: Ankle systolic pressure ≥ Brachial systolic pressure
What is the proper technique for segmental pressure analysis of the lower arteries?
Patient in basal state or warm room
Patient in supine position with extremities at level of heart
Correct cuff size and placement
What is the correct blood pressure cuff size?
20% greater than diameter of limb
40% of limb circumference
Too tight blood pressure cuffs will…
Overestimate BP
Too loose blood pressure cuffs will…
Underestimate BP

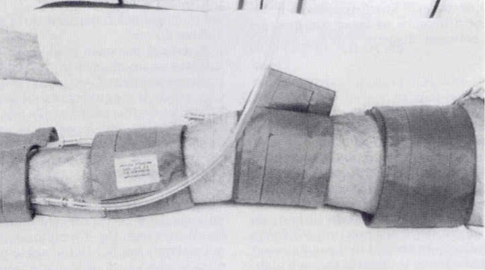
Identify this image.
A. Bladder length
B. Cuff width
What is the recommended amount of inflation to use with the blood pressure cuffs in general?
DO NOT EXCEED 220 mmHg
What is the three cuff method?
Use of one large (17-19 x 40 cm) thigh cuff with normal thigh pressure EQUAL to brachial pressure
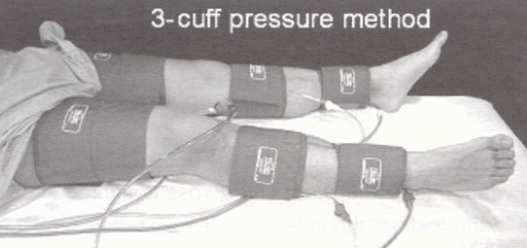
What are the normal and abnormal thigh pressure when using three cuff pressure method?
Normal: All pressures should be near equal to brachial pressure
Abnormal: Thigh pressure is 20-30 mmHg less than brachial pressure
What is the four cuff method?
Use of two smaller (12 × 40 cm) thigh cuffs to provide proximal and distal thigh pressures
What are the normal and abnormal pressure when using the four cuff method?
Normal high (proximal) thigh pressure: Thigh pressure is 20 mmHg greater than brachial pressure
Abnormal high (proximal) thigh pressure: Thigh pressure less than brachial pressure
Abnormal: High thigh and low thigh having a 30 mmHg pressure difference is suggestive of SFA disease
Why is there a pressure artifact when using the four cuff method?
Use of narrow high thigh cuff that elevates pressure 20-30 mmHg
What is the key difference between the three cuff and the four cuff method?
Four cuff method can differentiate between aortic-iliac (AI) and superficial femoral (SFA) disease
In general, what is considered to be a significant pressure gradient or drop in pressure for an abnormal ABI?
30 mmHg

Identify this image.
Abnormal left pressure due to decrease in at least 20 mmHg suggesting subclavian artery disease
What is the formula for finding the ABI?
Bilateral ankle pressures divided by highest brachial pressure
What is the highest ankle pressure marker used for?
Reported for ABI
What is the lowest ankle pressure marker used for?
Marker for PAD
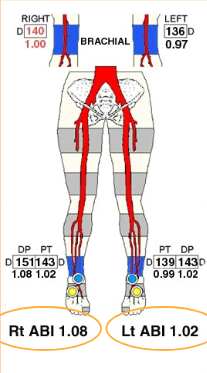
Identify this image.
Normal ABI
What are the normal resting ABI values?
> 1.35 = Probable calcified arteries
1.0-1.34 = NORMAL
0.9-1.0 = Minimal arterial disease
< 0.9 = Abnormal
< 0.8 = Probable claudication (leg pain w/ exertion)
< 0.5 = Multi-level disease and long segment occlusion
< 0.3 = Rest pain, severe disease, ischemia
< 0.2 = Tissue loss or gangrene
What occurs when systemic blood pressure is less than 100 mmHg or greater than 200 mmHg?
Ankle pressure is typically 25% lower than brachial pressure
In healthy (normal) people, what is the difference between systolic ankle pressure and systolic arm (brachial) pressure?
Systolic pressure in ankle is normally HIGHER than in arm due to amplified BP as blood travels away from heart
How do you distinguish between the dorsalis pedis artery (DPA) and the posterior tibial artery (PTA)?
DPA= Easily compressed and harder to locate
PTA= Harder to compress and easier to locate

