UNIT 3 EBSTEIN’S ANOMALY
1/77
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
78 Terms
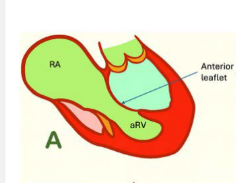
Ebstein’s anomaly is a rare congenital heart defect in which tricuspid valve leaflets are what towards where? producing variable degrees of what
Ebstein’s anomaly is a rare congenital heart defect in which the septal and posterior tricuspid valve leaflets are displaced toward the apex. producing variable degrees heart failure
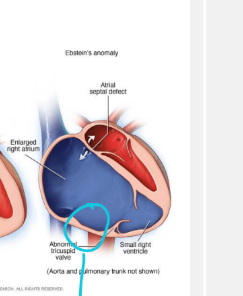
The septal and posterior tricuspid valve leaflets are displaced toward the apex, leading to annular what and causes part of the right ventricle to become what? And creates what of the RV list 2
leading to annular displacement, This causes part of the right ventricle to become atrialized, producing RV dilation and dysfunction
In Ebsteins’s anomaly which tricuspid valve leaflet is often redundant?
This deformation leads to a rotational displacement of the tricuspid valve into where? causing a variable degrees of what?
The anterior tricuspid valve leaflet is often redundant
and may rotate toward the RVOT, causing varying degrees of right ventricular outflow tract obstruction.
Redundant anterior tricuspid leaflet = big floppy extra leaflet tissue.
List the 4 factors that determine the severity of Ebstein’s anomaly.
Degree of tricuspid valve displacement
Degree of RV atrialization
Degree of RVOT obstruction
Degree of ventricular dysfunction
List the 3 incidence facts about Ebstein’s anomaly.
It is a _ congenital malformation of the tricuspid valve
It occurs in approximately 1–_ per 200,000 live births
It is one of the 2 common what anomalies
It is a rare congenital malformation of the tricuspid valve
It occurs in approximately 1–5 per 200,000 live births
It is one of the 2 common tricuspid valve anomalies* (other is TV dysplasia)
List the 3 categories of causes and risk factors for Ebstein’s anomaly.
Maternal medications and teratogens**** HIghly assocaited
Genetics
Anatomical maldevelopment
Delaminate means the valve leaflet is supposed to separate/free itself from the RV wall during development.
But in Ebstein’s, it does not separate normally, so parts of the tricuspid valve stay stuck/tethered too low in the RV.
Anatomical maldevelopment in Ebstein’s means the tricuspid valve formed wrong because it failed to separate from the RV wall, making the valve sit too low and creating an atrialized portion of the RV.
List the 3 maternal medication or environmental exposures associated with Ebstein’s anomaly.
Lithium
Benzodiazepines
Varnish or chemical exposure
during what trimester of pregancy is this maternal medication exposure is the best-known environmental risk factor for Ebstein’s anomaly?
Exposure to lithium during the first trimester of pregnancy.
(people with bipolar disorder take this)
How are benzodiazepines and varnishing substances associated with Ebstein’s anomaly?
Maternal use of benzodiazepines has been statistically linked to a higher risk of developing this heart defect (People how have anxiety disorders take this)
Varnish/Chemical Exposure: Studies suggest an increased risk is associated with periconceptional maternal exposure to varnishing substances
List the a genetic factors associated with Ebstein’s anomaly.
Gene mutations
Explain the embryologic abnormality that causes Ebstein’s anomaly.
The tricuspid valve fails to properly what, from the which wall of the what chamber?
This causes one or more leaflets to become what? the which leaflet becomes long and sail-like and may spiral towards where?
The tricuspid valve fails to properly delaminate, or separate, from the inner wall of the right ventricle.
This causes one or more leaflets to become apically displaced. The anterior leaflet becomes long and sail-like and may spiral toward the RVOT.
Delaminate means the valve leaflet is supposed to separate/free itself from the RV wall during development.
But in Ebstein’s, it does not separate normally, so parts of the tricuspid valve stay stuck/tethered too low in the RV.
How does failed tricuspid valve delamination divide the right ventricle?
This causes the valve to sit too where, splitting the right ventricle into
two parts: list those two
This causes the valve to sit too low, splitting the right ventricle into
two parts:
It divides the RV into:
A thin atrialized upper portion
A smaller functional lower portion
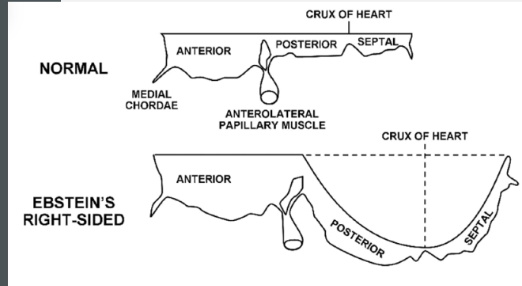
Apical displacement of the posterior and septal leaflets of the tricuspid valve ____from the what?
The anatomical what remains normally positioned, but the leaflet insertion is where and directed toward the where
List 3 descriptions of how the leaflets look?
