Chapter 34- Acute Renal Injury and Chronic Kidney Disease
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
20 Terms
Which of the following data would a clinician consider as most indicative of acute renal failure?
A) Alterations in blood pH; peripheral edema
B) Increased nitrogenous waste levels; decreased glomerular filtration rate (GFR)
C) Decreased serum creatinine and blood urea nitrogen (BUN); decreased potassium and calcium levels
D) Decreased urine output; hematuria; increased GFR
B) Increased nitrogenous waste levels; decreased glomerular filtration rate (GFR)
Feedback: The hallmark of acute renal injury is azotemia, an accumulation of nitrogenous wastes such as creatinine, urea nitrogen, and uric acid, plus a decrease in the GFR of the kidneys. While pH alterations, edema, electrolyte imbalances, and decreased urine output may accompany acute renal failure, they are all potentially attributable to other pathologies. Creatinine, GFR, and BUN would unlikely rise during renal failure.
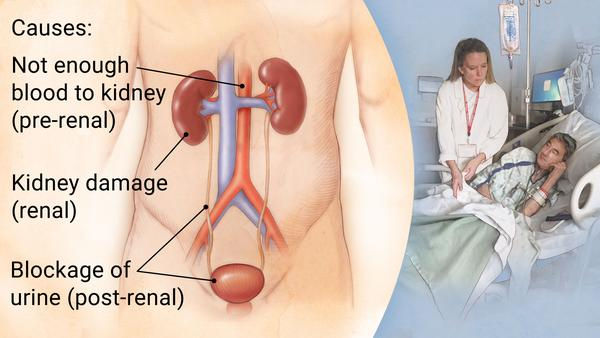
Which of the following clients would be considered to have a significant risk of developing the prerenal form of acute renal failure? Select all that apply.
A) A 22-year-old male who has lost large amounts of blood following a workplace injury
B) A 41-year-old female who is admitted for intravenous antibiotic treatment of pyelonephritis
C) A 79-year-old male with diagnoses of poorly controlled diabetes mellitus and heart failure
D) A 20-year-old male who is admitted for treatment of an overdose of a nephrotoxic drug
E) A 68-year-old male with a diagnosis of benign prostatic hyperplasia (BPH)
F) An 80-year-old female who has been admitted for the treatment of dehydration and malnutrition
A) A 22-year-old male who has lost large amounts of blood following a workplace injury
C) A 79-year-old male with diagnoses of poorly controlled diabetes mellitus and heart failure
F) An 80-year-old female who has been admitted for the treatment of dehydration and malnutrition
Feedback: Hemorrhage, heart failure, and dehydration (hypovolemia) are all noted contributors to prerenal failure. Pyelonephritis and damage from nephrotoxic drugs would more likely result in intrinsic renal failure, while BPH is postrenal in nature.

The clinical nurse educator on a nephrology unit of a large, urban hospital is orientating recent nursing graduates to the unit. Which of the following teaching points about acute tubular necrosis (ATN) should the educator include in the orientation session?
A) “The cardinal signs of ATN are oliguria and retention of potassium, creatinine, and sulfates.”
B) “Ureteral and bladder outlet obstructions are often contributors to ATN.”
C) “Trauma, burns, and major surgery are common precursors to ATN.”
D) “Tubular epithelial cells are sensitive to ischemia and toxins, and damage is irreversible.”
C) “Trauma, burns, and major surgery are common precursors to ATN.”
Feedback: ATN is often preceded by major surgery, burns, or trauma. Many cases of ATN are nonoliguric, and obstructions that are postrenal in nature are not common causes of ATN. Damage to tubular epithelial cells is not necessarily irreversible.

Which of the following patients scheduled for an interventional radiology procedure requiring administration of radiocontrast dye would be considered at high risk for nephrotoxicity? Select all that apply.
A) A 14-year-old with severe abdominal pain
B) A 25-year-old with a history of glomerular nephritis who is complaining of severe flank pain
C) A 67-year-old diabetic undergoing diagnostic testing for new-onset proteinuria
D) A 45-year-old with elevated liver enzymes possibly due to fatty liver cirrhosis
E) A 53-year-old male undergoing biopsy for a suspicious “spot” on his chest x-ray
B) A 25-year-old with a history of glomerular nephritis who is complaining of severe flank pain
C) A 67-year-old diabetic undergoing diagnostic testing for new-onset proteinuria
Feedback: Radiocontrast media-induced nephrotoxicity is thought to result from direct tubular toxicity and renal ischemia. The risk for renal damage caused by radiocontrast media is greatest in older adults and those with preexisting kidney disease, volume depletion, diabetes mellitus, and recent exposure to other nephrotoxic agents.

