2- benign tumors of the jaw
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
84 Terms
benign tumors are usually what shape
round/oval
benign tumors usually have what kind of periphery/margins
Well-defined
▪ Smooth, regular
▪ Mostly corticated
benign tumors usually have what kind of density + internal architecture
Radiolucent or mixed
▪ radiopaque flecks seen in mixed
lesions
▪ Septations, loculations
(multilocular lesions)
benign tumors usually have what kind of effect on surrounding structures
expansion + thinning of cortical bone, erosion (aggressive benign lesions)
displacement of max sinus floor, IAN canal, teeth w/ external root resorption
3 types of odontogenic tumors
epithelial
ectomesenchymal
mixed
3 types of epithelial odontogenic tumors
ameloblastoma
adenomatoid odontogenic
calcifying epithelial odontogenic
what’s the most common epithelial odontogenic tumor
ameloblastomas (2nd most common odontogenic tumor overall)
3 patterns of ameloblastomas
conventional (75-86%)
unicystic (13-21%)
peripheral (1-4%)
ameloblastomas affect max or mand more
mand, usually in molar region
T/F: ameloblastomas are painful
false, often painless
radiographic features of ameloblastomas
well circumscribed/corticated
radiloucent
unilocular/multilocular (course + curved septae if multi)
may arise in cyst wall

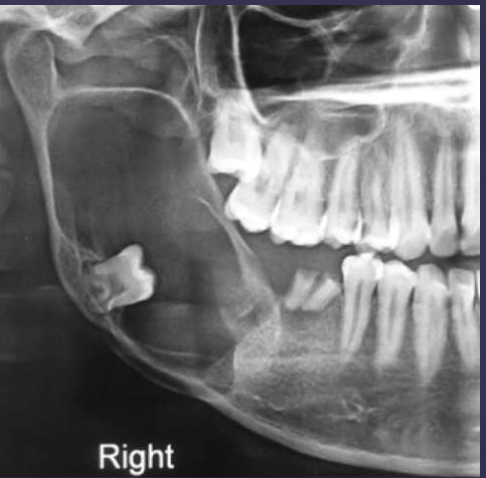
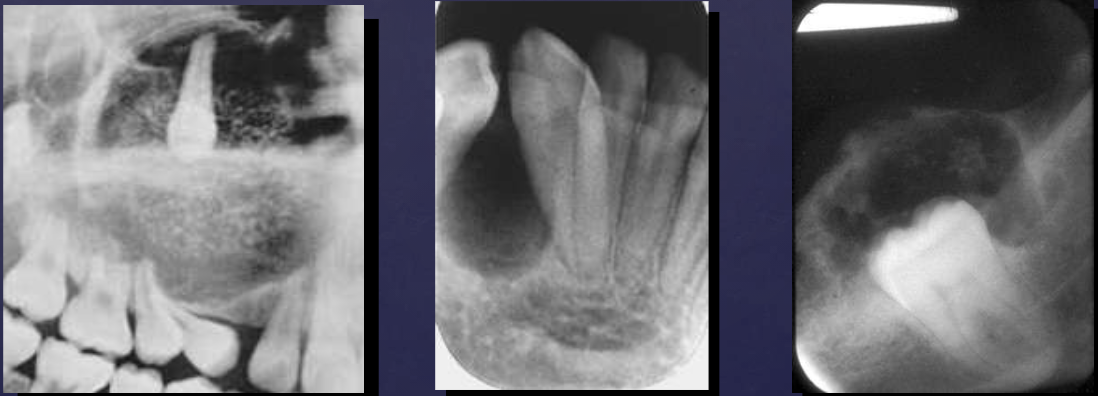
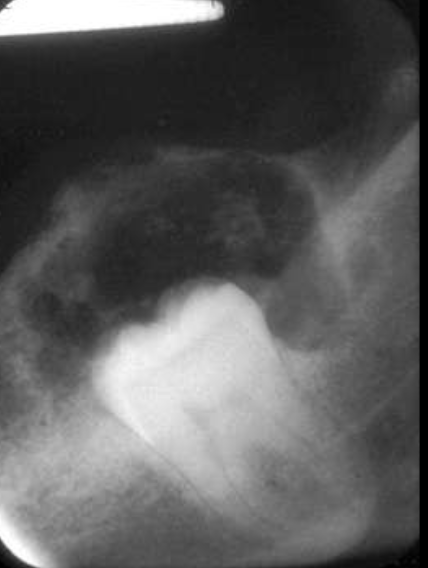
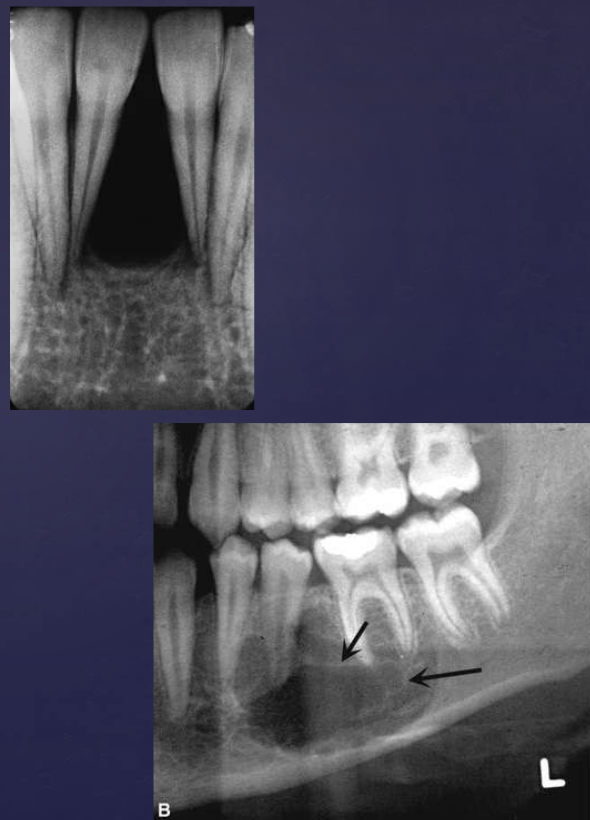
describe what’s occurring in this radiograph
pericoronal/mural; impacted tooth
displacement of #32 + IAN
osseous expansion
thinning of cortices

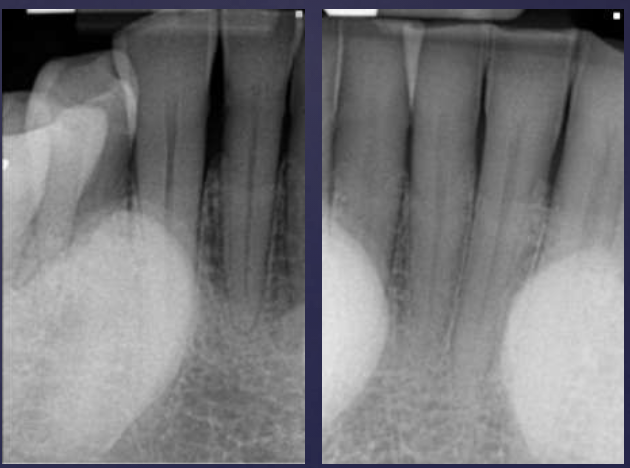
describe the ameloblastoma in this radiograph
multilocular w/ coarse septae
thinning of inferior mand border
displacement of teeth + IAN
follicular pattern hisopath features of ameloblastomas
nests of epithelium
island centers resembling stellate reticulum
peripheral columnar cells with nuclei polarized opposite basement membrane (sub-nuclear vacuolization)
mature fibrous background
desmoplastic pattern hisopath features of ameloblastomas
compressed islands + cords of odontogenic epithelium in densely collagenized stroma, presents in anterior max
2 tx options for ameloblastomas
simple enucleation (recurrence rate = 50-90%)
en bloc resection (recurrence rate = 15%)
unicystic ameloblastomas affects which age mostly
50% diagnosed between ages 10-20, associated w/ impacted 3rd molars

