EXAM 2 Liver Duplex
1/119
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
120 Terms
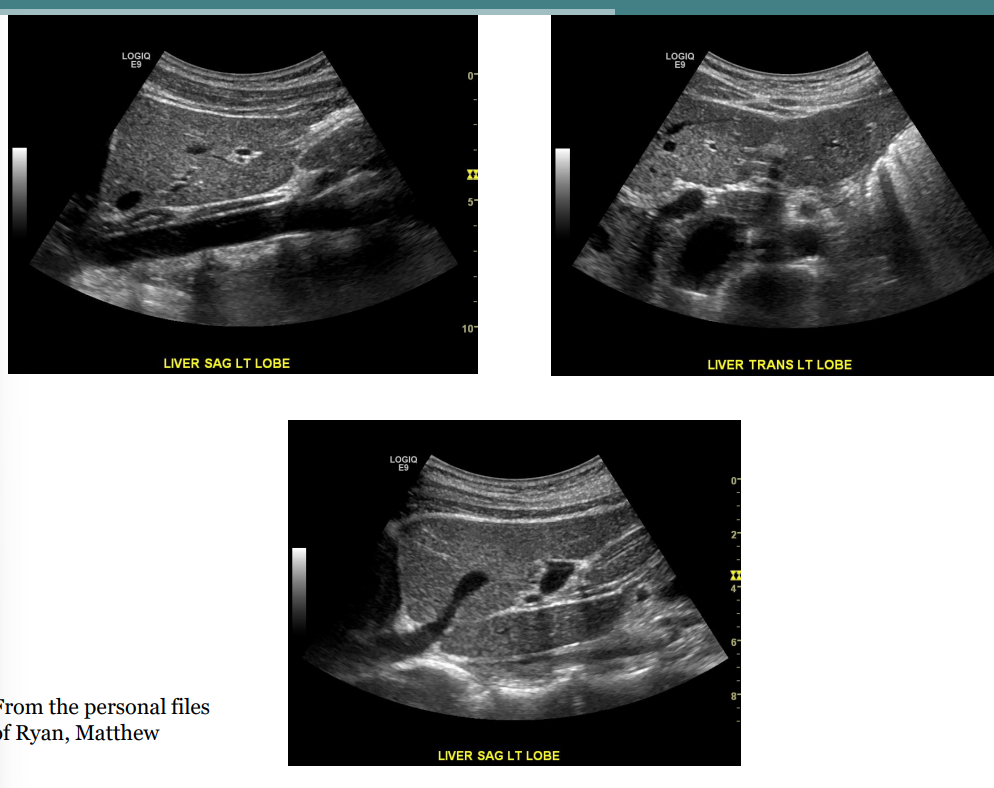
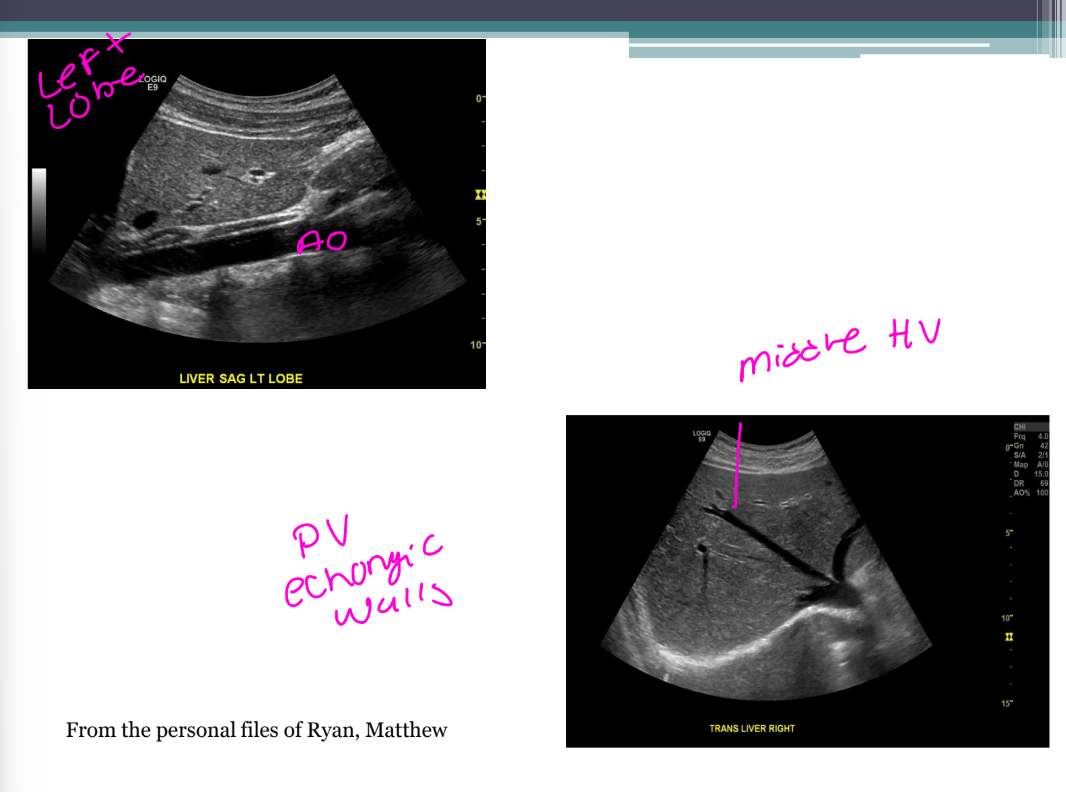
List the 4 key facts about the left lobe of the liver.
It has what 2 Lobes.
It is divided into segments by the what
It contains the what vein and artery?
It is imaged using the which window.
It has medial and lateral lobes.
It is divided into segments by the left hepatic vein.
It contains the left portal vein and left hepatic artery.
It is imaged using the subxiphoid window.
List the 2 key facts about the caudate lobe.
It is located near the what.
It is a separate ____with a separate ____supply
It is located near the IVC.
