Immunohematology Problem Solving | Quizlet
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
17 Terms
Is there a discrepancy between the following blood typing and secretor study results?
Blood typing results:
Anti-A: 4+, Anti-B: 0, A1 cells: 0, B cells: 4+
Secretor results:
Anti-A + saliva + A1 cells = 0
Anti-B + saliva + B cells = 4+
Anti-H + saliva + O cells = 0
A. No problem, the sample is from a group A secretor
B. Blood types as A and saliva types as B
C. Blood types as A, but the secretor study is inconclusive
D. No problem, the sample is from a group A nonsecretor
A. No problem, the sample is from a group A secretor
The blood typing result demonstrates A antigen on the red cells and anti-B in the serum. The secretor result reveals the A antigen in the saliva. The A antigen neutralized the anti-A, preventing agglutination when A1 cells were added. Each blood type (except a Bombay) contains some H antigen; therefore, the H antigen in the saliva would be bound by anti-H reagent. No agglutination would occur when the O cells are added.
What is the best course of action given the following test result? (Assume the patient has not been transfused recently.)
Anti-A: Mixed field, Anti-B: 0, A1 cells: 1+, B cells: 4+
A. Nothing, typing is normal
B. Type patient cells with Anti-A1 lectin and type serum with A2 cells
C. Retype patient cells; type with anti-H and anti-A,B; use screen cells or A2 cells on patient serum; run patient autocontrol
D. Wash patient cells four times with saline, then repeat the forward type
C. Retype patient cells; type with anti-H and anti-A,B; use screen cells or A2 cells on patient serum; run patient autocontrol
The mixed-field reaction with anti-A suggests a subgroup of A, most likely A3. The reverse grouping shows weak agglutination with A1 cells, indicating anti-A1. A positive reaction with anti-A,B would help to differentiate an A subgroup from group O. If A2 cells are not agglutinated by patient serum, the result would indicate the presence of anti-A1. If the patient's serum agglutinates A2 cells, then an alloantibody or autoantibody should be considered.
The following results were obtained on a 41-year-old female:
Anti-A: 4+, Anti-B: 0, A1 cells: 3+, B cells: 4+, O cells: 3+
Due to the discrepant reverse grouping, a panel was performed on patient serum revealing the presence of anti-M. How can the reverse grouping be resolved?
A. Repeat the reverse grouping with a 10-minute incubation at room temperature
B. Repeat the reverse grouping using A1 cells that are negative for M antigen
C. Repeat the reverse grouping using A1 cells that are positive for M antigen
D. No further work is necessary
B. Repeat the reverse grouping using A1 cells that are negative for M antigen
The scenario showed an antibody in the patient serum directed toward the M antigen, and the M antigen happened to be on the A1 cells in reverse grouping. To solve this problem, find A1 cells negative for the M antigen or enzyme treat the A1 cells to resolve the ABO discrepancy.
A 59-year-old male came through the emergency department of a community hospital complaining of dizziness and fatigue. History included no transfusions and a positive rheumatoid factor 1 year ago. His CBC confirmed anemia. A sample was sent to the blood bank for a type and crossmatch. Upon receipt of the sample in the blood bank, the MLS noticed the EDTA sample appeared very viscous. Fearing the sample would clog the ProVue, testing was performed using the tube method. Initial results revealed the following:
Anti-A: 0, Anti-B: 0, Anti-D: 4+, Rh control: 2+, A1 cells: 4+, B cells: 4+
The patient's red cells were washed eight times with saline, and testing was repeated giving the following results:
Anti-A: 0, Anti-B: 0, Anti-D: 4+, Rh control: 0, A1 cells: 4+, B cells: 4+
The antibody screen was negative at IS, 37 degrees Celsius, and AHG phases; check cells were positive. Crossmatch testing using two O-positive donor units revealed a 1+ at immediate spin, and negative results at 37 degrees Celsius and AHG phases. The check cells were positive In light of the crossmatch results, what is the next course of action?
A. Use other donor cells for the crossmatch
B. Perform a saline replacement for the crossmatch
C. Run the crossmatch using the Gel system
D. Result the crossmatch as incompatible
B. Perform a saline replacement for the crossmatch
The history of the patient correlates with abnormal plasma proteins causing a positive result with the Rh control. Perform a saline replacement technique to rectify the incompatible crossmatches at immediate spin.
An Rh phenotyping shows the following results:
Anti-D: 4+,
Anti-C: 2+,
Anti-E: 0,
Anti-c: 0,
Anti-e: 3+
What is the most likely Rh genotype?