unicystic ameloblastomas often mimics what
dentigerous cyst
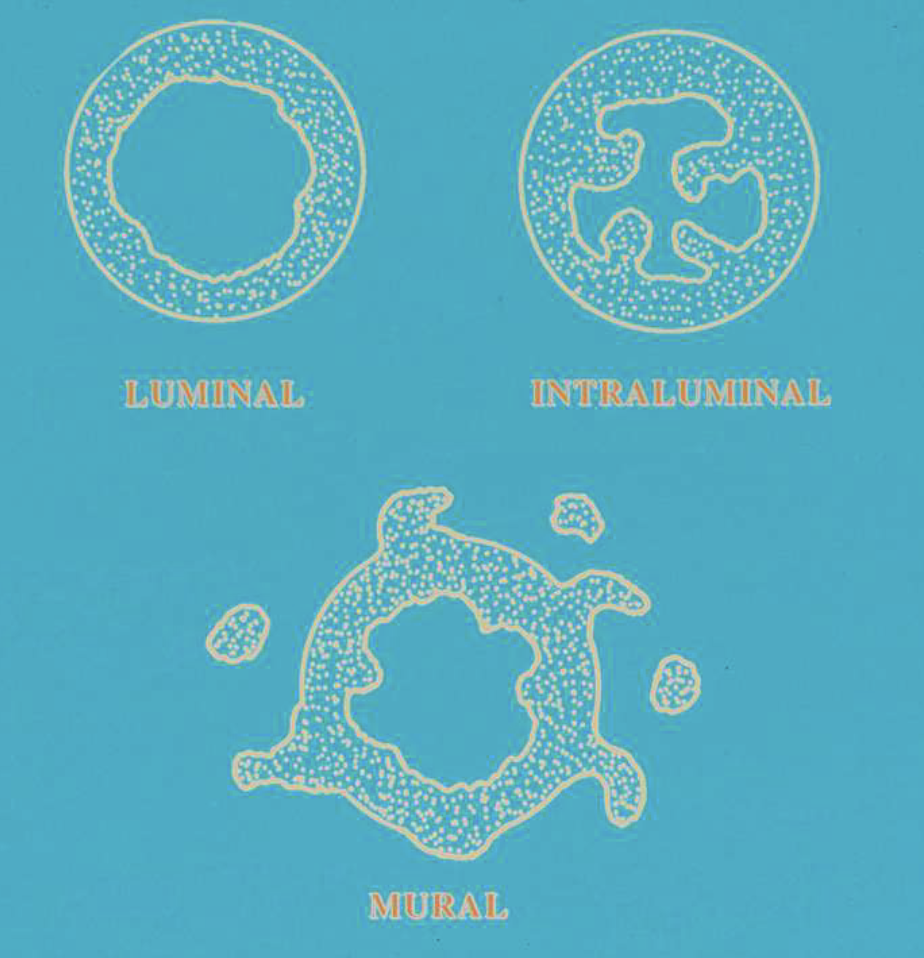
3 histopath types of unicystic ameloblastomas
luminal: confined to luminal surface
intraluminal: tumor nodules project from lining into lumen
mural: tumor islands in wall of cyst
tx options for unicystic ameloblastomas
luminal + intraluminal types treated w/ enucleation
mural type tx debatable
recurrence = 10-20%
T/F: peripheral ameloblastomas are soft tissue lesions only
true

peripheral ameloblastomas affects max or mand more
mand
peripheral ameloblastomas affect which age group
average age = 52
histopath features of peripheral ameloblastomas
epithelial islands beneath surface epithelium
plexiform and follicular patterns most common
50% show connection to basal layer of surface epithelium
tx options for peripheral ameloblastomas
local excision w/ 15-20% reoccurrence
adenomatoid odontogenic tumors affect which age group
70% 10-20 years
adenomatoid odontogenic tumors commonly affect what area
max anterior
adenomatoid odontogenic tumors affect which gender more
women
radiographic features of adenomatoid odontogenic tumors
associated w/ unerupted tooth (commonly max lateral incisor)
mixed radiodensity: mostly radiolucent w/ some radiopacity within
displacement of adjacent teeth

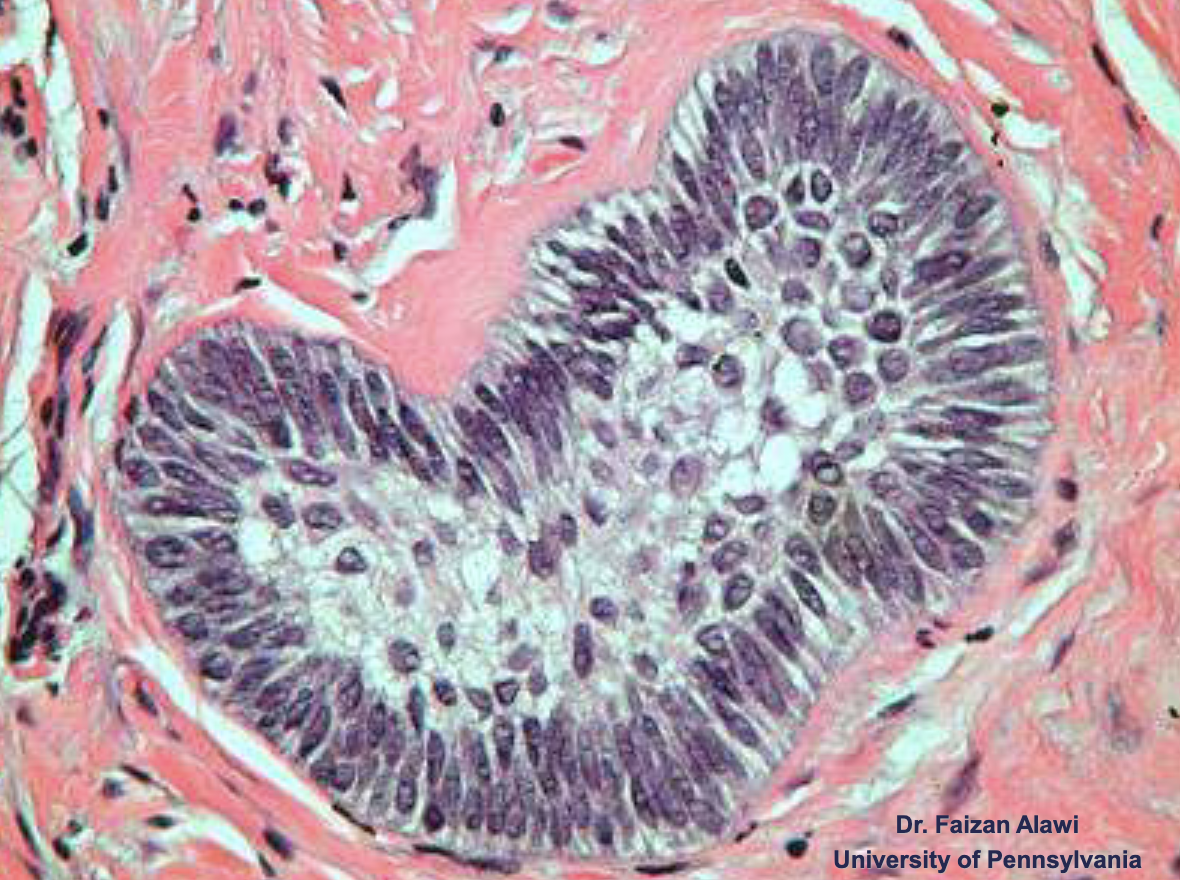
histopath features of adenomatoid odontogenic tumors
well-defined lesion surrounded by thick fibroud capsule
tubular or duct-like structures
tx options for adenomatoid odontogenic tumors
enucleation
which type of epithelial odontogenic tumor is the most rare
calcifying epithelial odontogenic (Pindborg) tumors
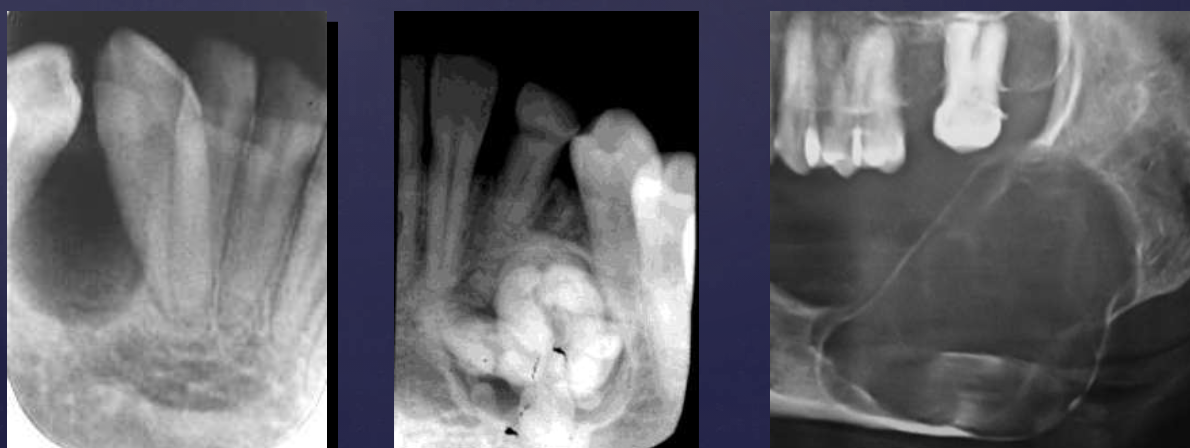
radiographic features of calcifying epithelial odontogenic (Pindborg) tumors
mixed density- central radiolucency with radiopaque foci
maybe associated w/ unerupted tooth
expansile- expands cortex
root resorption possible