It is a separate lobe with a separate blood supply
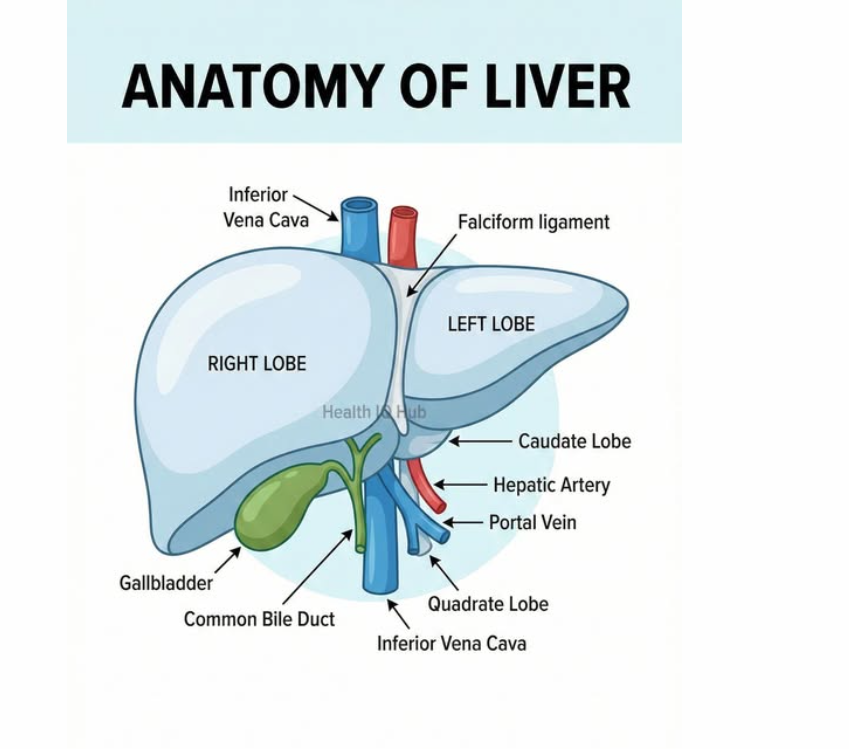
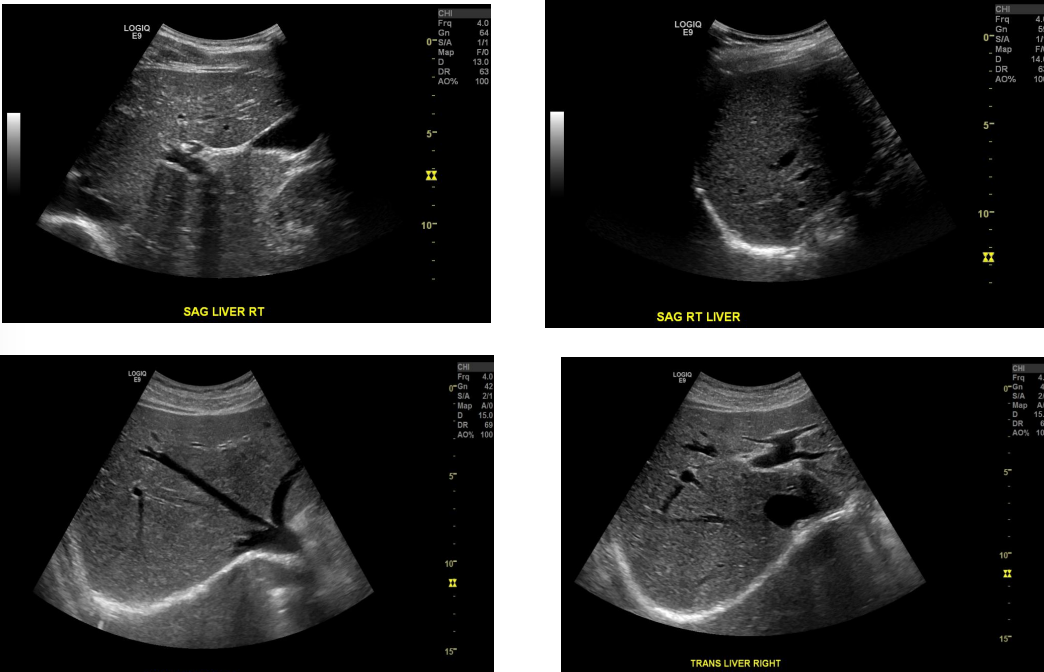
List the 5 key facts about the right lobe of the liver.
It has what 2 lobes.
It is separated from the what lobe by the what list 2
Divided into segments by what
contains what vein and what artery
what two windows can you use?
It has anterior and posterior lobes.
It is separated from the left lobe by the IVC and gallbladder.
It is divided into segments by the right hepatic vein.
It contains the right portal vein and right hepatic artery.
It is imaged using subcostal or intercostal windows.
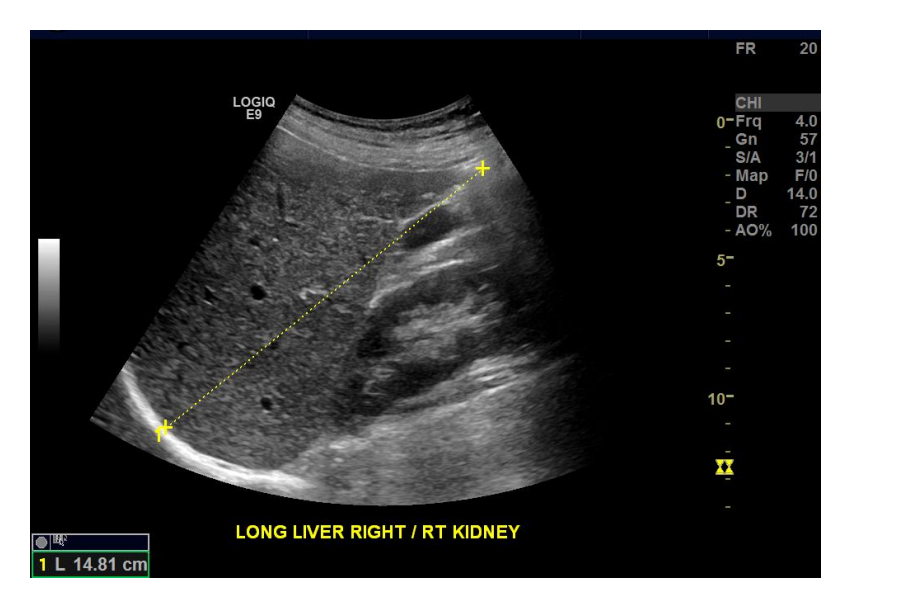
What is the normal longitudinal dimension of the liver?
The normal longitudinal dimension is 15–17 cm.
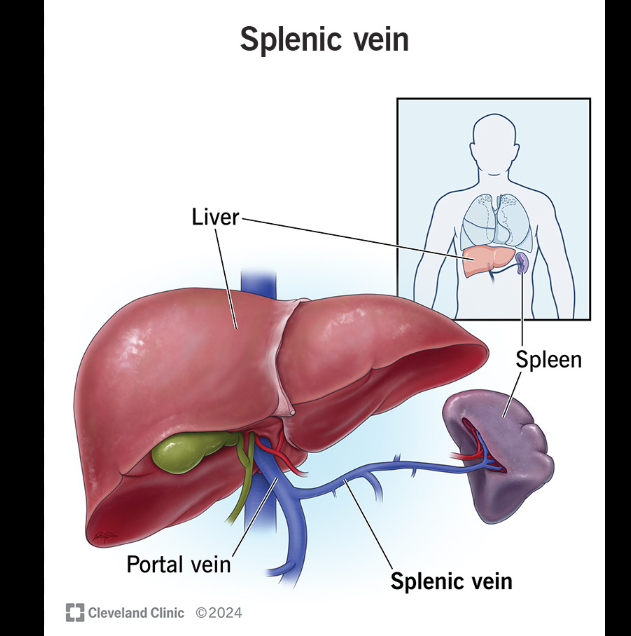
Explain the main function of the portal system.
The portal system drains - what? from the ___and ___into the liver.
The portal system drains nutrient-rich blood from the bowel and spleen into the liver.
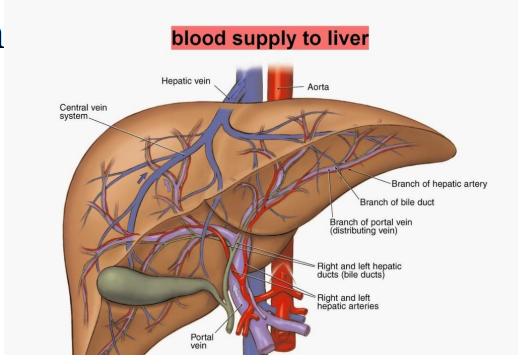
List the 2 main blood supplies to the liver and their percentages.- under normal conditions:
which one is the main source of supply for the liver?
Portal vein: 70% - main source of supply for the liver
Hepatic artery: 30%
What is normal portal venous flow direction called?
Normal portal venous flow is hepatopedal, meaning flow is toward/into the liver.
What happens to the portal vein branches as they terminate in the liver?
They get smaller.
Is the portal system part of the regular venous system?
No. It is separate from the venous system.
Portal venous system :
Blood from the stomach, intestines, pancreas, and spleen goes:
Digestive organs → portal vein → liver first
The liver then processes nutrients and removes harmful substances. After that:
Liver → hepatic veins → IVC → heart
So the portal system is like a special delivery route that makes one extra stop at the liver before returning to the heart.
List the 4 vessels of the portal venous system.