A 35-year-old female ultramarathon runner is admitted to the hospital following a day-long, 50-mile race because her urinary volume is drastically decreased and her urine is dark red. Tests indicate that she is in the initiating phase of acute tubular necrosis. Why is her urine red?
A) Hematuria
B) Hemoglobinuria
C) Myoglobinuria
D) Kidney bleeding
C) Myoglobinuria
Feedback: Myoglobinuria, which can cause acute tubular necrosis via intratubular obstruction, involves the leaching of myoglobin from skeletal muscle into the urine, bypassing the usual filtration by the glomerulus. Excess exercise and muscle trauma can contribute to this. While both hemoglobinuria and myoglobinuria discolor the urine, hemoglobinuria results from hemolysis following a reaction to a blood transfusion, whereas myoglobinuria involves muscle damage.
Following the diagnosis of acute renal failure, the nurse knows that one of the earliest manifestations of residual tubular damage is which of the following lab/diagnostic results?
A) Elevated blood urea nitrogen (BUN)
B) Serum creatinine elevation
C) Inability to concentrate urine
D) Reduced glomerular filtration rate
A) Elevated blood urea nitrogen (BUN)
Feedback: Urine tests that measure urine osmolality, urinary sodium concentration, and fractional excretion of sodium help differentiate prerenal azotemia, in which the reabsorptive capacity of the tubular cells is maintained, from tubular necrosis, in which these functions are lost. One of the earliest manifestations of tubular damage is the inability to concentrate urine. Conventional markers of serum creatinine and urea nitrogen, fractional secretion of sodium to assess glomerular filtration rate (GFR), and urine output do not manifest for 1 to 2 days after the acute renal failure has begun.

A family physician is providing care for a 61-year-old obese male who has a history of diabetes and hypertension. Blood work has indicated that the man has a GFR of 51 mL/minute with elevated serum creatinine levels. Which of the following statements will the physician most likely provide the client in light of these results?
A) “We will regularly monitor your kidney function, but most likely your kidneys will be able to compensate on their own and intervention is not required.”
B) “You likely have chronic kidney disease, and there may be urine in your blood until it is controlled.”
C) “Your chronic kidney disease has likely been caused by your diabetes and high blood pressure.”
D) “You're in kidney failure, and I'll be starting dialysis treatment
immediately.”
C) “Your chronic kidney disease has likely been caused by your diabetes and high blood pressure.”
Feedback: Diabetes and hypertension are conditions that can cause chronic kidney disease (CKD). While the kidneys do have a remarkable ability to compensate for impaired function, this fact does not mean that treatment would not be undertaken. Hematuria is not a common manifestation of CKD, and the client's GFR of 51 mL/minute does not indicate kidney failure or the need for dialysis.