T/F: you can see B/L expansion in this radiograph
false, since this PAN is a superimposed image- you cannot tell
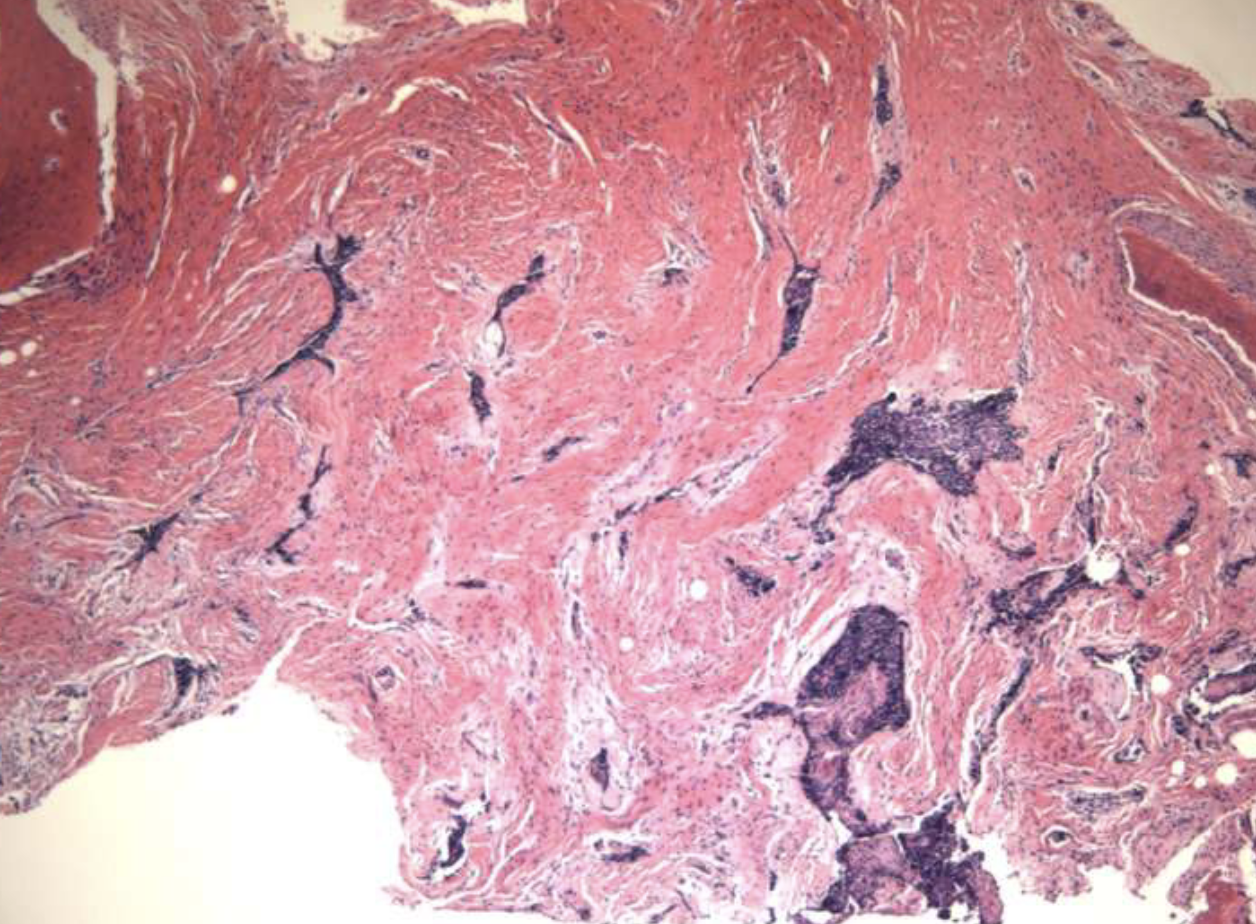
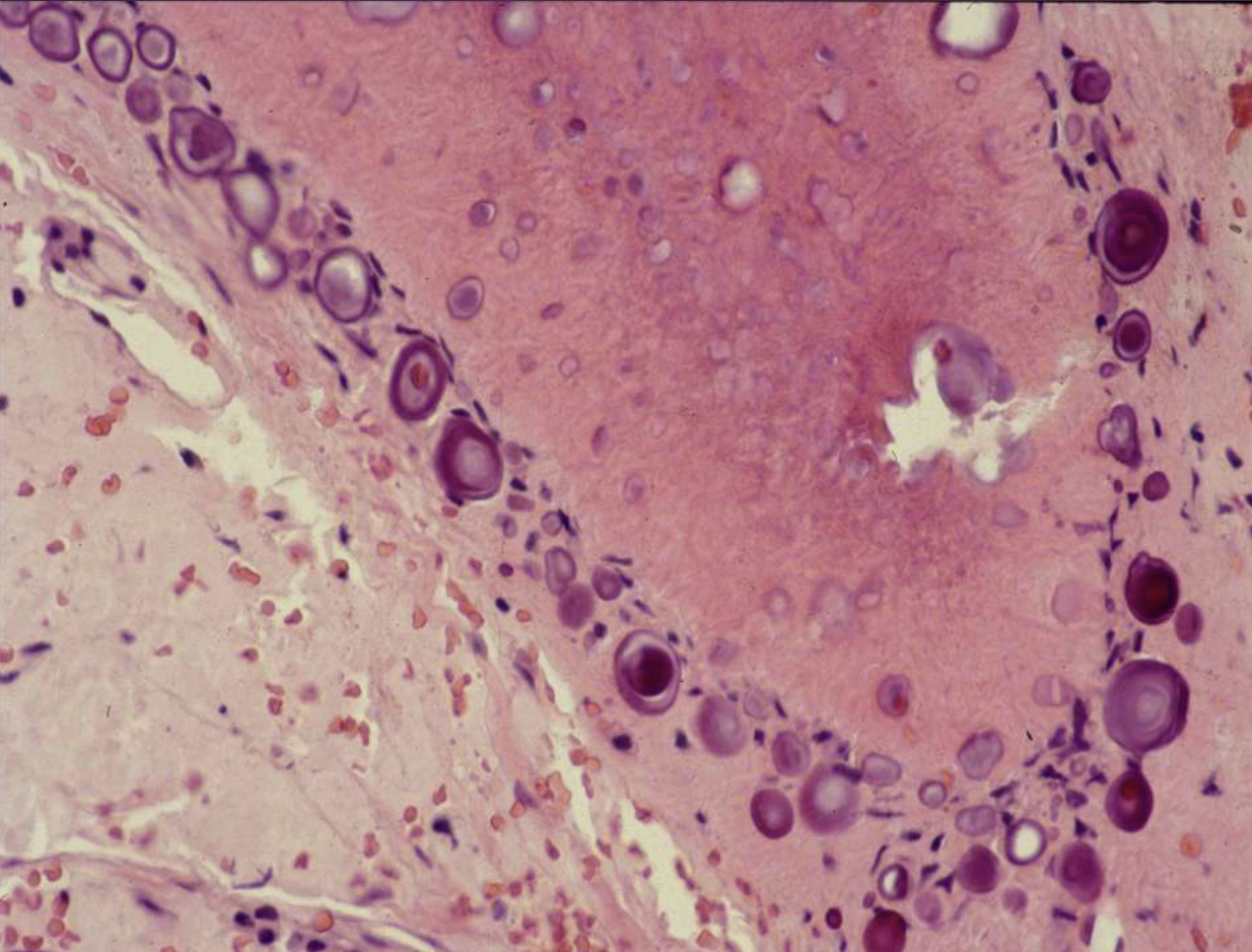
histopath features of calcifying epithelial odontogenic (Pindborg) tumors
islands, strands, or sheets of epithelial cells in fibrous stroma
Liesegang rings
tx options for calcifying epithelial odontogenic (Pindborg) tumors
conservative resection
2 types of ectomesenchymal odontogenic tumors
odontogenic myxoma
cementoblastoma
odontogenic myxomas usually affects which age
25-30
T/F: odontogenic myxomas are painless
true, small lesions are symptomatic + larger lesions are painless swelling
radiographic features of odontogenic myxomas
variable margins: well or poor defined
radiolucent
straight + thin septae