Main portal vein, or MPV
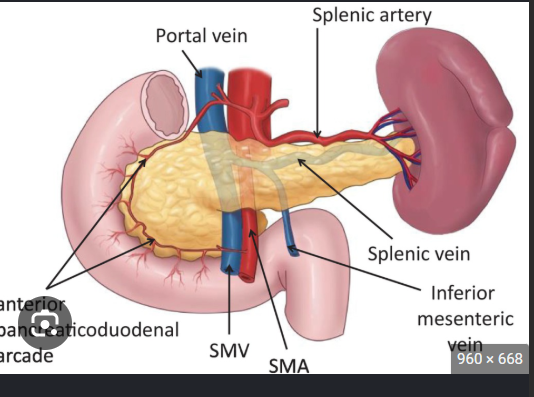
Superior mesenteric vein, or SMV
Splenic vein
Inferior mesenteric vein, or IMV
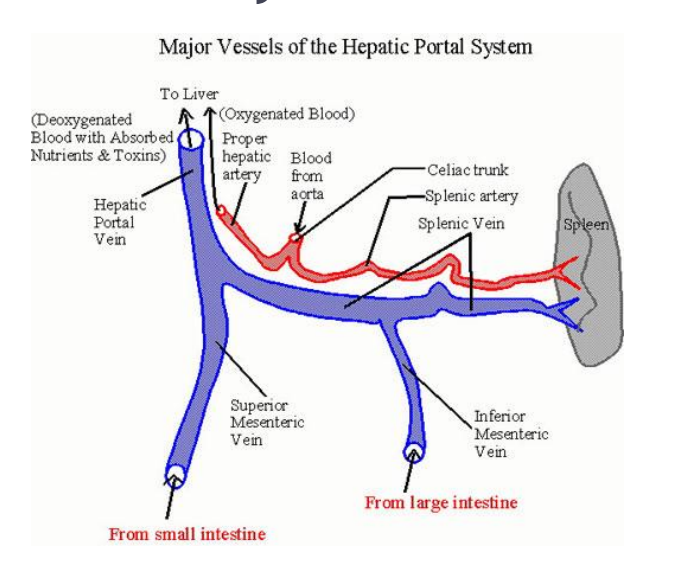
How is the main portal vein formed?
The MPV is formed _______to the ___—_by the union of the what vein and what vein.
The MPV is formed posterior to the pancreas by the union of the superior mesenteric vein and splenic vein.
What is the length of the main portal vein trunk?
The main trunk is 5–7 cm long.
Describe the course of the main portal vein.
Courses _____to _____, between layers of lesser omentum to where
It courses posterior to the duodenum, then between the layers of the lesser omentum to the porta hepatis.
What is the sonographic appearance of portal vein walls?
Portal vein walls are echogenic.
List the 2 main branches of the portal vein.
Right portal vein
Left portal vein
List the 2 branches of the right portal vein.
Anterior
Posterior
List the 2 branches of the left portal vein.
Medial
Lateral
What direction does the common hepatic artery travel?
It travels rightward to the liver.
List the 2 Doppler waveform features of the common hepatic artery.
Low resistance
Spectral broadening
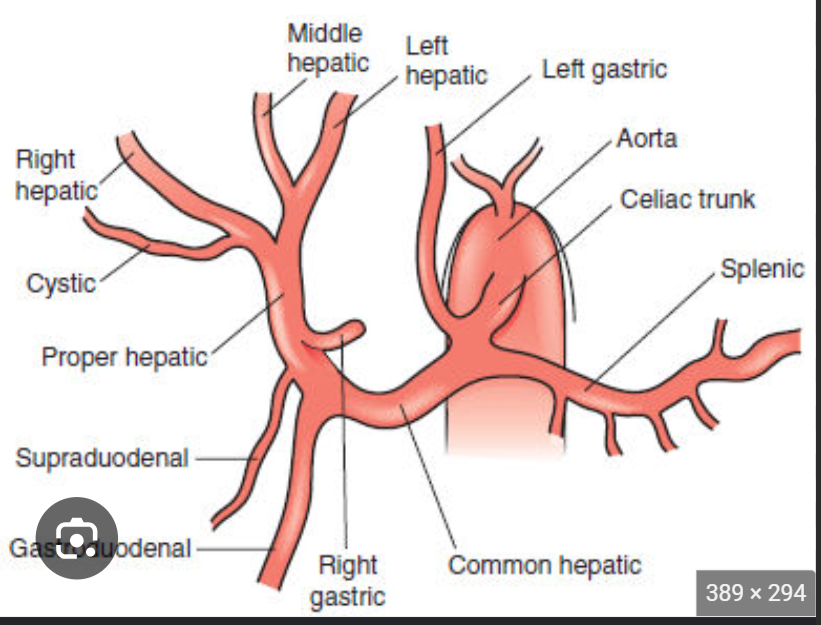
List the 3 arterial branches of the common hepatic artery.
Gastroduodenal artery
Proper hepatic artery
Right gastric artery
Where is the proper hepatic artery imaged?
It is imaged through the _____window at the where?
It is imaged through the intercostal window at the porta hepatis.
The porta hepatis is the liver’s main doorway.
It is an area where important tubes and blood vessels enter or leave the liver:
Portal vein enters
Hepatic artery enters
Bile duct leaves
Think of the liver like a building and the porta hepatis is the front entrance where the plumbing and blood vessels pass through.
The hepatic veins do not leave through the porta hepatis; they drain from the liver directly into the IVC.
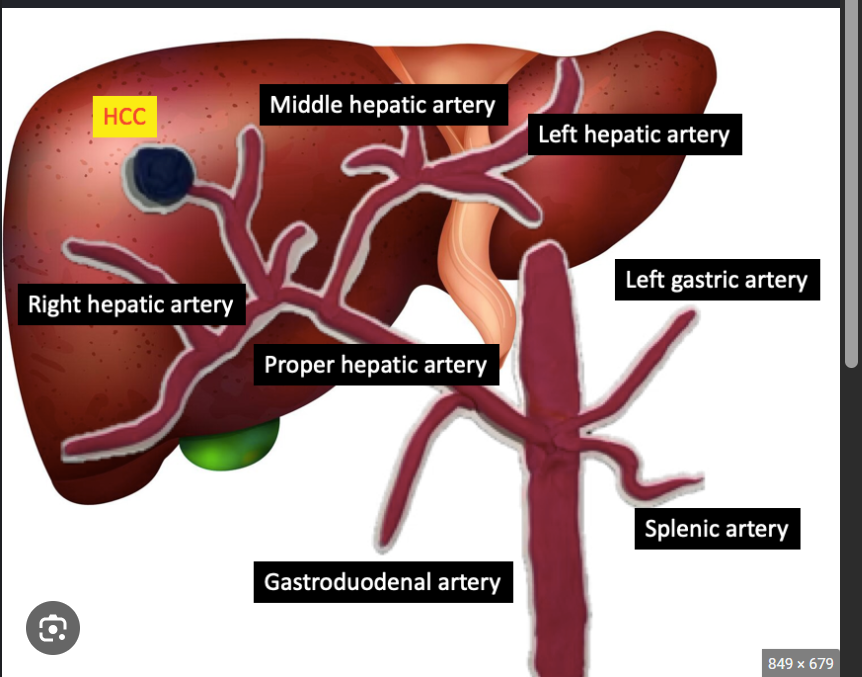
Where are the right and left hepatic arteries located?
They are within the liver parenchyma.
Which ______artery supplies the right lobe?
The right hepatic artery supplies the right lobe.
Which ____-artery supplies the left lobe?
The left hepatic artery supplies the left lobe.
What Doppler waveform should the hepatic artery have?
It should have a low-resistance waveform.
List the 3 key facts about the intrahepatic ducts.
They are within the where?
They include what ducts.
They join with the ____duct. to form the what?
They are within the liver parenchyma.
They include right and left ducts.