A nurse is collecting a urine specimen prior to measuring the albumin level in a client’s urine. A colleague questions the rationale for the test, stating, “I thought albumin was related to liver function, not kidney function.” How can the nurse best respond to this statement?
A) “Urine should normally be free of any proteins, and albumin is one of the more common proteins to be excreted in chronic renal failure.”
B) “Urine albumin levels are useful for diagnosing diabetic kidney disease.”
C) “A urine dipstick test will tell us exactly how much albumin is being spilled by the client's kidneys.”
D) “A urine test for albumin allows us to estimate the client's GFR quite accurately.”
B) “Urine albumin levels are useful for diagnosing diabetic kidney disease.”
Feedback: In clients with diabetes, albumin tests are useful adjunctive test of nephron injury and repair. Urine is not normally completely free of proteins, and a urine dipstick does not allow for the quantification of how much albumin is in a sample. Albumin tests do not allow for an accurate indirect indication of GFR.
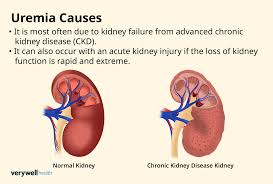
Which of the following clinical manifestations would lead the nurse to suspect the renal failure patient is developing uremia? Select all that apply.
A) Weakness and fatigue
B) Lethargy and confusion
C) Extreme itching
D) Blood in urine
E) Urine smell in the stool
A) Weakness and fatigue
B) Lethargy and confusion
C) Extreme itching
Feedback: Uremia affects all body systems. The symptoms at the onset include weakness, fatigue, nausea, and apathy. These are subtle signs. More severe symptoms include extreme weakness, frequent vomiting, lethargy, and confusion.
A hospital client with a diagnosis of chronic renal failure has orders for measurement of her serum electrolyte levels three times per week. Which of the following statements best captures the relationship between renal failure and sodium regulation?
A) Clients with advanced renal failure are prone to hyponatremia because of impaired tubular reabsorption.
B) Renal clients often require a sodium-restricted diet to minimize the excretion load on remaining nephrons.
C) Clients with renal failure often maintain high sodium levels because of decreased excretion.
D) Restricting sodium intake helps to preserve nephron function and has the additional benefit of lowering blood pressure.
A) Clients with advanced renal failure are prone to hyponatremia because of impaired tubular reabsorption.
Feedback: The compromised ability of the tubular nephrons to reabsorb sodium predisposes renal clients to low serum sodium levels. A sodium restriction is thus not normally indicated.
Which of the following clients' diagnostic blood work is most suggestive of chronic kidney disease (CKD)?
A) A client with high pH; low levels of calcium; and low levels of phosphate
B) A client with low vitamin D levels; low calcitriol levels; and elevated parathyroid hormone (PTH) levels
C) A client with low bone density; low levels of calcium; and low levels of phosphate
D) A client with low potassium levels; low calcitriol levels; and increased PTH levels
B) A client with low vitamin D levels; low calcitriol levels; and elevated parathyroid hormone (PTH) levels
Feedback: CKD is associated with low vitamin D and calcitriol levels, which induces increased PTH production. CKD is also associated with acidosis (low pH), high levels of phosphate, and hyperkalemia.
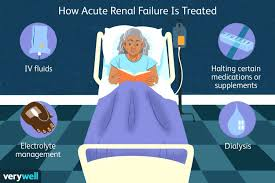
Which of the following medications would the nurse anticipate being prescribed for the renal failure patient who has hyperphosphatemia?
A) Vitamin D (calcitriol)
B) Calcium carbonate
C) Levothyroxine (Synthroid)
D) Sensipar (Cinacalcet)
B) Calcium carbonate
Feedback: Phosphate-binding antacids (aluminum salts, calcium carbonate, or calcium acetate) may be prescribed to decrease the absorption of phosphate from the GI tract.
To maintain hematocrit levels in people with kidney failure, the nurse should be prepared to
A) arrange for frequent blood transfusions in an outpatient clinic.
B) administer iron dextran intravenously.
C) administer a subcutaneous injection of recombinant human erythropoietin (rhEPO).
D) administer prenatal vitamins twice a day.
C) administer a subcutaneous injection of recombinant human erythropoietin (rhEPO
Feedback: Recombinant human erythropoietin (rhEPO) helps maintain hematocrit levels in people with kidney failure. Secondary benefits include improvement in appetite, energy level, sexual function, skin color, and hair and nail growth, and reduced cold intolerance. Blood transfusion is a treatment if symptomatic with low hemoglobin; however, they try to prevent this by giving EPO or IV iron dextran if there is severe iron deficiency anemia. Prenatal vitamins are high in vitamins but not helpful to renal failure patients.

A nurse educator is performing client education with a 51-year-old man who has been recently diagnosed with chronic kidney disease. Which of the following statements by the client would the nurse most likely want to correct or clarify?
A) “I'll be prone to anemia, since I'm not producing as much of the hormone that causes my bones to produce red blood cells.”
B) “My heart rate might go up because of my kidney disease, and my blood might be a lot thinner than it should be.”
C) “My kidney problems increase my chance of developing high blood pressure or diabetes.”
D) “I'll have a risk of either bleeding too easily or possibly clotting too quickly, though dialysis can help minimize these effects.”
C) “My kidney problems increase my chance of developing high blood pressure or diabetes.”
Feedback: While high blood pressure can be causative of, or consequent to, renal failure, diabetes is not normally a result of existing CKD. Persons with renal failure are indeed prone to anemia, increased heart rate, decreased blood viscosity, and coagulopathies. The risk of bleeding and thrombotic disorders can be partially mitigated by dialysis.
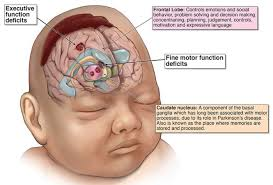
The nurse assessing a renal failure patient for encephalopathy caused by high uremic levels may observe which of the following clinical manifestations?
A) Severe chest pain with pericardial friction rub on auscultation
B) Stiff immobile joints and contractures
C) Loss of recent memory and inattention
D) Pruritus with yellow hue to skin tone
C) Loss of recent memory and inattention
Feedback: Reductions in alertness and awareness are the earliest and most significant indications of uremic encephalopathy. These often are followed by an inability to fix attention, loss of recent memory, and perceptual errors in identifying people and objects. Answer choice A refers to pericarditis; answer choice B refers to arthritis; answer choice D refers to liver involvement.