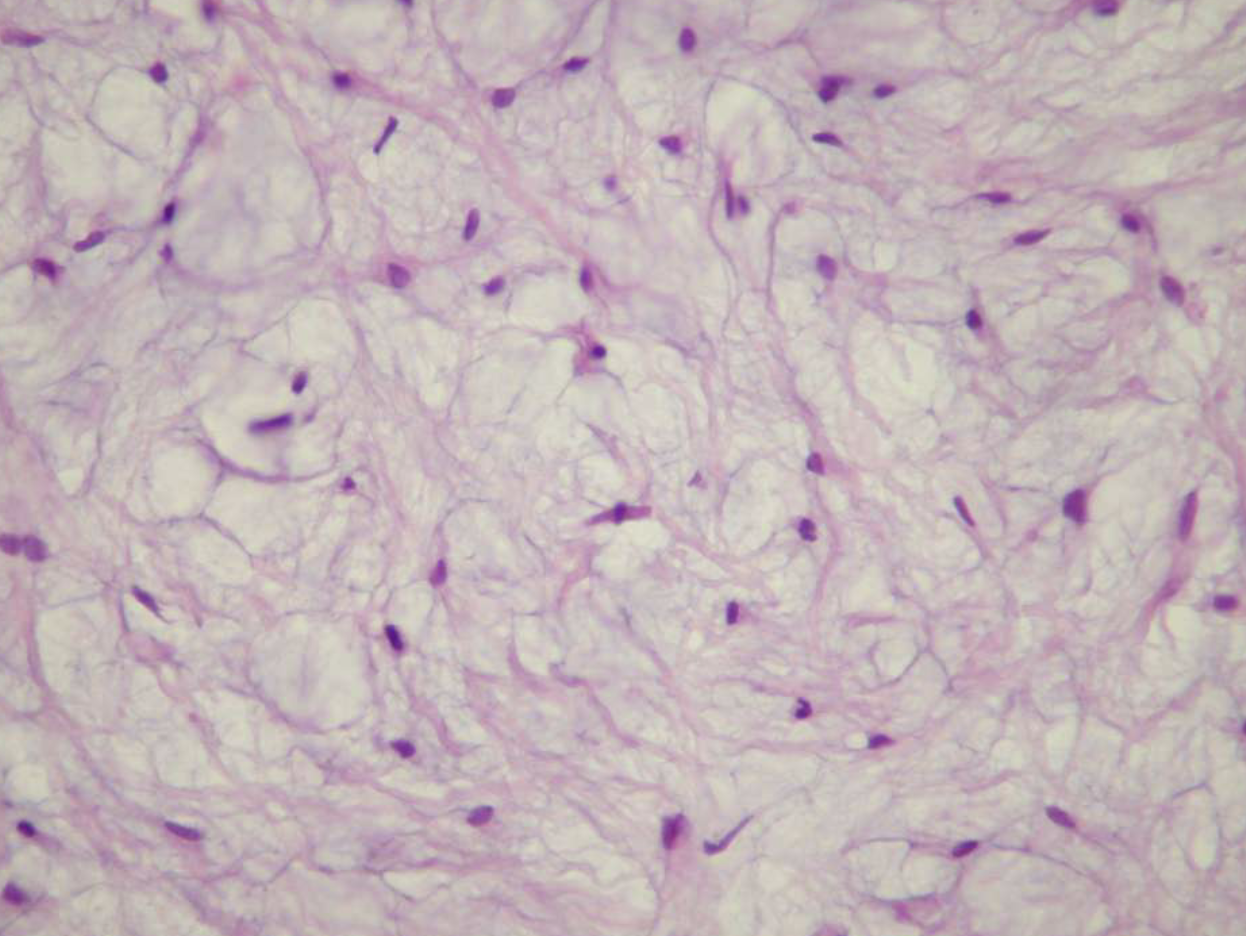
histopath features of odontogenic myxomas
loose stroma w/ collagen fibrils
haphazardly arranged stellate, spindle-shaped, round cells
tx options for odontogenic myxomas
small lesions are curetted
large lesions are resected
25% recurrence + egg-white consistency makes complete removal difficult
cementoblastomas usually affect which age
pts younger than 20
T/F: cementoblastomas are painless
false, 67% report pain + swelling
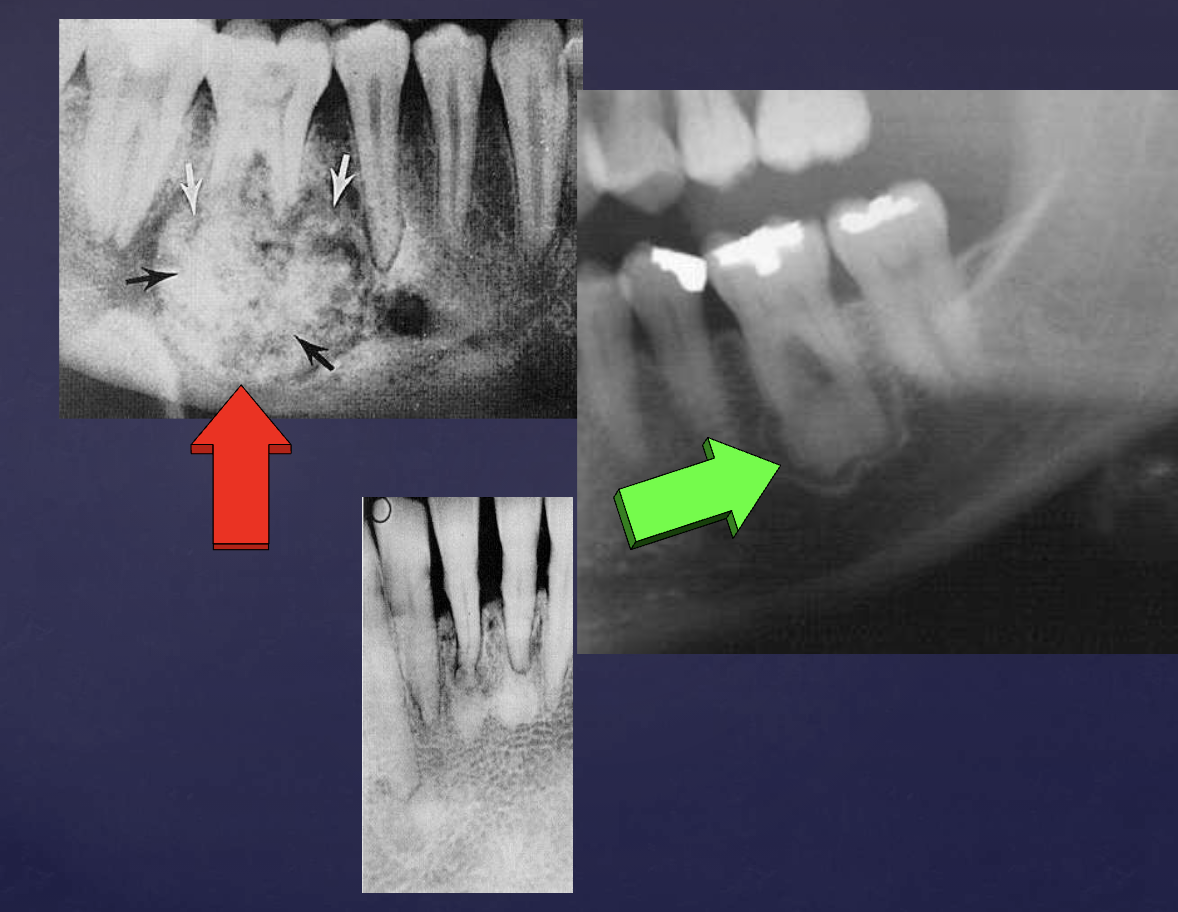
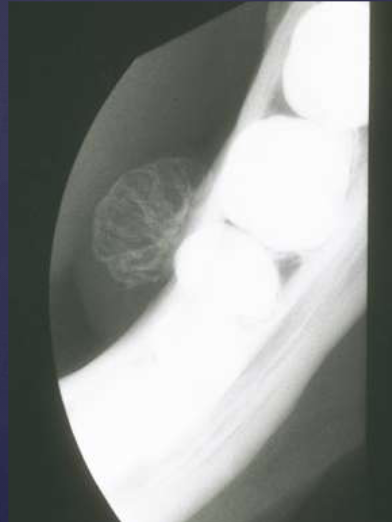
radiographic features of cementoblastomas
multiple punctate radiopacities within a well-defined radiolucency
homogeneous radiopaque mass
mass attached to 1st mandibular molar roots
obscured root outline, external resorption
radiolucent halo - continuity w/ PDL
sclerotic border
differentiate cementoblastomas vs. hypercementosis
cementoblastomas: globular
hypercementosis: bulbous, more tooth-shaped
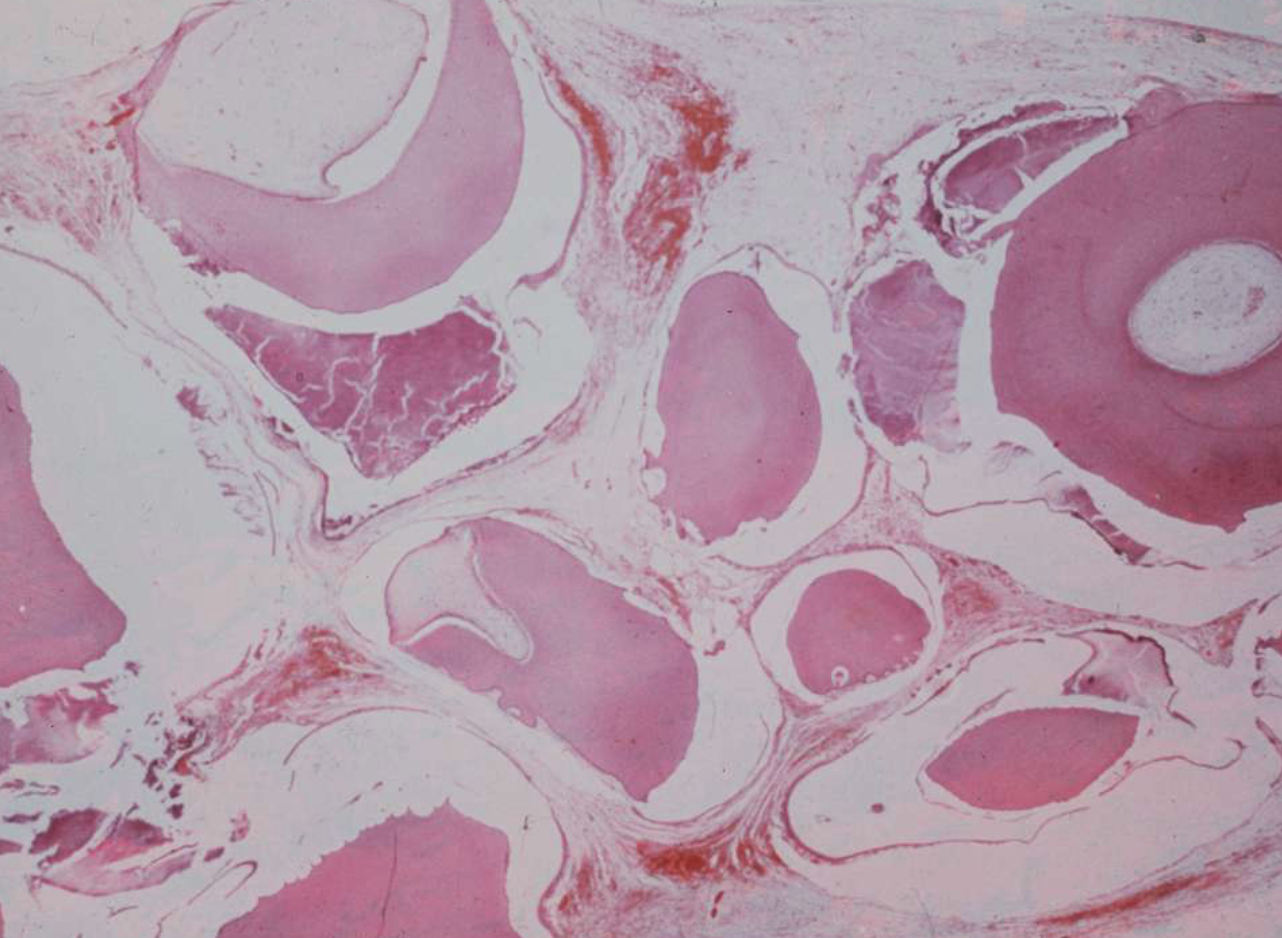
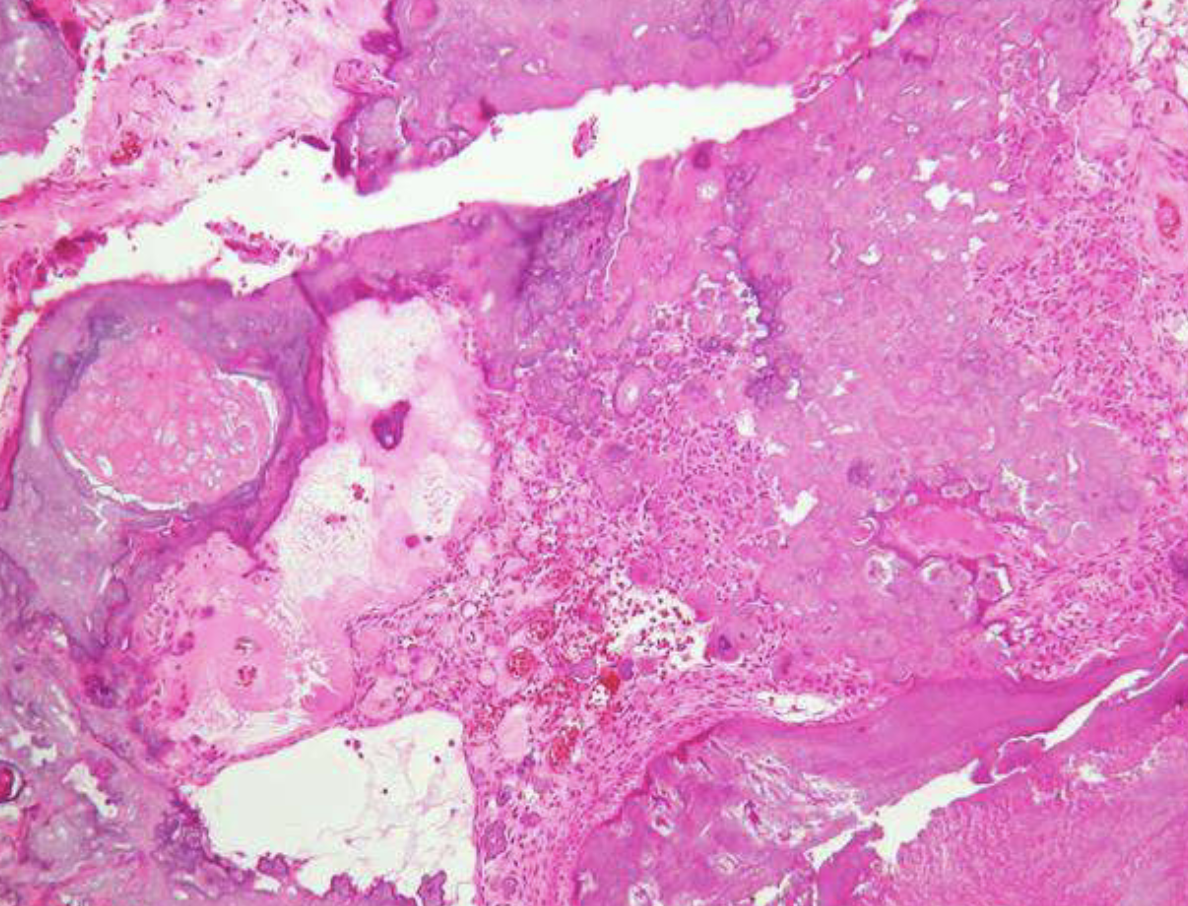
histopath features of cementoblastomas
trabeulae lined w/ plump cementoblasts
vascular CT