Joins with cystic duct to form common bile duct
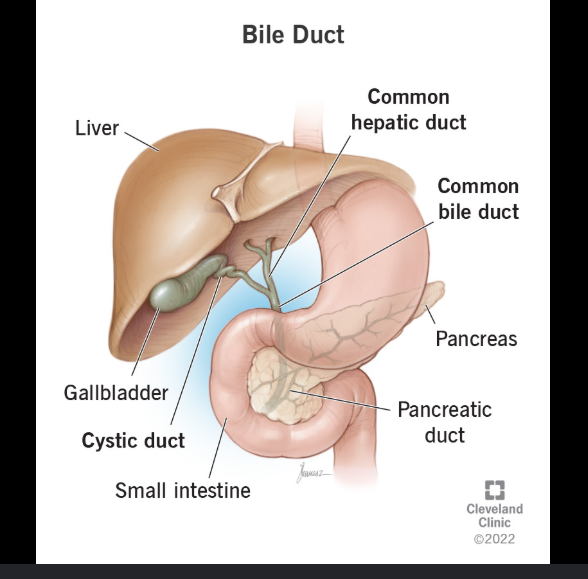
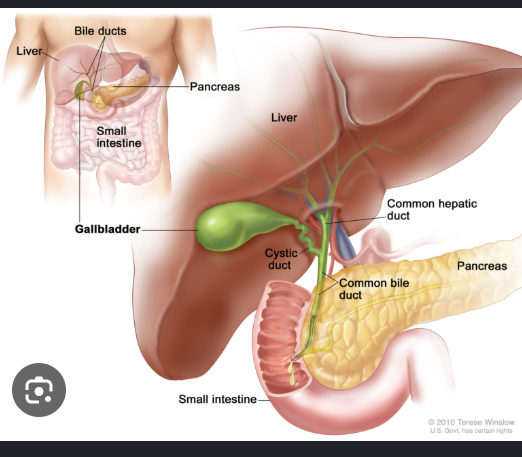
Intrahepatic ducts merge into the right and left hepatic ducts, which join outside the liver to form the common hepatic duct. The cystic duct (from the gallbladder) then merges with this common hepatic duct to form the common bile duct, which delivers bile into the small intestine
Intrahepatic Ducts: A network of tiny tubes inside the liver that collect bile.
Right & Left Hepatic Ducts: The two main branches exiting the liver.
Common Hepatic Duct: Formed by the union of the right and left hepatic ducts.
Cystic Duct: The tube connecting the gallbladder to the common hepatic duct. Bile flows back and forth here for storage.
Common Bile Duct: Formed where the common hepatic duct and cystic duct meet. It transports bile through the pancreas to the duodenum (the first part of the small intestine) to aid in digestion
List the 2 key facts about the common bile duct.
It extends from the what to the what.
what is the normal size of the common bile duct
It extends from the porta hepatis to the pancreatic head.
Normal size is 4–6 mm.
Where do hepatic veins originate and drain? and at the level of the what?
They originate in the liver and drain into the IVC at the level of the diaphragm
What happens to hepatic veins as they approach the diaphragm?
They enlarge as they near the diaphragm.
List the 3 hepatic vein tributaries.
Right hepatic vein
Middle hepatic vein
Left hepatic vein
What is the wall appearance of hepatic veins?
Hepatic veins have non-echogenic walls.
What do hepatic veins do anatomically? - They divide the liver into ______?
They divide the liver into segments.
List the 3 hepatic veins and what each one divides.
RHV: largest hepatic vein; divides the right lobe into anterior and posterior segments.
MHV: divides the liver into right and left lobes.
LHV: divides the left lobe into medial and lateral segments.
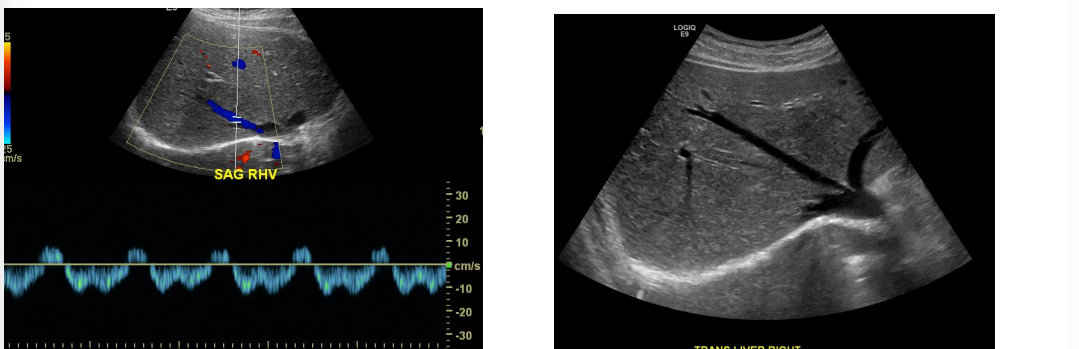
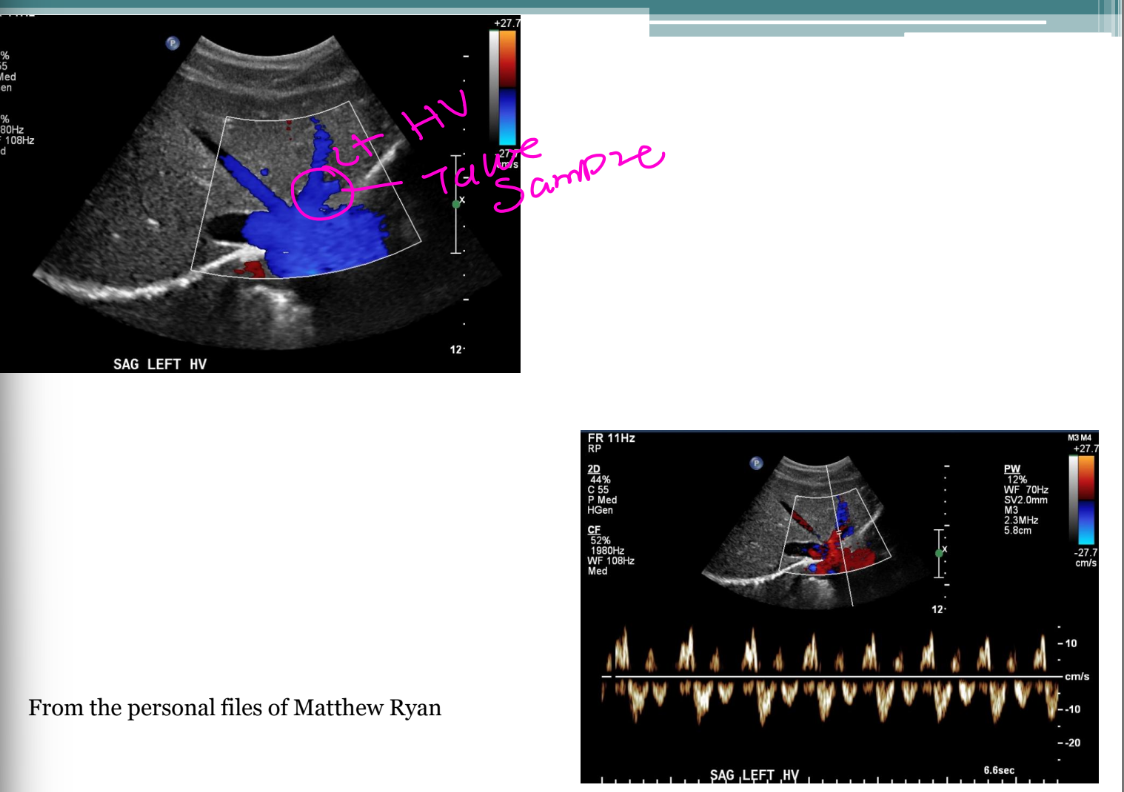
List the 2 normal hepatic vein flow features.
what is the normal direction ? and list 3 ways to describe the waveform?