Identify this image.
DPA for ABI

Identify this image.
PTA for ABI
(T/F) The probe should be held at a 90 degree angle when locating the PTA.
False; 45-60 degrees is best
What are the steps for taking segmental pressures?
Inflate cuffs to at least 20 mmHg above systolic arm pressure
Narrow high-thigh cuff inflated to 40 mmHg above arm pressure
Pause for a moment
Slowly lower pressure
Record returning systolic pressures
Which of the lower arterial test modalities provides diagnostic quantitative information?
Segmental pressures
What is photoplethysmography (PPG) when discussing segmental pressures?
Measurement of change in SYSTOLIC AND DIASTOLIC blood volume in different parts of body using infrared light to detect RBCs
What are the advantages of PPG segmental pressures?
Less operator dependent
Bilateral capability
What are the disadvantages of PPG segmental pressures?
No audible signal
Not able to use with severe disease
Motion and ambient light artifact can cause false readings
How do we take toe or digital pressures?
Cuff on toe or other digit that takes small pressures (1.9 or 2.5) alongside use of PPG transducer to display SYSTOLIC blood flow

When are toe pressures used?
Evaluating small vessel disease
Evaluating calcified, incompressible large vessels in diabetic patients
What is the normal toe / brachial index (TBI)?
Normal > 0.75 (60-80%)
What is the abnormal toe / brachial index (TBI)?
Abnormal < 0.66
What are the limitations of segmental pressure exams?
Diabetics medial calcinosis or calcification of arteries
Chronic steroid therapy
Renal dialysis patients
Segmental pressures unobtainable or excessively high (ABI > 1.35) PTA
In those with calcified arteries (medial sclerosis), how must you determine limb perfusion (BP)?
Combination of PVR, Doppler waveform analysis, or toes pressures due to unusable segmental pressures
What are some calcification clues?
Incompressible artery
Unobtainable pressures
Excessively high ABI (> 1.35)
High distal limb pressure
What is the correct way to obtain an ABI?
Right ankle / Highest arm or brachial
Left ankle / Highest arm or brachial
Lowest of two = ABI
(T/F) Toe pressures are more reliable than ankle pressures.
True; Toe vessels are less likely to be affected by calcification
When should exercise or stress testing be utilized when measuring ABIs?
Patient complains of intermittent claudication
ABI of 0.85-0.5
When should exercise or stress testing NOT be utilized when measuring ABIs?
Patient on Beta Blockers or Isorobides because they will not allow increase in heart rate
Patients with pulmonary or cardiac disease
ABI < 0.3
What can be interpreted from an exercise or stress ABI?
Ankle pressures that drop to low levels and recover to resting levels within 2-6 minutes post exercise suggest single level obstruction
If pressures remain reduced for up to 12 minutes, multilevel obstructions are present
What is the normal ankle pressure response to exercise or stress ABI testing?
No change to slight increase in pressure
What is the exercise or stress pressure value that indicates vascular claudication?
Ankle pressure of 60 mmHg or less
What is a substitution for a treadmill for an exercise or stress ABI?
Toe raises for one minute or until claudication symptoms return
What is assessed during exercise or stress ABI?
Exercise tolerance
Recovery time
Pressure drop
Diagnose leg pain
What are the disadvantages of an exercise or stress ABI?
Detects hemodynamically significant disease or > 60% stenosis
Cannot distinguish stenosis from occlusion
Locates general area of disease
What is the alternate test to an exercise or stress test?
Reactive hyperemia (PORH)
What is reactive hyperemia testing (PORH)?
Alternative method for stressing peripheral circulation system by inflating cuffs 20-30 mmHg above brachial pressure for 3-5 minutes
What is the result of a reactive hyperemia test (PORH)?
Ischemia and vasodilation distal to cuff
Single vessel disease seen as < 50% pressure drop in ankle
Multi-level disease seen as > 50% pressure drop in ankle
