Psychopathology- (Clinical psychology)
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
Statistical Infrequency
Behaviours that are uncommon or rare. Normally 5%
+ve - Standardised measures, not opinion based.
-ve - Traits like high IQ can be viewed as abnormal despite not causing distress
Deviation from social norms
Behaviour differs from accepted standards in society
+ve - Adapts to societal standards rather than numerical cut offs
-ve - Culturally relative. Cannot use one cultures abnormal standard to judge another.
Failure to function adequately
Individuals that cannot cope with the demands of everyday life.
+ve - Considers individuals subjective experiences as includes personal distress
-ve - Fails to identify abnormal behaviours that do not cause distress e.g. psychotic behaviour
Deviation from ideal mental health
If they lack characteristics associated with psychological well-being. Based of Jahoda’s criteria. Such as accurate representation of reality, self-actualisation, resistance to stress and more.
+ve - comprehensive, wide range of criteria that help identify mental health issues. Jahoda’s criteria acts as a threshold
-ve - Cultural issues. It reflects individualistic values like personal growth, so less applicable to collectivistic cultures that prioritise community.
Phobia characteristics
Behavioural- Avoidance, Endurance (Watch from afar), Panic (Crying and Screaming)
Emotional- Anxiety, Fear, Unrealistic thoughts to the actual threat
Cognitive- Irrational beliefs, Selective attention (Hyperfocus), Cognitive distortion (Perceptions are inaccurate
Depression Characteristics
Behaviour- (Lethargy) Change in activity levels, Changes in sleep- Insomnia and Hypersomnia, Changes in eating, High irritability
Emotional- Lower mood, Anger, Low self esteem
Cognitive- Dwell on negative, Poor concentration, Absolutive thinking (Black and white thoughts)
OCD Characteristics
Behaviour- Compulsions are repetitive, Avoidance, Compulsions to reduce anxiety
Cognitive- Obsessive thoughts, Coping strategies, Insight into own behaviour
Emotional- Anxiety and distress, Depression, Guilt and disgust
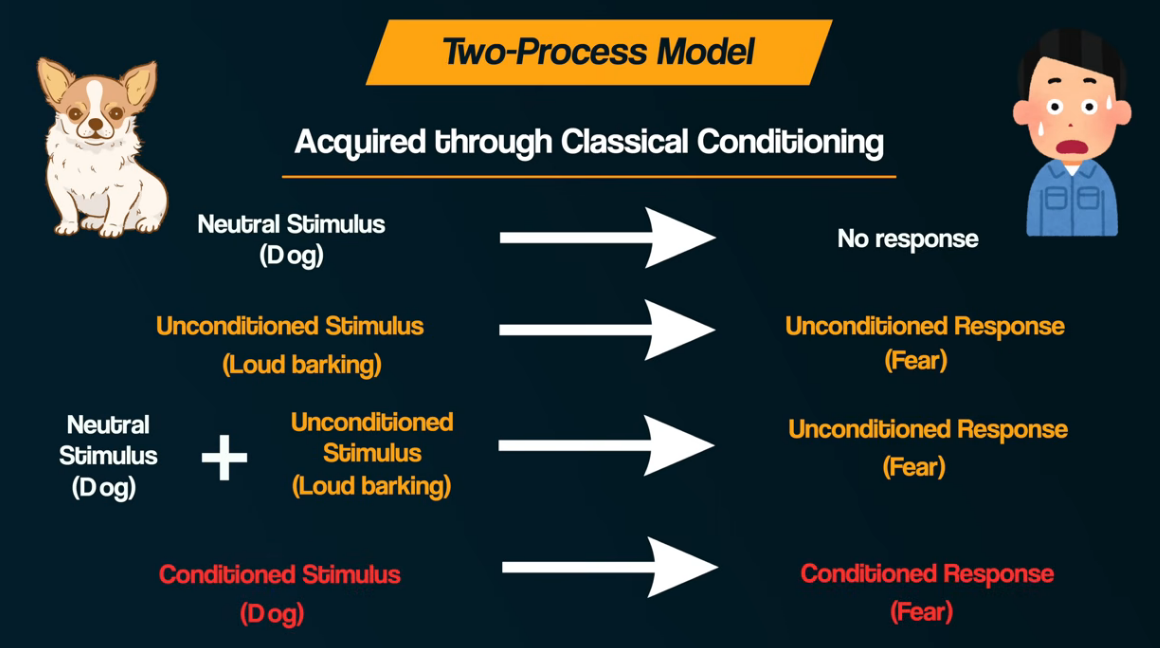
Two process model
Maintained By Operant conditioning, Avoidance rewards the person by ignoring the phobia so results in negative reinforcement
AO3 of Two process model
+ Support from the Little albert study by Watson. Classically conditioned a child to fear white rats or over similar things such as rabbits.