A. R^1r'
B. R^0r
C. R^1R^1
D. R^1r
C.R^1R^1
The most likely genotype is R 1 R 1 . The possibilities are DCe/DCe or DCe/dCe, which translates to R 1 R 1 or R 1 r´. The former is more common.
An obstetric patient, 34 weeks pregnant, shows a positive antibody screen at the indirect antiglobulin phase of testing. She is group B, Rh negative. This is her first pregnancy. She has no prior history of transfusion. What is the most likely explanation for the positive antibody screen?
A. She has developed an antibody to fetal red cells
B. She probably does not have antibodies because this is her first pregnancy, and she has not been transfused; check for technical error
C. She received an antenatal dose of RhIg
D. Impossible to determine without further testing
C. She received an antenatal dose of RhIg
Because the patient has never been transfused or pregnant, she probably has not formed any atypical antibodies. Because she is Rh negative she would have received a dose of RhIg at 28 weeks (antenatal dose) if her prenatal antibody screen had been negative. Although technical error cannot be ruled out, it is far less likely than RhIg administration.
A patient's serum contains a mixture of antibodies. One of the antibodies is identified as anti-D. Anti-Jk^a and anti-Fy^a and possibly another antibody are present. What technique(s) may be helpful to identify the other antibody(s)?
A. Enzyme panel; select cell panel
B. Thio reagents
C. Lowering the pH and increasing the incubation time
D. Using albumin as an enhancement media in combination with selective adsorption
A. Enzyme panel; select cell panel
An enzyme panel would help to distinguish between anti-Jk a (reaction enhanced) and anti-Fy a (destroyed). Anti-D, however, would also be enhanced and may mask reactions that may distinguish another antibody. A select panel of cells negative for D may help to reveal an additional antibody or antibodies.
An anti-M reacts strongly through all phases of testing. Which of the following techniques would not contribute to removing this reactivity so that more clinically significant antibodies may be revealed?
A. Acidifying the serum
B. Prewarmed technique
C. Adsorption with homozygous cells
D. Testing with enzyme-treated red cells
A. Acidifying the serum
Lowering the pH will actually enhance reactivity of anti-M. Prewarming (anti-M is a cold-reacting antibody), cold adsorption with homozygous M cells, and testing the serum with enzyme-treated red cells (destroys M antigens) are all techniques to remove reactivity of anti-M.
The reactivity of an unknown antibody could be anti-Jk^a, but the antibody identification panel does not fit this pattern conclusively. Which of the following would not be effective in determining if the specificity is anti-Jk^a?
A. Testing with enzyme-treated cells
B. Select panel of homozygous cells
C. Testing with AET-treated cells
D. Increased incubation time
C. Testing with AET-treated cells
AET denatures Kell antigens and has no effect on Kidd antibodies. Because the detection of Kidd antibodies is subject to dosage effect, selection of cells homozygous for the Jk a antigen (and longer incubation) would help to detect the presence of the corresponding antibody. Enzyme-treated red cells would also react more strongly in the presence of Kidd antibodies.
A col-reacting antibody is found in the serum of a recently transfused patient and is suspected to be anti-I. The antibody identification panel shows reactions with all cells at room temperature, including the autocontrol. The reaction strength varies from 2+ to 4+. What procedure would help to distinguish this antibody from other cold-reacting antibodies?
A. Autoadsorption technique
B. Neutralization using saliva
C. Autocontrol using ZZAP reagent-treated cells
D. Reaction with cord cells
D. Reaction with cord cells
Because RBCs contain variable amounts of I antigen, reactions with anti-I often vary in agglutination strength. However, because this patient was recently transfused, the variation in reaction strength may be the result of an antibody mixture. Although autoadsorption would remove anti-I, this procedure does not confirm the antibody specificity and can result in removal of other antibodies, as well. Cord cells express primarily i antigen with very little I antigen. Anti-I would react weakly or negatively with cord RBCs. ZZAP removes IgG antibodies from red cells. Because anti-I is IgM, the use of ZZAP would not be of value.