What is pulse volume plethysmography (EVR or PVR) when discussing segmental pressures?
Measurement of change in SYSTOLIC blood volume in different parts of body using pneumo-plethysmography, Doppler waveforms, and segmental pressures
What is the recommended amount of inflation to use with the blood pressure cuffs during PVR studies?
65 mmHg
What are the advantages of pulse volume plethysmography (EVR or PVR)?
Differentiates arterial claudication from nonvascular sources
Detects true arterial disease
Locates general area of obstruction
What are the disadvantages of pulse volume plethysmography (EVR or PVR)?
Cannot be specific to a single vessel
Cannot differentiate between major arteries and collateral obstruction
Not best with obese patients
Tremor or motion artifact
(T/F) PVR can be used alone to diagnose arterial disease.
False; Collateralization of an obstruction can produce a normal PVR when segmental pressure of same region indicates severe disease
Which of the following conditions would cause an abnormal pulse volume recording (PVR) at the high-thigh location?
Significant aortoiliac disease
What is strain gage plethysmaography (SGP)?
Measurement of change in blood volume in different parts of body using a mercury-filled plastic tube
What is duplex scanning?
Combination of b-mode and PW Doppler to create images and measure blood flow
What are the advantages of duplex scanning?
Localizes arterial stenosis and occlusion
Evaluates degree of stenosis
Determines presence of aneurysms
Evaluates arterial bypass grafts and hemodialysis access grafts
Detects AV fistulas
What are the disadvantages of duplex scanning?
Presence of dressings, open wounds, skin staples, sutures limits visualization of vessels
IV sites and other puncture sites in groin inhibit visualization
Obese patients difficult to image
(T/F) Normal PW Doppler signal should show triphasic flow.
True; Biphasic and monophasic patterns are abnormal
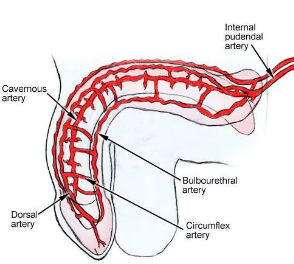
What is the blood supply to the penis?
Hypogastric artery to base of penis
Internal pudendal artery to base of penis
What is the blood supply within the penis?
Cavernosal arteries that supply main erectile tissue (corpora cavernosa)
Bulbourethral artery
Dorsal artery
With erection, flow resistance in the corpora cavernosa…
Increases
Normal erectile function requires… and…
Sufficient arterial inflow; Decreased venous outflow
What is a major cause of penile impotence?
Insufficient veno-occlusive mechanism from a venous leak
What are the risk factors of penile impotence?
Diabetes mellitus
HTN
PAD
Tobacco abuse
Arterial bypass surgeries
Prostatectomy
What is the indication for a penile arterial exam?
Determine if impotency or failure to maintain an erection is due to peripheral vascular insufficiency
What are possible reasons for vascular insufficiency to the penis?
Pelvic steal
Arterial vasospasm
Arterial occlusive disease
What size blood pressure cuff is used for a penile arterial exam?
2.5 × 12.5 cm
2.5 × 9 cm
What is the equation for a penile brachial index (PBI)?
Penile systolic pressure / Brachial systolic pressure
What are the values for PBI?
Normal= ≥ 0.75 (or 0.7-1.0)
Marginal or Borderline Normal = 0.65-0.74 (or 0.6-0.7)
Abnormal = < 0.65 (or less than 0.6)
How do you perform penile imaging?
Scan flaccid penis in trans and long views to identify plaque and locate corpora cavernosa and cavernosal arteries
Record Doppler waveforms (PSV & EDV)
Prostaglandin E-1 or Pavaparine injection
Rubber band applied to base for two minutes
Doppler PSV and EDV measurements are taken from the proximal cavernosal arteries at 5, 10, 15 and 20 minutes post injection
Normal erectile response should occur within 10 minutes and erection should be maintained for 30 minutes
What are the normal PSV and EDV values during erectile state?
PSV > 35 cm/sec
EDV > 5 cm/sec
What are the abnormal PSV and EDV values during erectile state?
PSV < 25 cm/sec
PSV > 35 cm/sec, but EDV is > 6 cm/sec (venous leak)
Vessel diameter increases less than 75%