tx options for cementoblastomas
EXT of tooth w/ calcified mass
excision of mass w/ root amputation + endo tx
what’s the #1 most common odontogenic tumor/hamartoma
odontoma (74% of odontogenic tumors in US)
odontomas are made of
enamel, dentin, pulp, and/or cementum
3 types of odontomas
compound
complex
compound-complex
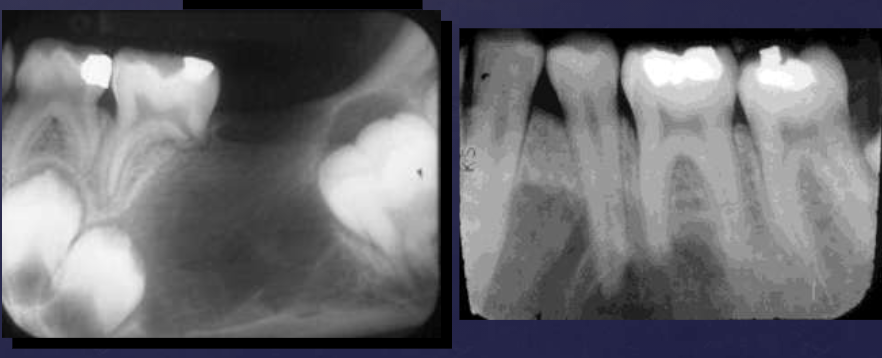
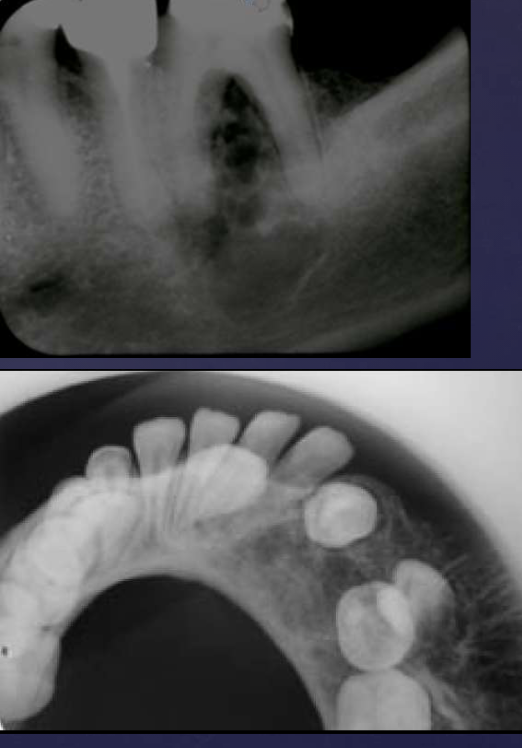
radiographic features of compound odontomas
radiolucent band/soft tissue capsule inside the cortical border
internal content is largely radiopaque: made of tooth-like structures called denticles
maybe associated w/ unerupted tooth

radiographic features of complex odontomas
radiolucent band/soft tissue capsule inside the cortical border
internal content is largely radiopaque- made of irregular mass of calcified tissue

radiographic features of compound-complex odontomas
mixed density, corticated
combination of amorphous radiopaque mass + tooth-like structures