Hepatofugal flow
Phasic, bidirectional/pulsatile waveform
Simple reminder:
Portal veins normally flow into the liver. Hepatic veins normally flow away from the liver.
The hepatic veins collect blood from the liver and “dump” it into the IVC, which then carries it to the right atrium of the heart.
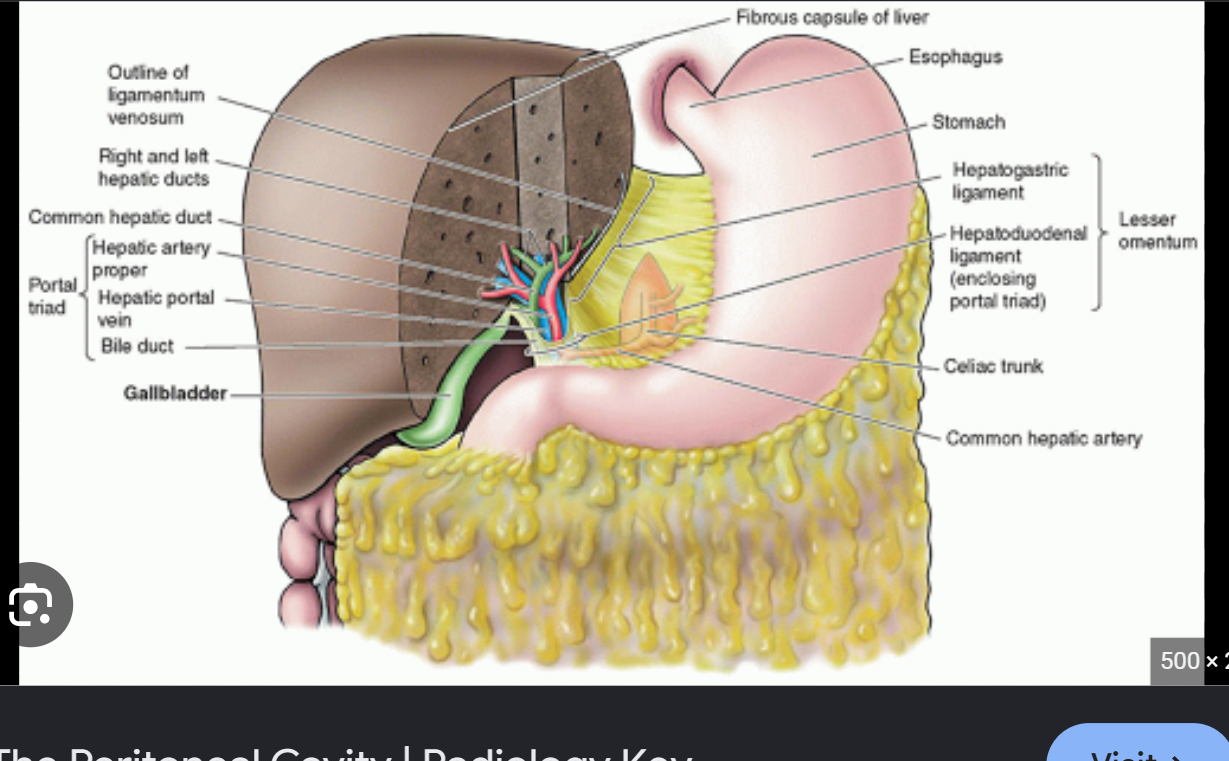
List the 3 structures in the portal triad.
Hepatic duct
Portal vein
Hepatic artery
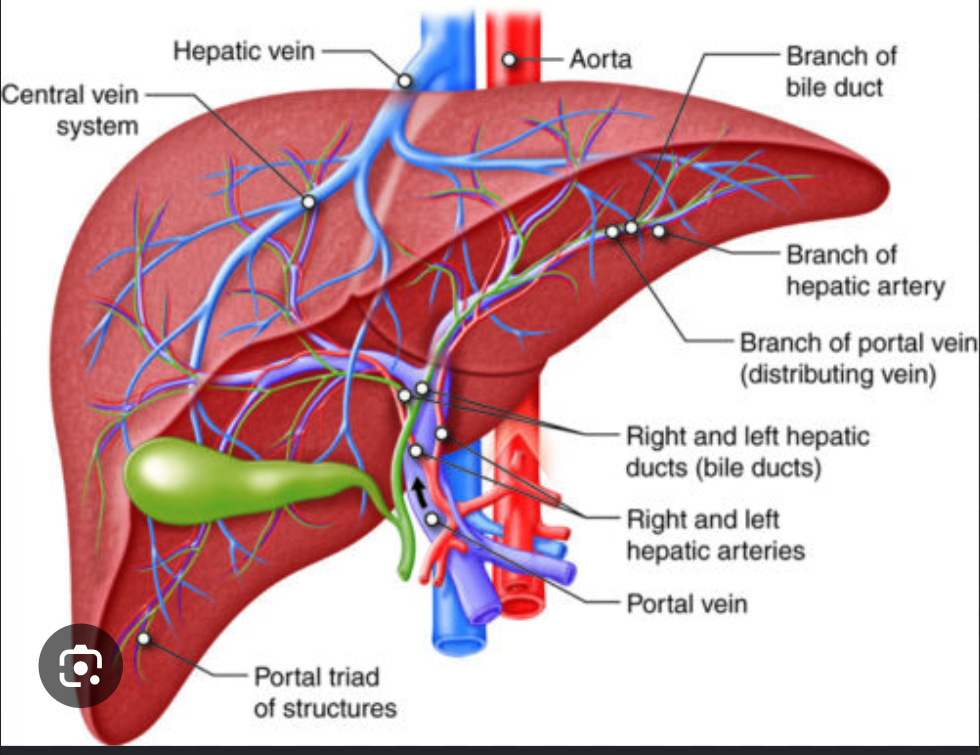
Describe the relationship between portal veins and hepatic veins. - how do they run towards each other?
Portal veins and hepatic veins run perpendicular to each other.
When the portal vein is long, how does the hepatic vein appear?
When the portal vein is long, the hepatic vein appears transverse.
List the 2 basic liver functions. - most important
Bile formation and secretion
Detoxification
Bile formation and secretion:
The liver makes a liquid called bile. Bile helps your body break down and digest fats from food. The liver sends bile to the gallbladder, where it is stored until needed.
Detoxification:
The liver acts like a filter. It removes or changes harmful substances from the blood, such as alcohol, medicines, and waste, so the body can safely get rid of them.
List the 2 liver blood tests.
Bilirubin, Albumin
Bilirubin:
Bilirubin is a yellow waste product made when old red blood cells break down.
The liver takes bilirubin out of the blood, puts it into bile, and helps the body get rid of it through stool.
If bilirubin gets too high, the skin and eyes can turn yellow. This is called jaundice.
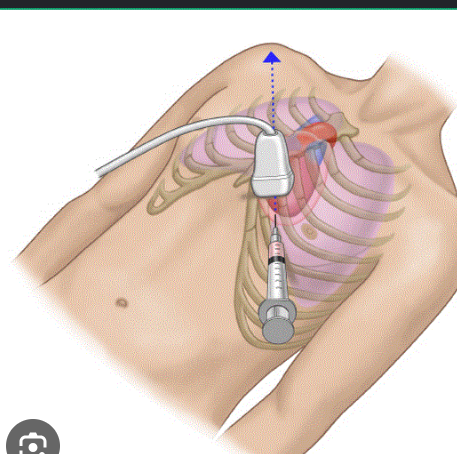
List the 4 patient/positioning techniques for liver duplex.
Patient begins supine.
Use left lateral decubitus if needed.
Utilize breathing techniques.
Change windows
List the 3 imaging windows used for liver duplex.
Subxiphoid
Subcostal
Intercostal
What transducer is used for liver duplex?
A curvilinear 2.0–6.0 MHz transducer.
List the 6 indications for a liver duplex exam.
