Blood Bank Lecture 2 Fundamentals of Immunology
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
Primary lines of defense
Early evolutionary development
Non-specific
- Natural. Present at birth
- Immediately available
- May be physical, biochemical, mechanical, or a combination of defense mechanisms
Mechanism does not alter on repeated exposed to any specific antigen
Innate or Natural Immunity Comparison
Supplements protection provided by innate immunity
Later evolutionary development - seen only in vertebrates
Specific
- Specialized
- Acquired by contact with a specific foreign substance
- Initial contact with foreign substance triggers synthesis of specialized antibody proteins resulting in reactivity to that particular foreign substance
Memory
- Response improves with each successive encounter with the same pathogen
- Remembers the infectious agent and can prevent it from causing disease later
- Immunity to withstand and resist subsequent exposure to the same foreign substance is acquired
Acquired/Adaptive Immunity
Internal Components:
Physical
- Intact skin
- Mucous membranes
- Cilia
- Cough reflexes
Biochemical
- Secretions
- Sweat
- Tears
- Saliva
- Mucus
- Very low pH of vag and stomach
Innate or Natural Immunity First Line of Defense
Internal Components:
Cellular
- Phagocytic cells
- Macrophages-dendritic cells
- Monocytes
- PMNs Large granular leukocytes
- NK Cells
Humoral (Fluid) Biochemical
- Complement-alternate pathway
- Cytokines
- Interferons
- Interleukins
- Acute inflammatory reaction
Innate or Natural Immunity Second Line of Defense
Internal Components
Cellular
- Lymphocytes
- T cells
- TH
- TC
- T memory cells
- B Cells
- B memory cells
- Plasma cells
Humoral
- Antibodies
- Complement-classic pathways
- Cytokines
Acquired or Adaptive Immunity Third Line of Defense
Function of antibodies is to bind antigens
Binding is very specific: antibody reacts with only one epitope, or antigenic determinant, of an antigen
Binding inactivates the antigen and activates effector mechanisms that ultimately lead to the destruction of the antigen and the cell to which it is bound
Humoral Immunity
The laboratory study of antigen-antibody reactions - the basis of routine blood bank testing
Serology
Lag phase of 5-10 days, influence by the characteristics of the antigen and hosts immune system
IgM is produced first, IgG seen later
Primary immune response
Can detect antibodies within 1-3 days of exposure
Much higher concentration of antibodies that persist longer
Primary antibody is IgG
Secondary (anamnestic) immune response
Gamma (IgG)
Alpha (IgA)
Mu (IgM)
Delta (IgD)
Epsilon (IgE)
Heavy Chains
Kappa
Lambda
Light Chains
Constant and variable regions
Papain and pepsin digestion
Disulfide bonds
Fc fragments binds complement or Fc receptors on other
Fab region binds antigen
IgM and IgA can exist in monomeric or polymeric
IgM as pentamer
IgA as dimer or trimer
IgG only exists in monomeric form
Characteristics of Immunoglobulins
IgG and IgM are the most significant for blood banking
Most clinically significant antibodies that react at body temperature are IgG
IgM antibodies are commonly encounter as naturally occurring antibodies and usually react best at room temperatures or colder
Immunoglobulins significant for blood banking
Heavy chain composition - Mu
Light chain composition - Kappa or Lambda
J Chain - Yes
Molecular Weight - 900,000
Valence - 10
Total serum concentration - 10
Serum half-life in days - 5
Crosses the placenta - No
Activation of classical pathways of complement - Yes; very efficient
Clearance of red cells - Intravascular
Detection in laboratory tests - Immediate spin
IgM
Heavy chain composition - Gamma
Light chain composition - Kappa or Lambda
J Chain - No
Molecular Weight - 150,000
Valence - 2
Total serum concentration - 70-75
Serum half-life in days - 23
Crosses the placenta - Yes
Activation of classical pathways of complement - Yes; not as efficient
Clearance of red cells - Extravascular
Detection in laboratory tests - Antiglobulin test
IgG
Activation when antibody (IgM, IgG1, or IgG3) binds to antigen
- Activation by IgG requires many IgG molecules
- Activation by IgM requires only 1 IgM molecule
Majority of blood group antibodies do not activate complement at body temperature
ABO antibodies DO bind complement and induce intravascular hemolysis
Classical Complement Pathway
Activation occurs by surface contacts with complex molecules and artificial substances with repeating units
Allows complement to be activated without acquired immunity
Alternative complement pathway
Activation occurs when mannose-binding lectins (MBL) bind to microbes and then follows classical pathway
Lectin complement pathway