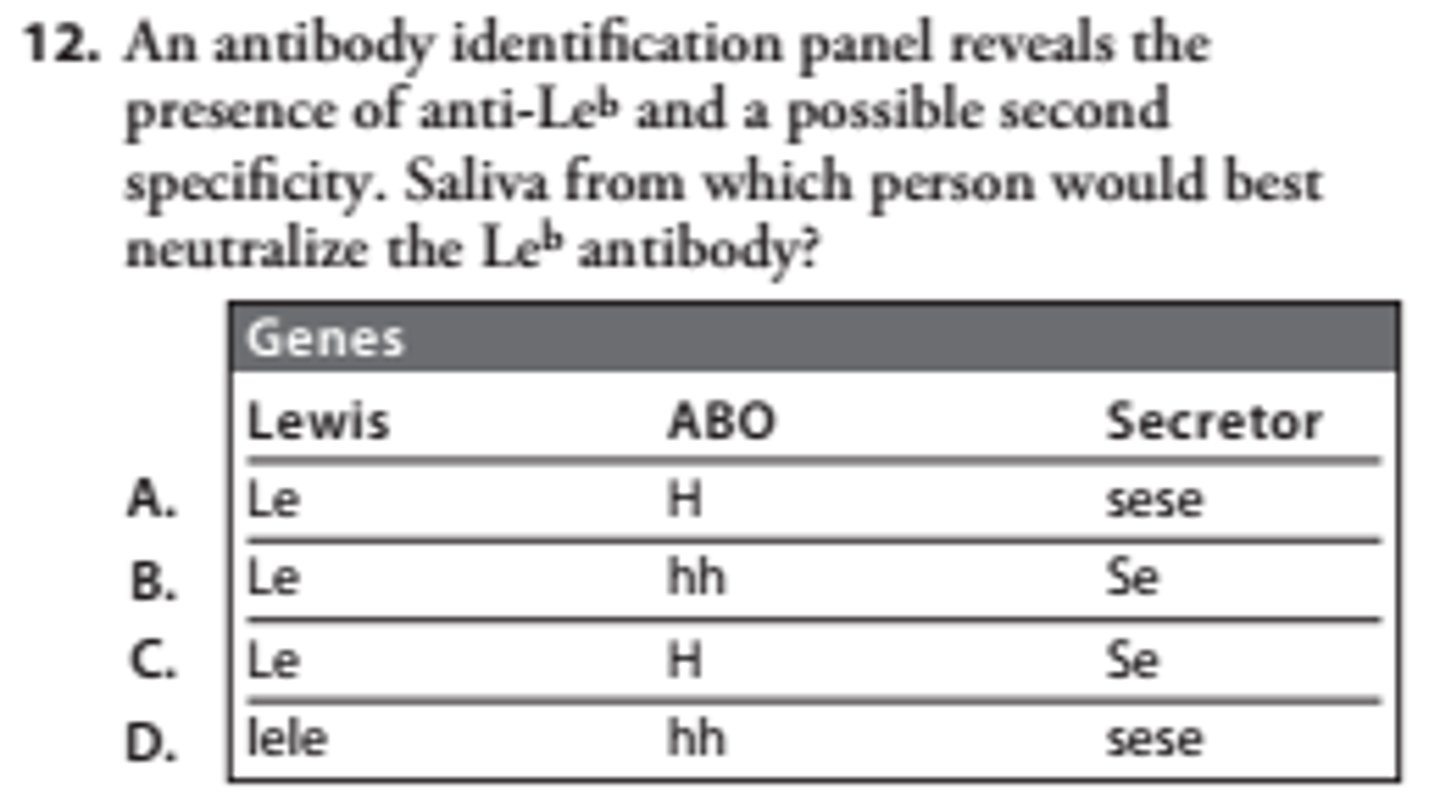
C
Lewis antibodies are usually not clinically significant but may interfere with testing for clinically significant antibodies. Lewis antibodies are most easily removed by neutralizing them with soluble Lewis substance. The Lewis antigens are secreted into saliva and plasma and are adsorbed onto the red cells. Le b substance is made by adding an L-fucose to both the terminal and next to last sugar residue on the type 1 precursor chain. This requires the Le, H, and Se genes. Since some examples of anti-Le b react only with group O or A2 RBCs, neutralization is best achieved if the saliva comes from a person who is group O.
A cord blood workup was ordered on Baby Boy Jones. The mother is O negative. Results on the baby are as follows:
Anti-A: 4+,
Anti-B: 0,
Anti-A, B: 4+,
Anti-D: 0,
DAT (poly): 2+
The test for weak D was positive at AHG. Is the mother an RhIg candidate?