Hepatitis
NAFLD / NASH - Non-Alcoholic Fatty Liver Disease
◦ NASH – old nomenclature
Cirrhosis / ETOH abuse / portal hypertension
Abnormal lab values
Cancer
Portal hypertension assessment
Cirrhosis:
Cirrhosis means the liver has become badly scarred and damaged over time. The scar tissue makes it harder for the liver to do its job and for blood to flow through it.
EtOH abuse:
“EtOH” means alcohol. Drinking too much alcohol for many years can repeatedly injure the liver, causing inflammation and eventually cirrhosis.
What is the protocol ?
The RUQ protocol first.
Grey Scale / Color Doppler / Spectral Doppler
Splenic vein – posterior to pancreas head
Portal vein : Main , Right , Left
Hepatic veins: Right , middle, Left
Grey Scale / Color Doppler / Spectral Doppler
Inferior Vena Cava
Color Doppler / Spectral Doppler
Hepatic artery : Main, common or proper , Right and left, & Collateral venous pathways if noted
Color Doppler and Spectral Doppler : SMV
What does shear wave elastography measure?
It measures the stiffness of liver tissue.
List the 4 patient histories where shear wave elastography may be performed.
Elevated LFTs (liver function test)
Hepatitis
Cirrhosis
NASH (Non-Alcoholic Fatty Liver Disease)
Elevated liver function tests (LFTs) or enzymes simply indicate that your liver is stressed, inflamed, or injured. When liver cells become damaged, they leak higher-than-usual levels of enzymes into your bloodstream
List the 7 technique points for elastography. (MAYBE SKIP?)
Technique is vendor specific.
Patient may be what list 2
_____arm is placed over the ____.
Use Couinaud segments 7 or 8.
Sample at least ____cm from the liver surface.
Choose an area free of structures such as _____.
Apply ____pressure with the transducer.
Technique is vendor specific.
Patient may be supine or (Left Posterior Oblique).
Right arm is placed over the head.
Use Couinaud segments 7 or 8.
Sample at least 1.0 cm from the liver surface.
Choose an area free of structures such as vessels.
Apply firm pressure with the transducer.
Should hold breathing, beacuse it affects the velocities and should be fasting becasuse it could affect the velocities of the stiffness of the liver)
How many elastography samples are taken?
10–12 samples are taken.
List the 4 GE liver fibrosis staging categories with m/s.
Normal–mild:
Mild–moderate:
Moderate–severe:
Cirrhosis:
what does red mean and what does blue mean?
Normal–mild: 1.35–1.66 m/s
Mild–moderate: 1.66–1.77 m/s
Moderate–severe: 1.77–1.99 m/s
Cirrhosis: >1.99 m/s
Red is fast flow stiff, blue is slower not as stiff - no vessels just the tissues
What values indicate no clinically significant fibrosis for Phillips/Siemens criteria?
and Clinically significant fibrosis / cirrhosis: METAVIR stage? and tell me the value of m/s ?
No clinically significant fibrosis is METAVIR stage <F2, or F0–F1, with values <1.37 m/s
Clinically significant fibrosis / cirrhosis: METAVIR stage > F4 (high end of F4) >2.2 m/s
List the 4 normal grayscale liver findings.
Homogeneous liver
Low-level echoes
Smooth borders
Intrahepatic vessels easily identified
What is normal portal vein flow direction?
Normal portal vein flow is hepatopedal, meaning flow is into the liver.
What Doppler angle should be used for the portal vein?
Doppler angle should be ≤60° and parallel to the flow state.
What should be measured in the portal vein?
Velocity should be measured.
Are portal vein velocities consistent?
No. Velocities are widely variable.
What is the normal MPV diameter in quiet respiration?
The MPV diameter should be <13 mm in quiet respiration.
What may an MPV diameter >13 mm suggest?
It may suggest portal hypertension.
Describe normal portal venous flow.
Normal flow is what flow with possible minor respiratory _______.
Normal flow is continuous antegrade flow with possible minor respiratory phasicity.
What can cause exaggerated portal venous pulsatility? List 2
Right heart failure or tricuspid regurgitation can produce exaggerated pulsatility.
How should the MPV diameter be measured?
Measure the portal vein diameter where it crosses _____to the ____during quiet respiration.
Want to sample as where of the liver as we can see it
Measure the portal vein diameter where it crosses anterior to the IVC during quiet respiration.
Want to sample as far outside of the liver as we can see it

What position should the patient be in for MPV diameter measurement?
The patient should be supine.
What waveform should normal hepatic arteries have?
They should have low-resistance waveforms.
What index should be obtained for hepatic arteries?
A resistive index, or RI.
What is the RI formula?
RI = (PSV − EDV) / PSV
Which approach / window is used for the proper and right hepatic artery?
The intercostal approach.
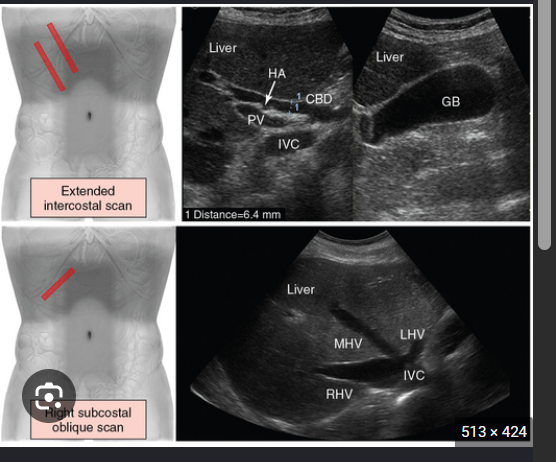
Which approach is used for the left hepatic artery?
The subxiphoid approach.
What waveform is seen at the hepatic vein confluence?
A “flying W” waveform.
What is normal hepatic vein flow direction?
Hepatofugal flow direction.
What waveform is seen in the IVC?
A “flying W” waveform.
What affects hepatic venous diameter?
Hepatic venous diameter varies with respiration.
List the 3 hepatic vasculature pathologies covered
Portal hypertension, or PHTN
Portal vein thrombosis, or PVT
Hepatic vein obstruction
List the 4 abnormal liver grayscale findings
Heterogeneous echotexture
Nodular liver surface
Increased echogenicity
Intrahepatic vessels not easily identified
Liver surface is nodular:
This means the outside of the liver looks bumpy and uneven instead of smooth.
It happens because cirrhosis creates scar tissue. As the liver tries to repair itself, small lumps called nodules form.
Think of it like a smooth sponge becoming hard, scarred, and bumpy.
What fluid finding may be present?
Ascites may be present.
What spleen finding may be present?
The spleen may be enlarged. (because flow is backing into the spleen)
Explain what happens in portal hypertension at the sinusoid level.
____changes at the sinusoid level cause
list 2 things that changes, loses the ability to manage what? what develop?
Fibrotic changes at the sinusoid level cause resistance and pressure changes. The liver loses the ability to manage blood flow, and collateral pathways develop.
Sinusoidal level means the problem is happening in the liver’s tiny blood channels called sinusoids.
Sinusoids are like very small pathways where blood flows through the liver so the liver cells can clean and process it.
In cirrhosis, scar tissue squeezes these tiny channels, making it harder for blood to pass through. This causes pressure to build up in the portal vein, called portal hypertension.
List the 3 classifications of portal hypertension. & Which classification is most common?
Extrahepatic
Hyperdynamic
Intrahepatic portal hypertension is most common.
These are three ways portal hypertension can happen:
Extrahepatic:
The blockage is outside the liver, such as a blood clot in the portal vein.
Hyperdynamic:
Too much blood is flowing into the portal system, so the pressure becomes high.
Intrahepatic — most common:
The problem is inside the liver. Cirrhosis and scar tissue make it difficult for blood to flow through the liver, causing pressure to build up.
Think of it like a traffic jam:
Extrahepatic: the road is blocked before the liver.
Hyperdynamic: too many cars are entering the road.