Though majority of blood group antibodies do not activate the classical complement pathway and result in intravascular hemolysis, clinically significant blood group antibodies can result in extravascular hemolysis via reticuloendothelial (mononuclear phagocytic) system and other anaphylatoxic effects
Complement System
Antigens are large molecular weight proteins and polysaccharides that may initiate formation of and react with antibodies
Can be located on the surfaces of cell membranes or as an integral portion of the cell membrane
Characteristics of antigen
Degree to which an antigen is capable of eliciting an immune response
Immunogenicity
Size
Complexity
Conformation
Charge
Accessibility
Solubility
Digestibility
Chemical composition
Antigen characteristics influencing their immunogenicity
Blood group antigens differ in their immunogenicity
Transfused red cells express antigens that may be recognized as foreign to the patient
The exposure to these foreign antigens may cause an immunogenic response resulting in production of corresponding antibodies
RBC antigens
Blood group antibodies are present in a patients serum/plasma
Polyclonal or monoclonal
Naturally occurring or immune
Alloantibodies or autoantibodies
Characteristics of blood group antigens
Secreted by different B cell lineages
They are a collection of immunoglobulin molecules that react against a specific antigen, each identifying a different epitope
Polyclonal antibodies
Made by identical B cells that are all clones of a unique parent cell using hybridoma technology
They have monovalent affinity, in that they bind to the same epitope
Monoclonal antibodies
Which of the following would likely be more optimal for laboratory testing
Polyclonal antisera
Monoclonal antisera
Monoclonal antisera
Produced without transfusion, injection, or pregnancy
IgM, RT or lower, activate complement, may be hemolytic at 37C
Visible agglutination in saline
ABO, Hh, Ii, Lewis, MN, P
Naturally occuring antibodiesA
Acquired through transfusion or pregnancy
IgG, 37C
Require AHG testing for detection
Rh, Kell, Duffy, Kidd, Ss
Immune antibodies
A red cell antibody is considered clinically significant if it can cause accelerated destruction of transfused donor red cells. Which of the following is FALSE concerning clinically significant red cell antibodies
Most clinically significant antibodies are IgM
Directed at non-self antigens after exposure/transfusion
Alloantibodies
Directed at self-antigens
Can have a specificity common to transfused blood or no detectable specificity
Autoantibodies
Most clinically significant antibodies react at body temp 37C, are IgG, and can cause immune destruction of transfused red cells possessing the antigen
IgG can cross the placenta, weakly cause complement fixation, and mark red cells for phagocytosis
The destruction of red cells can cause transfusion reactions, anemia, and Hemolytic Disease of the Fetus and Newborn (HDFN)
IgM antibodies react best at room temp 20-22C or lower and are usually not implicated in the destruction of transfused red cells (they are usually not clinically significant)
The antibodies to ABO antigens are an important EXCEPTION to this generalization
A transfusion of the wrong ABO group antigens would effectively activate the classical complement system, initiate intravascular hemolysis of the transfused cells, and cause a severe hemolytic transfusion reaction
RBC antibodies
Antigen-Antibody ratio
pH
Temperature
Immunoglobulin type
Incubation time
Ionic strength
Distance between cells
Factors that influence antigen-antibody reactions
Detection of blood group antibodies depends on characteristics of antigen-antibody reactions
These reactions depend upon binding forces between antigens and antibodies, properties of the antibody itself, and individual host characteristics
Antigen-antibody reactions
Can occur in vivo or in vitro
The binding of an antigen and antibody is a reversible process
When the immune complex has been generated, non-covalent attractive forces, including electrostatic forces (ionic bonding), hydrogen bonding, hydrophobic bonding, and van der Waals forces hold the complex together
Intermolecular binding forces
Strength of a single antigen-antibody bond
Affinity
A measure of functional affinity
Avidity
Specific reaction, cross-reaction, no reaction
Specificity
Number of antigen/antibody binding sites
Valency
Antigen-antibody reactions in vitro are detected by visible agglutination of red cells or evidence of hemolysis at the end of the testing
No agglutination means no reaction
Two stages of hemagglutination reaction
Sensitization: Binding of antibody and antigen