A. No, the baby is Rh positive
B. Yes, the baby's Rh type cannot be determined due to the positive DAT
C. No, the baby is Rh negative
D. Yes, the mother is Rh negative
B. Yes, the baby's Rh type cannot be determined due to the positive DAT
The baby forward types as an A and the mother is O negative. It is possible that anti-A,B from the mother is attaching to the baby's red cells, causing a positive DAT. In the presence of a positive DAT, a weak test for D is not valid. Therefore, the baby's Rh type is unknown and the mother would be a candidate for RhIg.
Red cells from a recently transfused patient were DAT positive when tested with anti-IgG. Screen cells and a panel performed on a patient's serum showed very weak reactions with inconclusive results. What procedure could help to identify the antibody?
A. Elution followed by a panel on the eluate
B. Adsorption followed by a panel on the adsorbed serum
C. Enzyme panel
D. Antigen typing the patient's red cells
A. Elution followed by a panel on the eluate
If the red cells show a positive DAT, then IgG antibody has coated incompatible, antigen-positive red cells. If screening cells and panel cells show missing or weak reactions, most of the antibody is on the red cells and would need to be eluted before it can be detected. An elution procedure followed by a panel performed on the eluate would help to identify the antibody.
A patient types as O positive. All three screen and red cells from two O-positive donor units show agglutination after incubation at 37 degrees Celsius, and increase in reactivity at the IAT phase of testing. What action should be taken next?
A. Perform an autocontrol and direct antiglobulin test on the patient
B. Perform an enzyme panel
C. Perform an elution
D. Choose another 2 units and repeat the crossmatch
A. Perform an autocontrol and direct antiglobulin test on the patient
All screening cells and all units are positive at both 37°C and the IAT phase. This indicates the possibility of a high-frequency alloantibody or a warm autoantibody. An autocontrol would help to make this distinction. A positive autocontrol indicates an autoantibody is present; a negative autocontrol and positive screen cells indicates an alloantibody. A DAT would be performed to determine if an antibody has coated the patient's red cells, and is directed against screening cells and donor cells.
Four units of blood are ordered for a patient. Blood bank records are checked and indicate that 5 years ago this patient had an anti-Jk^b. What is the next course of action?
A. Antigen type units for the Jk^b antigen and only crossmatch units positive for Jk^b
B. Antigen type units for the Jk^b antigen and only crossmatch units negative for Jk^b
C. Randomly pull 4 units of blood that are ABO compatible and crossmatch
D. Perform an immediate spin crossmatch on 4 Jk^b-negative units
B. Antigen type units for the Jk^b antigen and only crossmatch units negative for Jk^b
A patient with a history of a significant antibody like anti-Jk b must receive blood that has been completely crossmatched and negative for the corresponding antigen; otherwise, an anamnestic reaction may occur with subsequent lysis of donor cells.
A 56-year-old patient diagnosed with colon cancer demonstrates a positive antibody screen in all three screen cells at the antiglobulin phase. A panel study is done and shows 10 cells positive as well as the autocontrol at the antiglobulin phase. The reactions varied from 1+ to 3+. This patient had a history of receiving 2 units of blood approximately 1 month ago. What should be done next?
A. Perform a DAT on the patient's cells
B. Perform an autoadsorption
C. Perform an alloadsorption
D. Issue O-negative cells
C. Perform an alloadsorption
In this situation, an allogeneic adsorption must be performed to adsorb out the autoantibody and leave potential alloantibodies in the patient's serum that will need to be identified before transfusion of blood to the patient. An autoadsorption cannot be performed due to the fact that any alloantibodies would be absorbed by circulating donor cells from a month prior.
A 33-year-old maternity patient is drawn for a type and screen at 36 weeks' gestation. The following results are found on the Ortho Provue:
Anti-A: 3+, Anti-B: 0, Anti-A, B: 4+, Anti-D: 4+, A1 cells: 2+, B cells: 4+, SCI: 0, SCII: 0, SCIII: 0, A1 lectin: 3+
The reference lab identified anti-P1 in the patient plasma using enzyme techniques. How could the ABO discrepancy be solved?
A. Wash the patient's red cells and repeat the forward grouping
B. Test the patient's plasma against A2 cells
C. Warm the patient plasma at 37 degrees Celsius for 10 minutes and repeat the reverse grouping
D. Treat the A1 cells with dithiothreitol and repeat the reverse grouping
C. Warm the patient plasma at 37 degrees Celsius for 10 minutes and repeat the reverse grouping
Anti-P1 is a cold-reacting antibody. Warming the plasma at 37°C will dissipate the antibody, preventing its reactivity with P1 antigen on the A1 cells.