+ Practical application systematic desensitisation (relaxation, anxiety hierarchy, Gradual exposure)
-ve Not all phobias are learnt and its biological. People are scared of snakes but may not have encountered them.
-ve Only cares about behaviours so nothing about cognitive aspects.
Treating Phobias SD
Systematic desensitisation- Gradually exposed to phobia using an anxiety hierarchy and gradual exposure. Associating fear with relaxation over time. Reciprocal inhibition (Cant be relaxed and scared at the same time)
+ve Slowly increase proximity, not as stressful as Flooding, Build up slowly.
+ve Odgers meta analysis- Found exposure is effective, little to no difference between effectiveness of the 2
-ve Expensive
-ve Harder for people who are less willing to commit to a goal
Treating Phobias Flooding
Immediate intense exposure, no escape cannot stay in high anxiety state forever eventually relax and leads to extinction of fear as they realise phobia is safe.
+ve Cost effective, One session, Similar results to SD
-ve Ethical issues, Harder for those who are young or have intellectual disabilities.
-ve high attrition rates (Dropout rates), Schmacher- Participant said flooding as more stressful than SD
Depression- Becks explanation
Cognitive Distortions - Faulty information processing, Overgeneralising and catastrophising causing negative interpretation of life events.
Negative schemas- negative view of self based on past experiences
Negative triad- Negative views on: Self, Future, World
+ve real world application in CBT
-ve Not just cognitive factors such as serotonin
Ellis’ ABC Model
A- Activating Event (irrational thoughts triggered by events)
B- Beliefs (We have irrational thoughts)
C- Consequences A and B cause this and cause depression
+ve Real world application with REBT - Is there evidence for their beliefs, questions there logic
-ve Doesnt explain Reactive (Triggered) and endogenous depression (Cannot be traced back to an event) so it is a Half explanation
OCD Genetic explanation
OCD is Polygenetic 230 candidate genes such as SERT. OCD is believed to be aetiologically heterogeneous so some people with genes may have OCD yet others may not.
Diathesis-Stress model, People must have genetic makeup and be genetically vulnerable, the need a environmental trigger
+ve support from nestadt. Twin studies MZ twins 68% concordance rates, DZ 31% concordance. High validity and real world application.
-ve Ahmaris animal studies, Mice that had genes for ocd displayed characteristics, However not generalisable to humans.
Neural explanation OCD
OCD caused by faulty Brain regions. and through neurotransmitters and serotonin.
Frontal lobe involved in decision making and the parahippocampal gyrus which is used for emotional processing.
Serotonin is mood regulator hormone. It goes through pre synaptic nerve and is released into the the synapse where it should bind to post synaptic neurons receptors. How a lot of it is reuptake and recycled so it doesnt get recieved and this is the cause of OCD
+ve Real world use of SSRI’s are effective in treatment of OCD as prevent reuptake of Serotonin, high ecological validity.
-ve No unique neural system so we cannot be sure that SSRI’s are treating OCD fully or are only treating the depression as systems overlap. So not a full explanation.