Which of the following phenomena contributes to the difficulties with absorption, distribution, and elimination of drugs that are associated with kidney disease?
A) Reductions in plasma proteins increase the amount of free drug and decrease the amount of protein-bound drug.
B) Acute tubular necrosis is associated with impaired drug reabsorption through the tubular epithelium.
C) Decreased retention by the kidneys often renders normal drug dosages ineffective.
D) Dialysis removes active metabolites from circulation minimizing therapeutic effect.
A) Reductions in plasma proteins increase the amount of free drug and decrease the amount of protein-bound drug.
Feedback: A decrease in plasma proteins, particularly albumin, that occurs in many persons with renal failure results in less protein-bound drug and greater amounts of free drug. Drug elimination problems do not stem as directly from impaired tubular reabsorption, decreased retention, or the process of dialysis.

A 42-year-old male has been diagnosed with renal failure secondary to diabetes mellitus and is scheduled to begin dialysis soon. Which of the following statements by the client reflects an accurate understanding of the process of hemodialysis?
A) “It's stressful knowing that committing to dialysis means I can't qualify for a kidney transplant.”
B) “I know I'll have to go to a hospital or dialysis center for treatment.”
C) “Changing my schedule to accommodate 3 or 4 hours of hemodialysis each day will be difficult.”
D) “I won't be able to go about my normal routine during treatment.”
D) “I won't be able to go about my normal routine during
treatment.
Feedback: Hemodialysis requires the client to remain connected to dialysis machinery, whereas peritoneal dialysis allows for activity during treatment. Dialysis does not disqualify an individual from receiving a transplant. Dialysis does not require attendance at a dialysis center, and patients can be taught to perform the dialysis in their home with a family member in attendance. Hemodialysis is normally conducted three times weekly, not once per day.

Following kidney transplantation, the patient is prescribed maintenance immunosuppressive therapy consisting of prednisone, azathioprine, and cyclosporine. Educating the patient about long-term maintenance on immunosuppressive therapy should include discussion of side effects that may include: (Select all that apply).
A) cardiovascular complications.
B) increased risk of developing cancer.
C) nephrotoxicity of a newly transplanted kidney.
D) development of moon face and buffalo hump.
E) ringing or buzzing of the ears.
A) cardiovascular complications.
B) increased risk of developing cancer
Feedback: Mostly all immunosuppressive drugs have serious side effects such as CV complications, metabolic dysfunction, and cancer. Rarely do these medications harm the newly transplanted kidney. Distracter D lists classic s/s of Cushing syndrome. Ringing or buzzing of the ears can be associated with ibuprofen intake

A 1-year-old baby boy with renal dysplasia risks end-stage renal disease unless intervention occurs. Which of the following treatment options is his care team most likely to reject?
A) Dietary restriction plus erythropoietin
B) Continuous cyclic peritoneal dialysis
C) Renal transplantation
D) Continuous ambulatory peritoneal dialysis Ans: A
A) Dietary restriction plus erythropoietin
Feedback: Renal transplantation and dialysis are recommended for children; of these, transplantation is the preferred treatment. Conservative measures are inappropriate in this age group because of the importance of fostering proper bone growth, especially in the first 2 years, and appropriate cognitive development, which is at risk due to issues such as uremic encephalopathy and the effect of renal failure upon the central nervous system of the developing child.

Which of the following clinical findings among older adults is most unlikely to warrant further investigation and possible treatment?
A) An 81-year-old male's serum creatinine level has increased sharply since his last blood work.
B) A 78-year-old female's GFR has been steadily declining over several years.
C) A 90-year-old female's blood urea nitrogen (BUN) is rising.
D) An 80-year-old male whose urine dipstick reveals protein is present.
B) A 78-year-old female's GFR has been steadily declining over several years.
Feedback: A gradual decrease in GFR is considered a normal age-related change. Increased creatinine or BUN would warrant follow-up, as would the presence of protein in a client's urine.