Intrahepatic: the roads inside the liver are narrowed or blocked.
List the 6 effects of elevated pressure in portal hypertension.
Ascites
Splenomegaly
GI / esophageal bleeding
Jaundice
Signs of hepatic failure
Hepatic encephalopathy
GI – Esophageal bleeding:
This means bleeding in the digestive system from the esophagus, the tube that carries food to the stomach.
With portal hypertension, pressure builds up and causes veins in the esophagus to become enlarged. These enlarged veins are called esophageal varices.
Hepatic encephalopathy:
This happens when the liver cannot properly remove toxins from the blood.
The toxins build up and travel to the brain, causing problems such as:
Think of the liver as a filter. When the filter is damaged, waste stays in the blood and affects the brain.
List the 2 portal flow directions used in PHTN evaluation.
Hepatopedal: flow into the liver; normal state
Hepatofugal: flow away from the liver - abnormal
Are velocities a good diagnostic parameter for PHTN?
can you name 4 more useful findings are:
No. Velocities are not a good diagnostic parameter.
Because portal vein velocities vary a lot from person to person, even in normal patients. A person with portal hypertension may have a velocity similar to someone without it, so one velocity number cannot reliably prove PHTN.
Instead, more useful findings are:
Direction of flow—especially reversed, hepatofugal flow
Enlarged portal vein
Portosystemic collaterals
Other signs such as ascites or an enlarged spleen
So remember: velocity alone is unreliable because normal and abnormal values can overlap.
What happens to portal vein size in PHTN? due to what?
Portal vein size increases due to elevated pressures.
Why is portal vein enlargement important?
It is a reliable sign for portal hypertension.
List the 2 types of extrahepatic portal hypertension.
Prehepatic
Posthepatic
List the 3 prehepatic causes of extrahepatic PHTN.
Portal vein thrombosis
Compression
Stenosis
Prehepatic = before the liver
The blockage is in the portal vein before blood enters the liver.
Examples:
Portal vein clot
Portal vein narrowing
Something pressing on the portal vein
So the blood is saying: “I cannot get into the liver.”
List the 3 posthepatic causes of extrahepatic PHTN.
Hepatic vein or IVC thrombosis
Compression
Stenosis
Posthepatic = after the liver
The blockage is in the hepatic veins or IVC after blood passes through the liver.
Examples:
Hepatic vein clot
IVC clot or narrowing
Something pressing on these vessels
So the blood is saying: “I entered the liver, but I cannot get out.”
What causes hyperdynamic PHTN? list 2
Arteriovenous malformations (AV fistula) or conditions that cause arterial portal fistulas.
Arterial-portal fistula
This is an abnormal shortcut connecting a high-pressure artery directly to the low-pressure portal vein.
Because arteries carry blood with more force, blood rushes into the portal vein and raises its pressure.
Think of it like connecting a powerful fire hose to a small garden hose. Too much water enters too quickly, so the pressure builds up.
So remember:
Hyperdynamic = too much blood entering the portal system.
Hyperdynamic portal hypertension means the pressure is high because too much blood is being pushed into the portal system, not because the liver is blocking it.
On Doppler, you may see:
Fast, increased portal vein flow
Turbulent color aliasing near an abnormal artery-to-portal vein connection
A portal vein branch that looks pulsatile like an artery
The feeding hepatic artery shows high velocity and low resistance
Think of it as:
Too much fast arterial blood enters the portal vein → portal pressure rises.
List the 2 types of intrahepatic portal hypertension.
Presinusoidal
Postsinusoidal
List the 4 presinusoidal causes of intrahepatic PHTN.
Hepatic fibrosis: Scar tissue forms in the liver and makes it harder for blood to pass.
Sarcoidosis: Small clumps of inflamed cells form in the liver and can block blood flow.
Schistosomiasis: A parasite causes inflammation and scarring around the liver’s small portal vessels.
Lymphoma: Cancer of the lymphatic system can enter or press on liver tissue and interfere with blood flow
These are presinusoidal causes of intrahepatic portal hypertension. That means the problem is inside the liver but before blood reaches the tiny sinusoids.
These conditions narrow or block the small blood pathways before the sinusoids, causing portal pressure to build up.
List the 2 postsinusoidal causes of intrahepatic PHTN.
Cirrhosis
Veno-occlusive disease
Postsinusoidal means the blood-flow problem happens after blood passes through the liver’s tiny channels called sinusoids, but before it can leave the liver normally.
Cirrhosis: Scar tissue makes the liver hard and squeezes the tiny blood channels, so blood has trouble moving through and out of the liver.
Veno-occlusive disease: The tiny veins that carry blood out of the liver become narrowed or blocked.
Think of the sinusoids as tiny roads through the liver. In postsinusoidal disease, the exit side of those roads is blocked, so blood backs up and causes portal hypertension.
cirrhosis leads to what that causes a increased in what to what flow?
Leads to bridging fibrosis that causes increased
resistance to hepatic inflow
Hepatic inflow means the blood flowing into the liver.
Blood enters the liver through:
The portal vein — most of the blood
The hepatic artery — the rest
With cirrhosis, scar tissue makes it harder for this incoming blood to travel through the liver.
Cirrhosis → scarring inside the liver → resistance to incoming blood → portal pressure builds up.
“increased resistance to hepatic inflow” simply means blood has a harder time entering and passing through the scarred liver.
Hepatocellular death: Liver cells die from repeated damage.
Parenchymal degeneration: The healthy working tissue of the liver becomes damaged.
Regeneration: The liver tries to repair itself by growing new cells, but they grow in abnormal lumps called nodules.
Bridging fibrosis: Thick bands of scar tissue form and connect different damaged areas, almost like bridges of scar tissue across the liver.
Increased resistance to hepatic inflow: The scar tissue squeezes the tiny blood pathways, making it difficult for blood from the portal vein to enter and travel through the liver.
Explain how portal flow changes as PHTN progresses.
At first, increased in portal ______maintains portal venous ______.
As sinusoidal resistance increases, it does what?
Eventually, sinusoidal resistance becomes what than what, causing what to flow and diversion of flow to ______.
At first, increased portal pressure maintains portal venous volume.
As sinusoidal resistance increases, it equalizes with portosystemic collateral resistance.
Eventually, sinusoidal resistance becomes greater than collateral resistance, causing reversal of portal flow and diversion of flow to collaterals.
(REVERSED OF MAIN PV IS CHRONIC).
portosystemic collateral = an alternate vein that carries portal blood around the liver. Blocked/scarred liver route → blood uses collateral veins → blood returns toward the heart
At first, higher pressure keeps blood moving through the liver. As cirrhosis worsens, the liver becomes harder to flow through, so blood reverses and takes collateral “detour” veins around the liver.
List the 2 types of portosystemic collaterals.
Tributary collaterals
Developed collaterals
What are tributary collaterals?
They are ______vessels that normally drain into the where list 3 systems
They are preexisting vessels that normally drain into the portal, splenic, and mesenteric venous systems.
Because those veins normally collect blood from the stomach, intestines, and spleen and carry it into the portal system so the blood can go to the liver.
Before portal hypertension:
Organs → small veins → splenic/mesenteric veins → portal vein → liver
After portal hypertension:
High pressure makes blood back up and reverse through some of those veins. They enlarge and become collateral detours toward the regular venous system.
So they are normal drainage veins first and only become important collaterals when the flow reverses because of portal hypertension.
What is the most prevalent tributary collateral?
The coronary vein.
What are developed collaterals?-
They are vessels that are not normal ________but develop or recanalize in the setting of what?
What is the easiest developed collateral to identify?
What are developed collaterals?
They are vessels that are not normal tributaries but develop or recanalize in portal hypertension. PHTN
Question:
What is the easiest developed collateral to identify?
The umbilical vein.
Tributary Collaterals
What is another name for the coronary vein?
What varices are associated with the coronary vein?
What acoustic window is used to see the coronary vein?