Apical displacement of the posterior and septal leaflets of the tricuspid valve away from the annulus
The anatomical annulus remains normally positioned, but the leaflet insertion is lower and directed toward the RVOT.
The leaflets may be: (all creates TR)
Dysplastic
Thickened or rolled
Tethered
What region should be carefully examined to recognize leaflet displacement?
Look for the region from annulus to leaflet insertion
Hall mark finding:
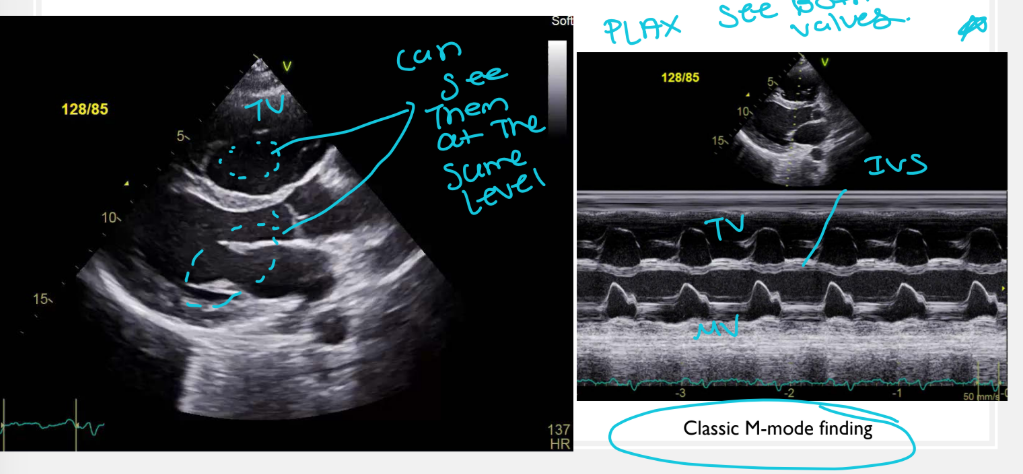
What unusual relationship between the tricuspid and mitral valves may be seen in Ebstein’s anomaly? & list 2 views we can this in?
The displaced tricuspid valve may appear at the same level as the mitral valve in PLAX and PSAX views.
Describe the anterior tricuspid leaflet in Ebstein’s anomaly.
The anterior leaflet remains attached to the normal ___ring but becomes: what list 3 things ?
it flaps in where? what does it resemble?
what can this cause of the RVOT?
The anterior leaflet remains attached to the normal valve ring but becomes:
Excessively large
Redundant
Hypermobile
It flaps in the RV and resembles a sail in the wind.
(becomes very long and can be sucked into the RVOT and cause obstruction)
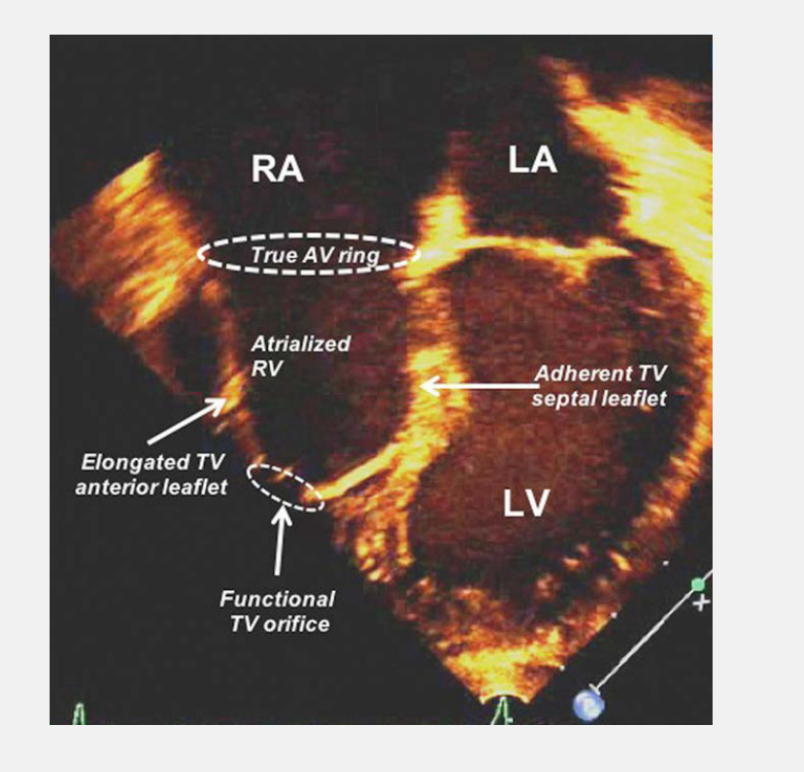
What is the atrialized right ventricle? - it is the what portion of the RV located between where?
The atrialized right ventricle is the inlet portion of the RV located between the true tricuspid annulus and the functional annulus.

List the 3 characteristics of the atrialized RV.
It progressively dilates because of tricuspid regurgitation
It acts as a thin-walled reservoir with no myocardium
no contractility
Think of a reservoir like a storage tank.