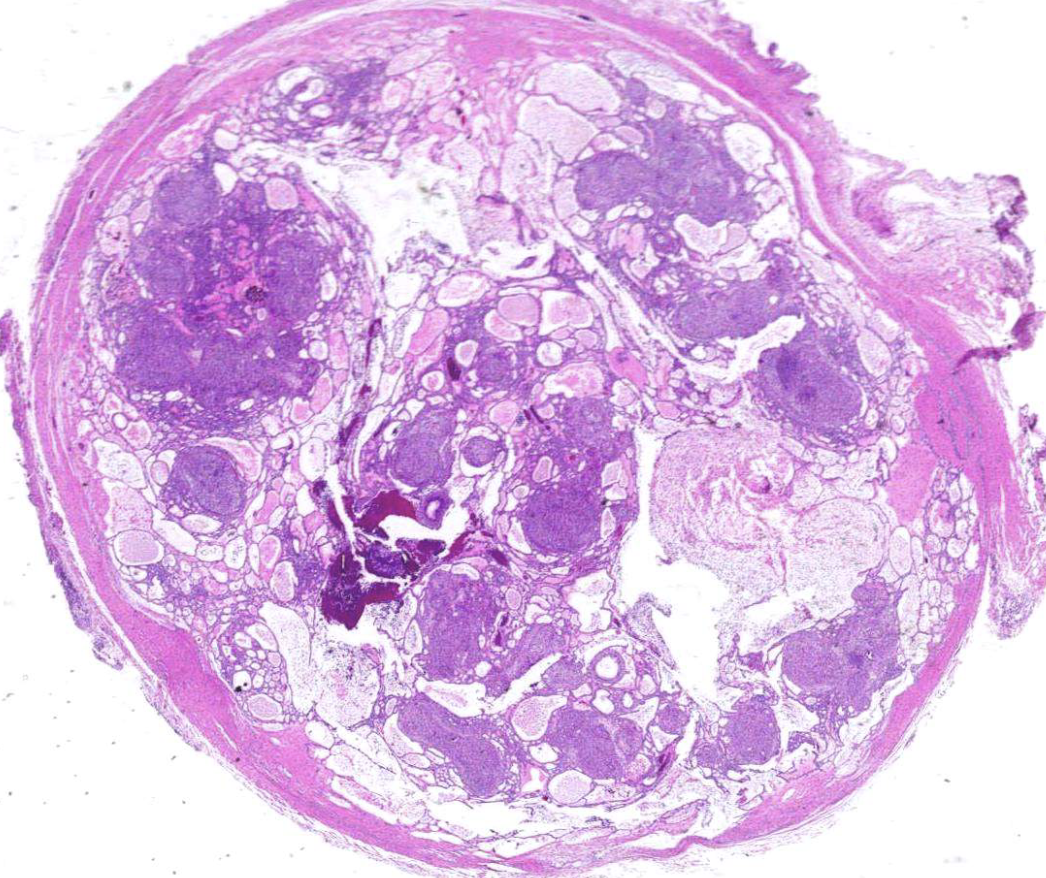
histopath features of compound odontomas
multiple structures resemble small teeth in loose fibrous matrix
histopath features of complex odontomas
mature tubular dentin with structures that contained enamel before decalcification
20% show ghost cells
thin layer of cementum around mass
tx options for odontomas
conservative enucleation
4 types of non-odontogenic tumors
osteoma
neurofibroma
vascular malformation (hemangioma)
giant cell lesions
radiographic features of osteomas
internal structure- uniformly radiopaque or internal trabecular structure
maybe be exophytic (projects outward), extending into adjacent soft tissues

why is the osteoma radiolucent
b/c it’s affecting more cancellous bone
T/F: osteomas only affect cancellous bone
false, can affect cortical bone too
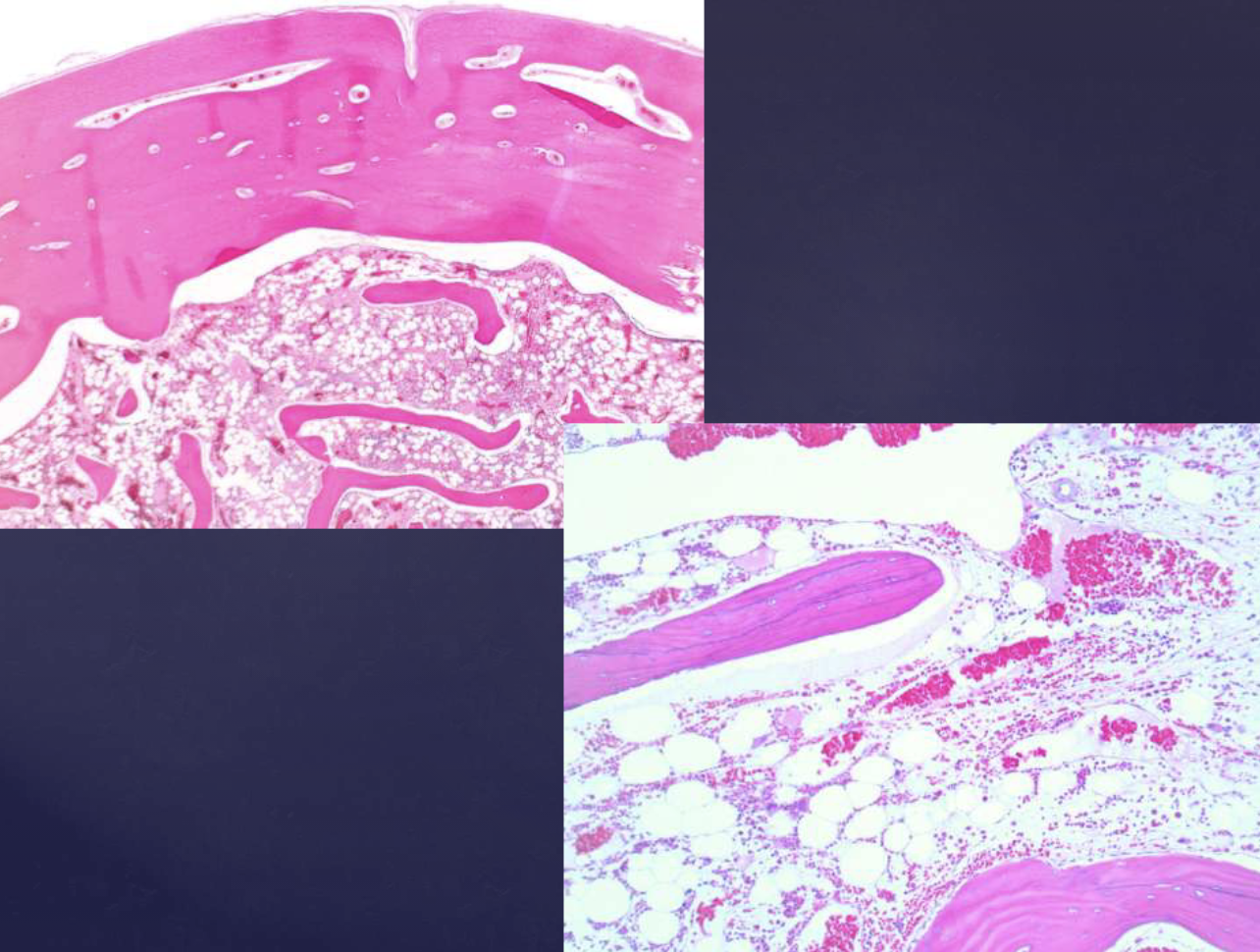
histopath features of osteomas
compact lamellar bone w/ fibrofatty marrow, similar to tori + exostoses
syndrome associated w/ osteomas
Gardner’s syndrome: multiple osteomas + unerupted supernumerary/permanent teeth

Gardner’s syndrome has potential of malignancy for what
polyps in GI tract
radiographic features of neurofibromas
radiolucent
unilocular/multilocular
fusiform enlargement of the neurovascular canal