The left gastric vein.
Esophageal varices.
The left lobe acoustic window.
Esophageal varices are swollen, enlarged veins in the esophagus, the tube that carries food to the stomach.
They happen when portal hypertension makes it difficult for blood to flow through the liver. The blood takes a detour through small veins around the esophagus, causing them to swell.
So the coronary vein acts as the collateral detour, and the swollen veins that result around the esophagus are the esophageal varices.
Think of it as:
Portal blood backs up → takes the left gastric vein side road → fills the esophageal veins → varices form.
That is why the slide says reversed flow in the coronary vein can be an early sign of portal hypertension.
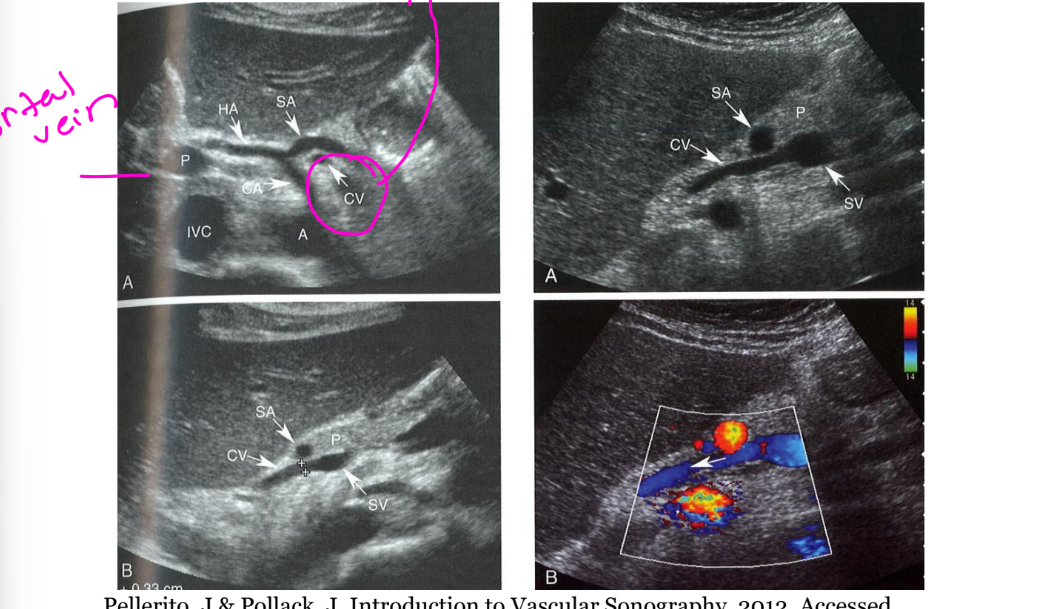
Where is the coronary vein seen?
It is seen superior to the _____artery and anterior to the _____axis or posterior to the what artery or what artery.
What is the normal coronary vein diameter?
What is an early sign of PHTN in the coronary vein?
It is seen superior to the splenic artery and anterior to the celiac axis or posterior to the common hepatic artery or splenic artery.
It should not exceed 5–6 mm.
Reversed flow is an early sign
When pressure gets too high in the portal system, blood has trouble passing through the liver. The body opens or enlarges other veins to create detour pathways around the liver.
So:
Portal hypertension → blood backs up → collateral veins develop/enlarge → blood is redirected around the liver
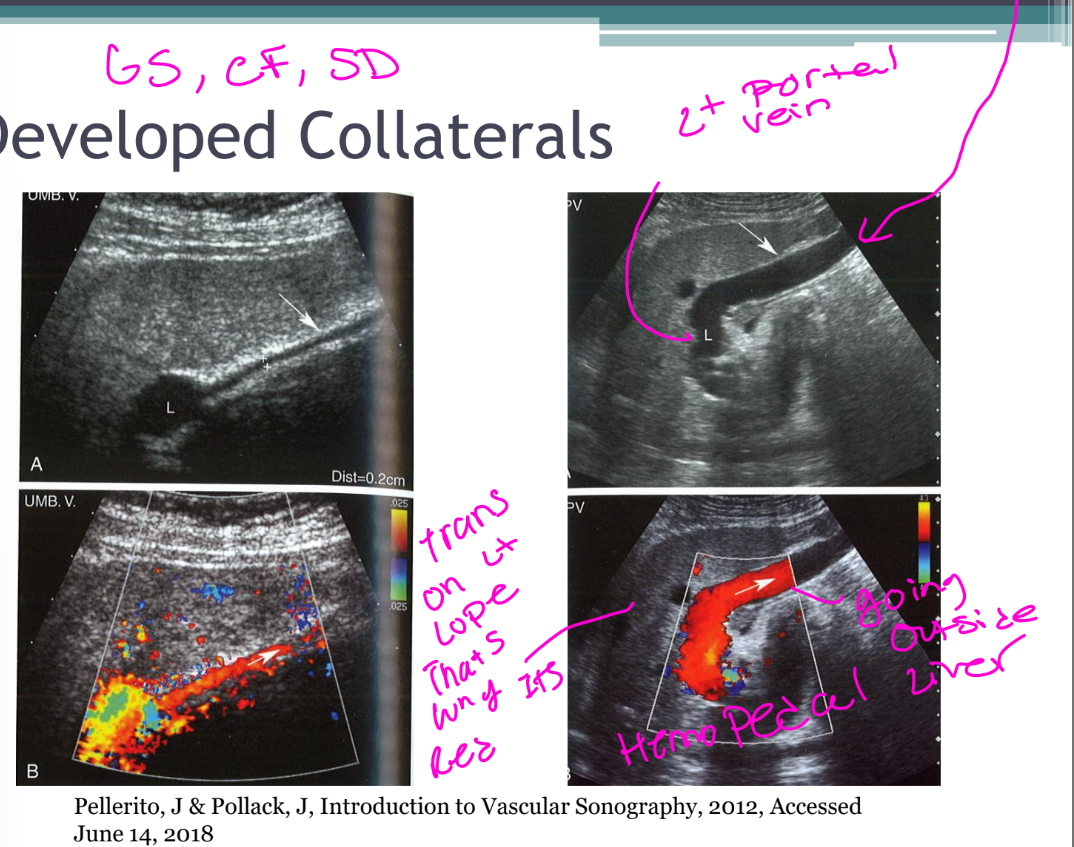
List the 6 key features of the umbilical vein collateral. Developed Collaterals
It is a remnant of ___circulation.
It is located in the what.
It courses from the ______to the anterior what vein.
It normally measures ____.
It may become numerous and tortuous.
Recanalized veins have variable appearances. Straight, Serpiginous (crazy), multiple, single
It is a remnant of fetal circulation.
It is located in the ligamentum teres.
It courses from the umbilicus to the anterior left portal vein.
It normally measures <3 mm.
What happens to hepatic artery inflow in portal hypertension?
How can the hepatic artery appear in PHTN? - as a compensatory reaction.
Hepatic artery inflow increases substantially as a compensatory reaction.
It may become enlarged and tortuous. a compensatory reaction.
Can the hepatic artery fully compensate for the loss of portal flow?
No. It cannot adequately compensate for the loss of portal flow.
Normally, the liver gets about:
70% of its blood from the portal vein
30% from the hepatic artery
With portal hypertension, less blood reaches the liver through the portal vein. The hepatic artery tries to help by sending more blood than normal. This is called a compensatory reaction.
Because it is carrying extra blood, the hepatic artery may become:
Enlarged = wider
Tortuous = more twisted or winding
However, the hepatic artery cannot completely replace all the blood lost from the portal vein, so the liver may still not receive enough total blood.
Think of two water pipes supplying a building: the large pipe loses flow, so the smaller pipe opens wider and works harder—but it still cannot supply everything by itself.
List the 3 hepatic vein effects of PHTN
Extrinsic compression with loss of pulsatility
Size may not change with respiration