Lattice Formation: Cross-linking of antibody-coated RBCs resulting in visible agglutination of cells
Hemagglutination
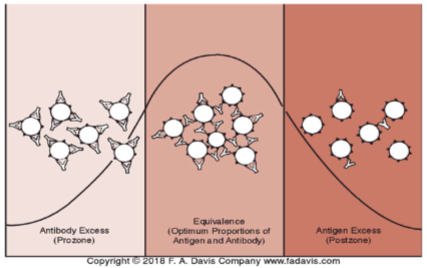
The probability of antigen-antibody interaction relies upon the effect of the ratio of the antibody & antigen concentrations
Antigen-antibody ratio
Postzone effect in an antigen-antibody reaction would likely result in a
False-negative result
Recall heterozygous genotypes can lead to weaker phenotype expression, less antigen being present on RBCs can lead to weaker antigen-antibody reactions
Test system can be manipulated in the lab to overcome the effects of excessive antigen or antibody
Dosage effect
Antigen-antibody ratio
Dosage effect
pH
Temperature
Incubation Time
Ionic Strength
Factors that influence sensitization
Optimal is 7.0
pH
Generally acts by increasing reaction rate, but different Ig isotypes also have different optimal reactivity temperatures
IgM: immediate spin phase at room temperature
IgG: Antihuman globulin (AHG) phase with 37C incubation
Temperature
Allowing adequate time to attain equilibrium; varies by test procedure
Incubation time
Na+ and Cl- ions in isotonic environment (saline) are attracted to oppositely charged groups on antigen/antibodies, hindering their interaction with each other; lowering increases antibody uptake
Ionic strength
Distance between cells
Zeta potential
Centrifugation
Zone of equivalence
Factors influencing lattice formation
Red cells possess a net negative charge on the cell surface in a saline suspension
Cations from the saline environment are attracted to those negative charges and form a stable cationic cloud around each cell, resulting in a force of repulsion between any similarly charged molecules
Because of this, the red cells remain at a distance from each other, proportional to the zeta potential
IgM is larger and has pentameter shape with multivalent properties; thus agglutination can be seen without enhancement media
IgG is smaller and cannot always overcome the zeta potential but enhancement media can help form macroscopically visible agglutination
Zeta potential
Helps facilitate lattice formation by forcing the red cells closer together in the test environment
Centrifuges are calibrated to the optimal speed and time for the best visible reaction (may vary by test)
Centrifugation
Again, optimal antibody to antigen ratio is very important for both stages of agglutination
Washing is another procedural step to remove unbound antibody that we do not want to detect
Zone of equivalence
What can enhance hemagglutination reactions
Increasing the incubation time
To help us detect IgG in our patients, we use potentiators or enhancement media to enhance the reactivity of IgG
Most enhancement media works to reduce the zeta potential and allow the more positively charged antibodies to get closer to the negatively charged red cells
Factors influencing agglutination
Low Ionic Strength Solution
Polyethylene Glycol (PEG)
Proteolytic Enzymes
Antihuman Globulin (AHG)
Potentiators
Decreases the ionic strength of test system
Reduces zeta potential
Increases antibody uptake during the sensitization stage and helps lower the needed incubation time
Low Ionic Strength Solution LISS
Concentrates test system by removing water molecules
Brings sensitized red cells closer together, helping to form those crosslinks for lattice formation
Is considered to be more effective than albumin and LISS for detection of weak antibodies
Polyethylene Glycol (PEG)
Ficin, Papain, Trypsin, Bromelin
Modifies various blood group antigens, which can be especially useful when IDing multiple antibodies
ENHANCES reactivity of Rh, Kidd, P1, Lewis, and I blood group antigens by removing hydrophilic glycoproteins from RBC membrane
DESTROYS reactivity of Fya, Fyb, M, N, and S blood group antigens
Proteolytic Enzymes
Reveals if red cells are coated with antibody and/or complement proteins
If the antibodies present in serum/plasma do not cause red cell agglutination but only sensitize (bind) them, AHG reagent allows for visible agglutination to occur by cross-linking the antibodies coating the RBCs
Antihuman Globulin (AHG)
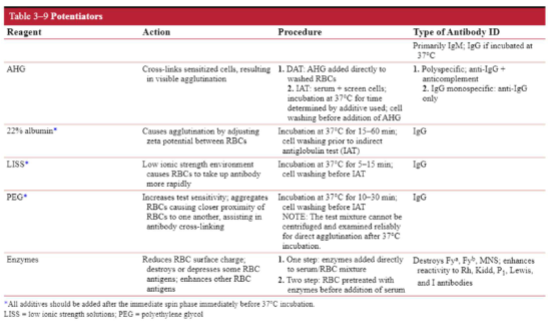
Potentiators Chart
In routine blood banking, red cell agglutination is graded qualitatively
Testing can be performed in test tubes, microplate wells, or in microtubes filled with gel particles
Defined grading system in place to help standardize the subjectivity uses a 0 to 4+ scale
ANY Agglutination or hemolysis in the supernatant is considered a positive result
Grading hemagglutination
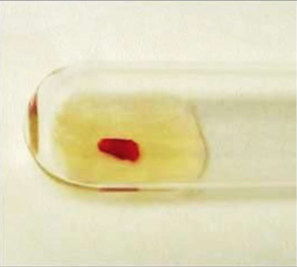
4+ reaction

3+ reaction

2+ reaction

1+ reaction

Hemolysis
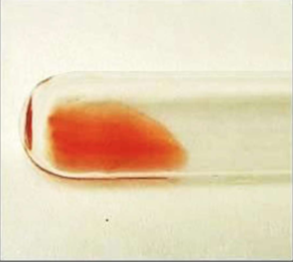
Negative reaction