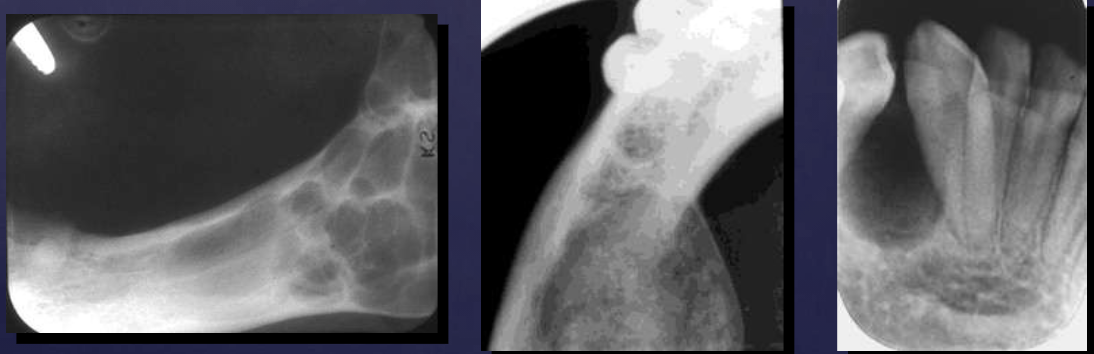
radiographic features of central vascular malformations (hemangiomas)
well defined, corticated or ill defined periphery possible
radiolucent
periosteal rxn (sunray-like appearance)
maybe multilocular
honeycomb pattern
displacement of teeth/root resorption
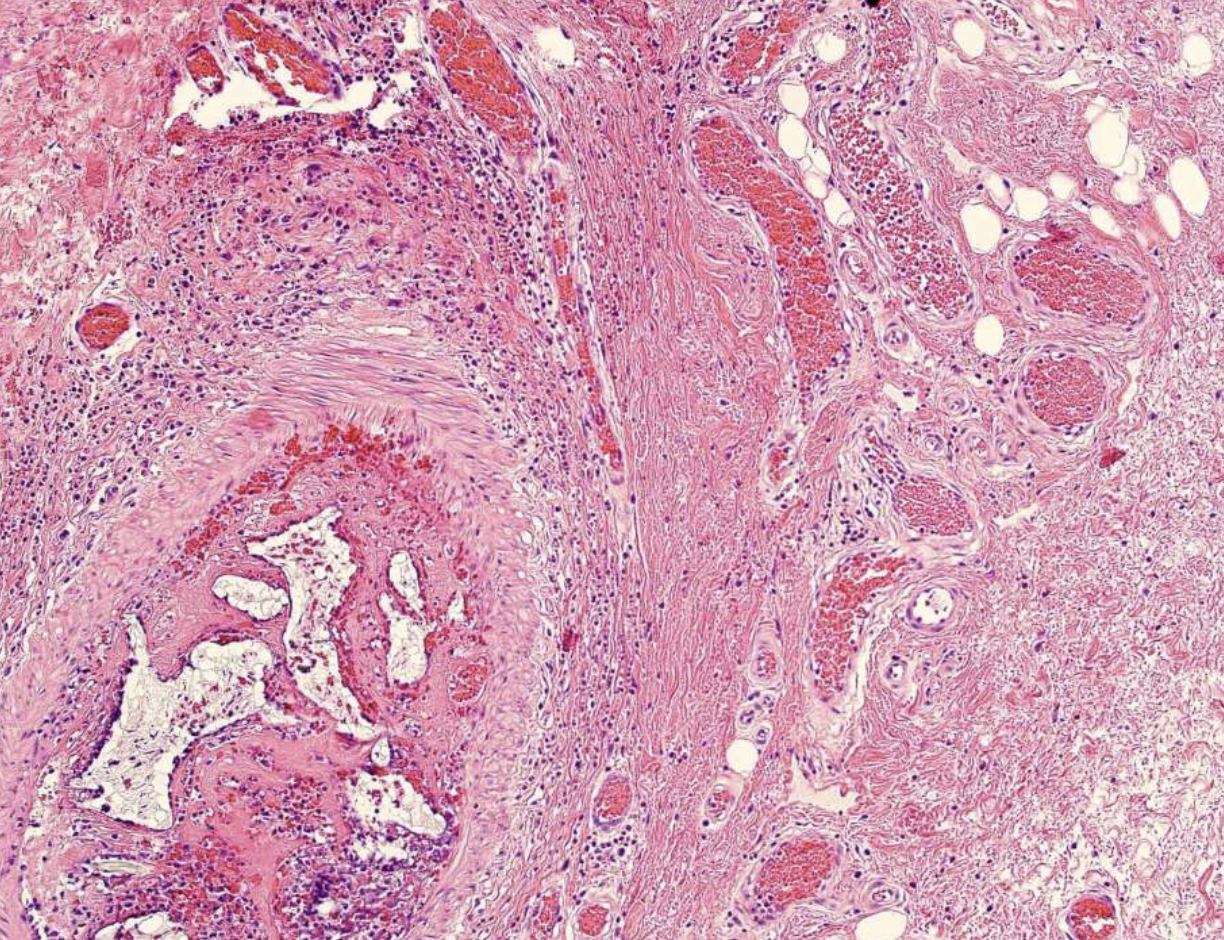
histopath features of central vascular malformations (hemangiomas)
proliferation of capillaries + endothelial cells containing abundant blood
2 types of bone hyperplasias
exostosis/tori: surface growth
enostosis (dense bone island): internal growth
2 types of exostosis/tori
torus palatinus
torus mandibularis
radiographic features of torus palatinus
dense radiopaque shadow attached to the hard palate
well-defined periphery, may have convex or lobulated outline
maybe superimposed over roots of teeth

radiographic features of torus mandibularis
hyperostosis that protrudes from lingual aspect of mandibular alveolar process
premolar area, bilaterally
radiopaque shadow w/ defined borders superimposed over roots of teeth
radiographic features of enostosis (dense bone island)
well-defined periphery but may blend w/ trabeculae of surrounding bone
no effect on teeth but rarely associated w/ root resorption
similar opacity as cortical bone

4 types of giant cell lesions
central giant cell granulomas (CGCG)
cherubism
brown tumors of hyperparathyroidism
aneurysmal bone cysts
central giant cell granulomas (CGCG) usually affects which age
younger than 20
clinical signs of central giant cell granulomas (CGCG)
asympomatic, swelling if lesion is on boen surface
tenderness on palpation, occasionally pain
sometimes overlying mucosa is purple
radiographic features of central giant cell granulomas (CGCG)
well defined periphery, not corticated generally
radiolucent: small lesions
internally: subtle granular calcifications, thin wispy septae
if adjacent to teeth: absence of lamina dura
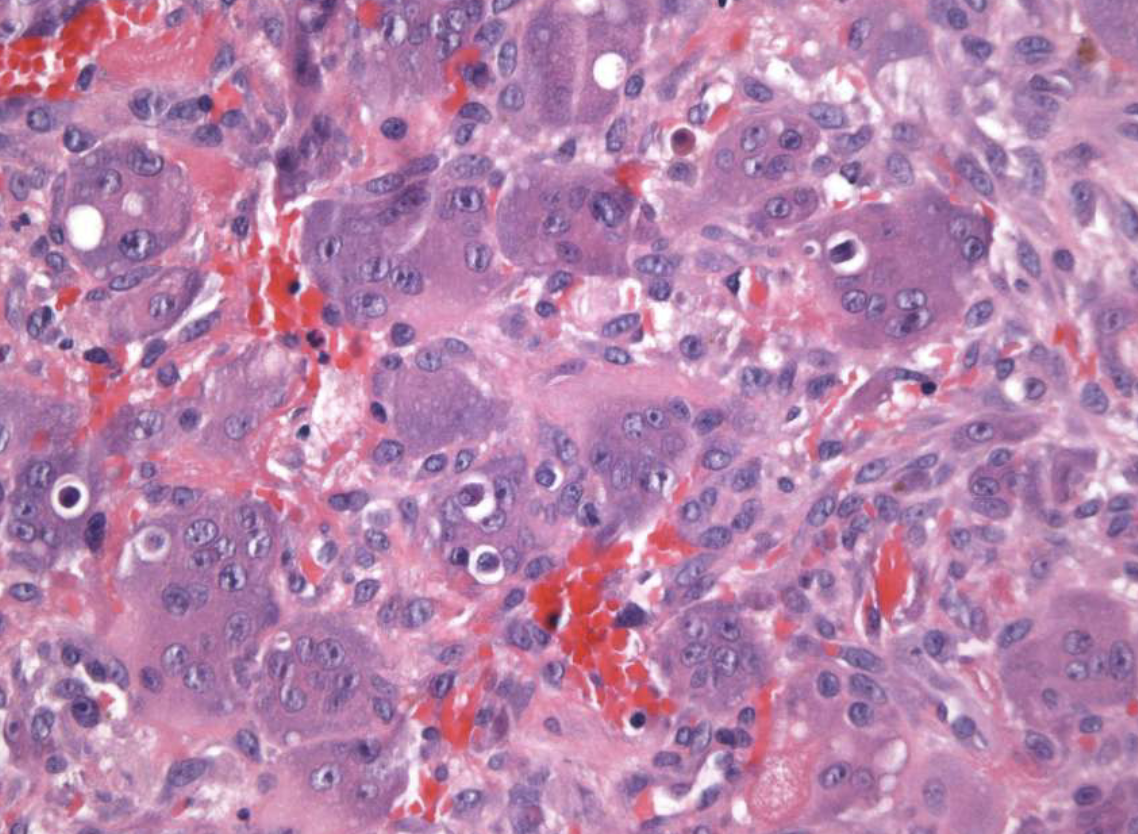
histopath features of central giant cell granulomas (CGCG)
multi-nucleated giant cells
background of ovoid-spindle shaped mesenchymal cells
tx options for central giant cell granulomas (CGCG)
thorough curettage
aggressive tumors may be treated w/ corticosteroids, calcitonin, interferon-alpha-2a
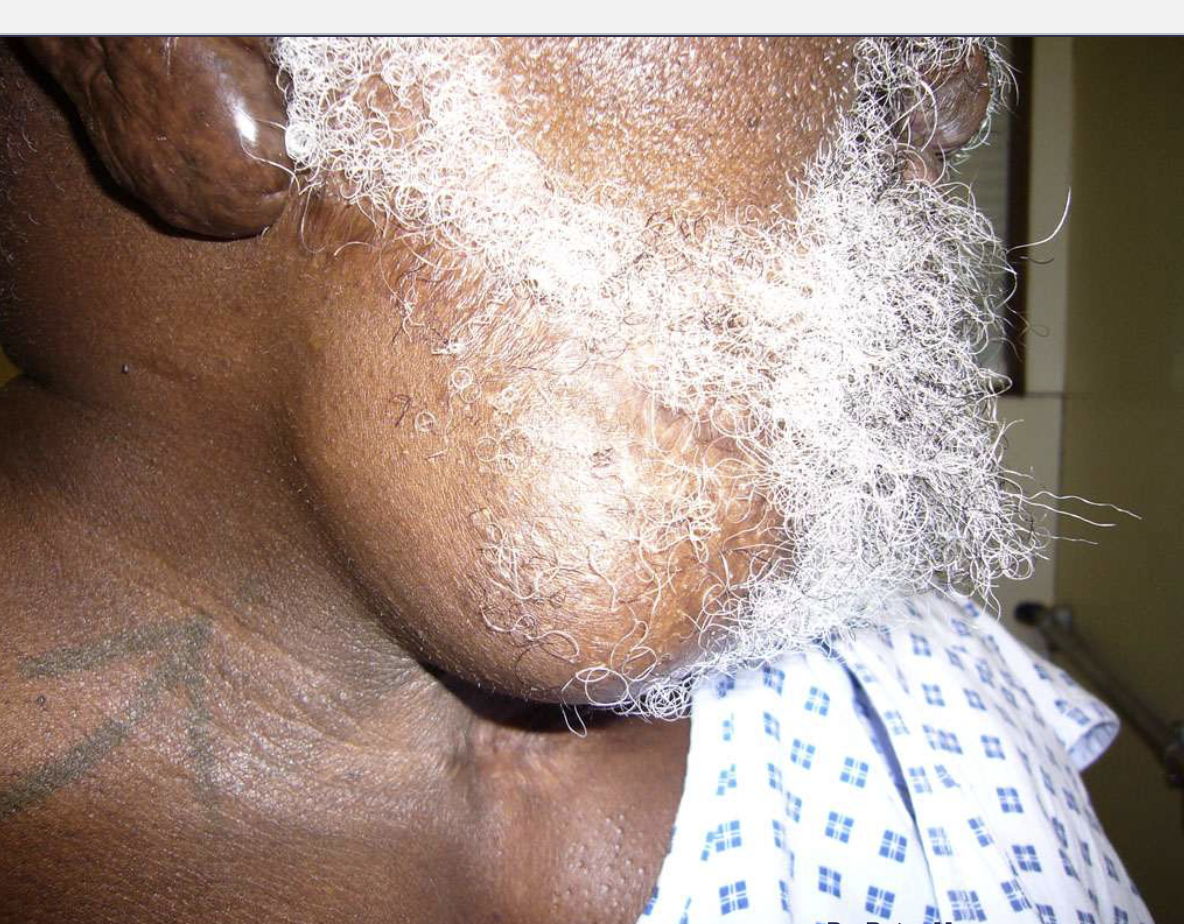
what’s cherubism
familial fibrous dysplasia of the jaws: bilateral swellings at mand angles
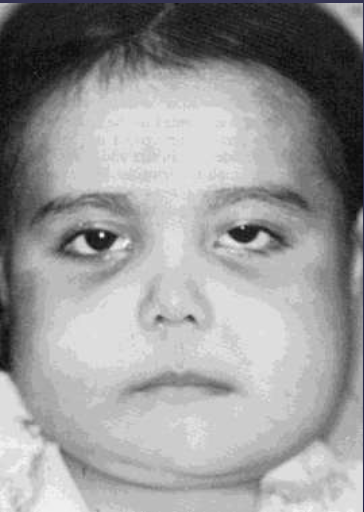
clinical signs of cherubism
early childhood
chubby face
firm on palation, painless, normal mucosa
stops growing + regresses w/ age
radiographic features of cherubism
bilateral multilocular radiolucencies
multicystic appearance
expansion/thinning of cortices
uncommon perforation
tooth displacement, resorption

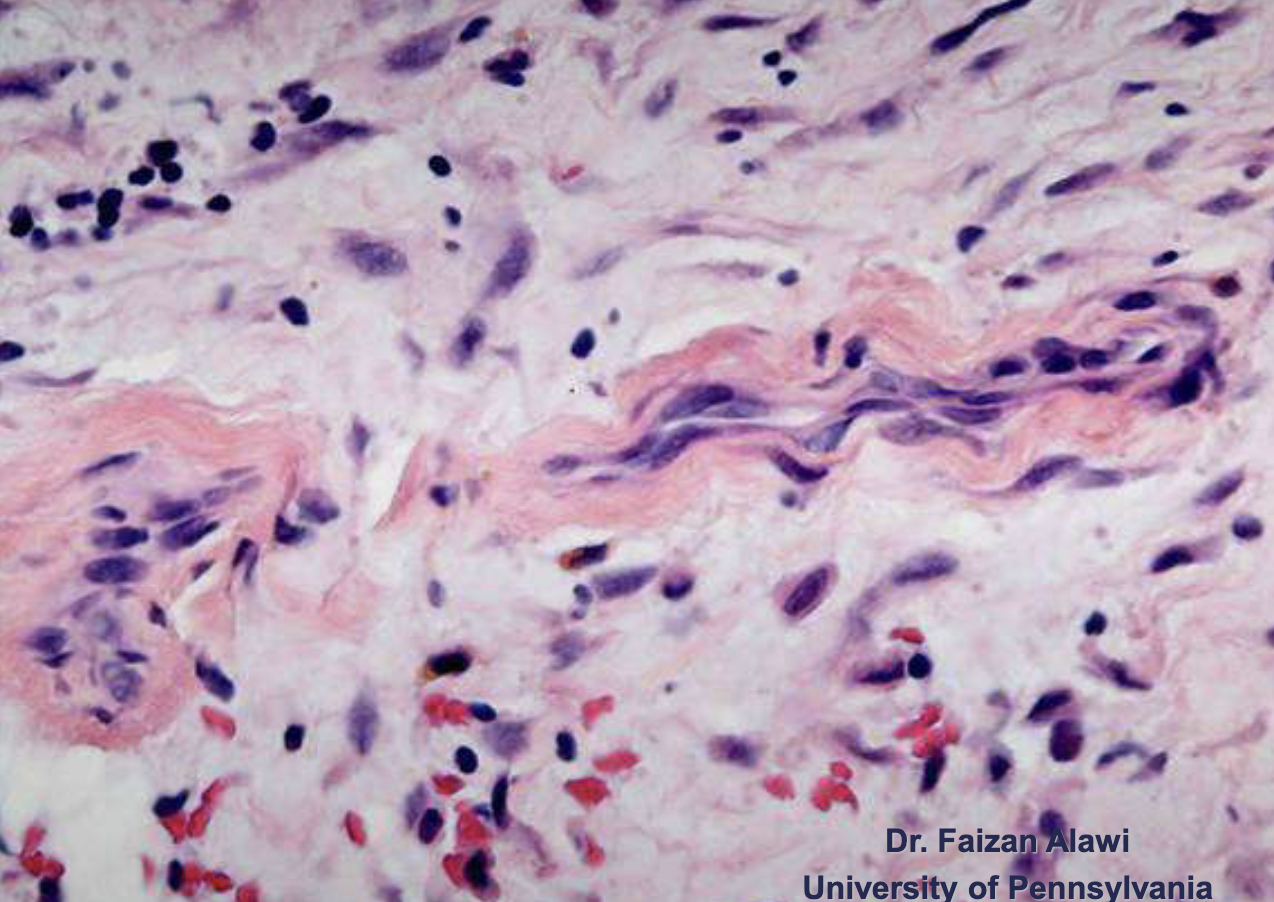
histopath feature of cherubism
eosinophilic cuffing (pink areas around purple), deposits around periphery of blood vessels
tx option for cherubism
intervention post puberty, usually no tx