It holds blood, but it doesn't pump it.
What is the functional right ventricle? & It consists which portions of the RV list 2 ?
The functional RV is the smaller but functioning part of the RV. It consists of the:
Trabeculated portion
Outlet portion
List the 2 hallmark right-sided findings in Ebstein’s anomaly.
Severe RA dilation is common and a hallmark finding**
Tricuspid regurgitation
Why does tricuspid regurgitation occur?
The tricuspid leaflets are thickened, tethered, displaced, and unable to close normally.
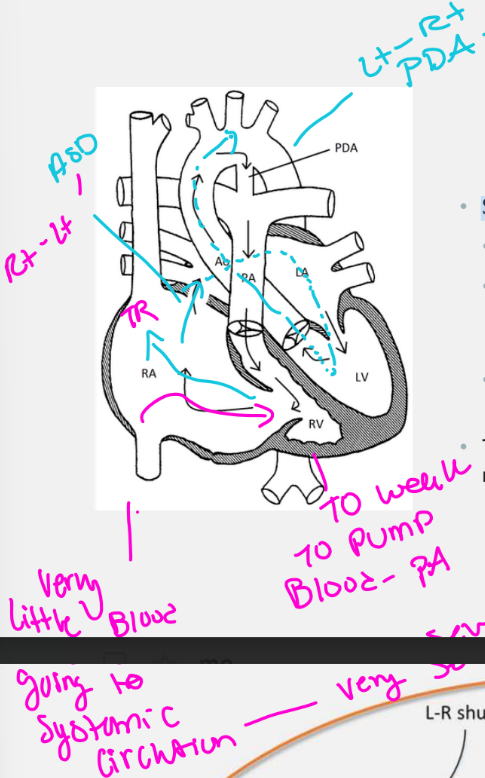
What atrial communication is commonly present in Ebstein’s anomaly, and what is the usual shunt direction?**
An ASD or PFO is present in approximately 50–70% of patients and may produce right-to-left shunting.
What clinical effect can result from right-to-left atrial shunting?
Deoxygenated blood enters the systemic circulation, causing cyanosis.
Why are arrhythmias common in Ebstein’s anomaly?
What disrupts the normal AV-node and electrical pathway anatomy, increasing the risk of abnormal conduction and arrhythmias?
Displacement of the septal tricuspid leaflet disrupts the normal AV-node and electrical pathway anatomy, increasing the risk of abnormal conduction and arrhythmias.
Explain how severe right-heart enlargement affects the left ventricle. and list 3 things it can produces?
Dilation of the atrialized RV causes the interventricular septum to bow toward the LV. This produces:
Diastolic septal flattening from RV volume overload in diastole
A banana-shaped LV (LV compressed by the RV)
Reduced LV cavity volume
Explain how severe Ebstein’s anomaly can cause functional pulmonary atresia.
The functional RV may be unable to generate enough pressure to open a structurally normal pulmonary valve. Therefore, little or no antegrade flow crosses the pulmonary valve.
What supplies pulmonary blood flow when functional pulmonary atresia is present?
Pulmonary blood flow becomes ductal-dependent and is supplied through the PDA.
effectively “stealing” blood from the systemic circulation
Systemic circulation = blood going to the body through the aorta.
Stealing = blood leaves the aorta/body pathway and goes through the PDA to the lungs.
List the 3 findings that can further decrease forward pulmonary flow.
Severe pulmonary valve insufficiency, which leads to regurgitation and further reduces forward flow
RVOT obstruction caused by the elongated anterior tricuspid leaflet
List the 3 main methods used to classify the severity of Ebstein’s anomaly.
& which is the primary quantitative measurement used to diagnose Ebstein's anomaly?
These systems help determine what list 2
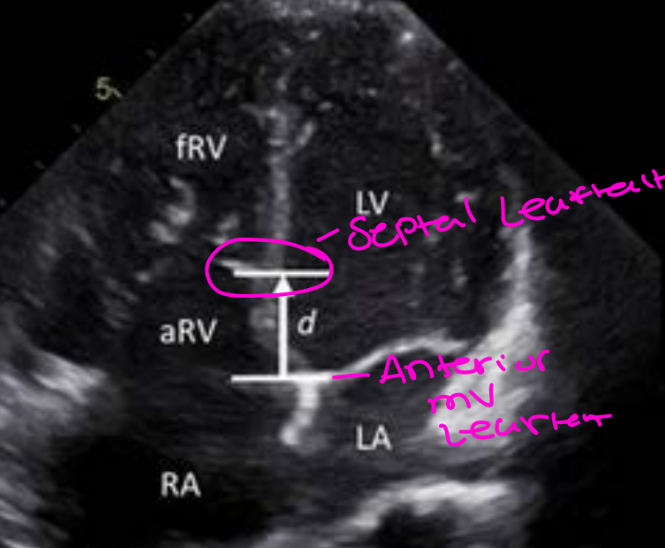
Apical displacement index (ADI) is the primary quantitative measurement used to diagnose Ebstein's anomaly
Carpentier classification (based on anatomy)
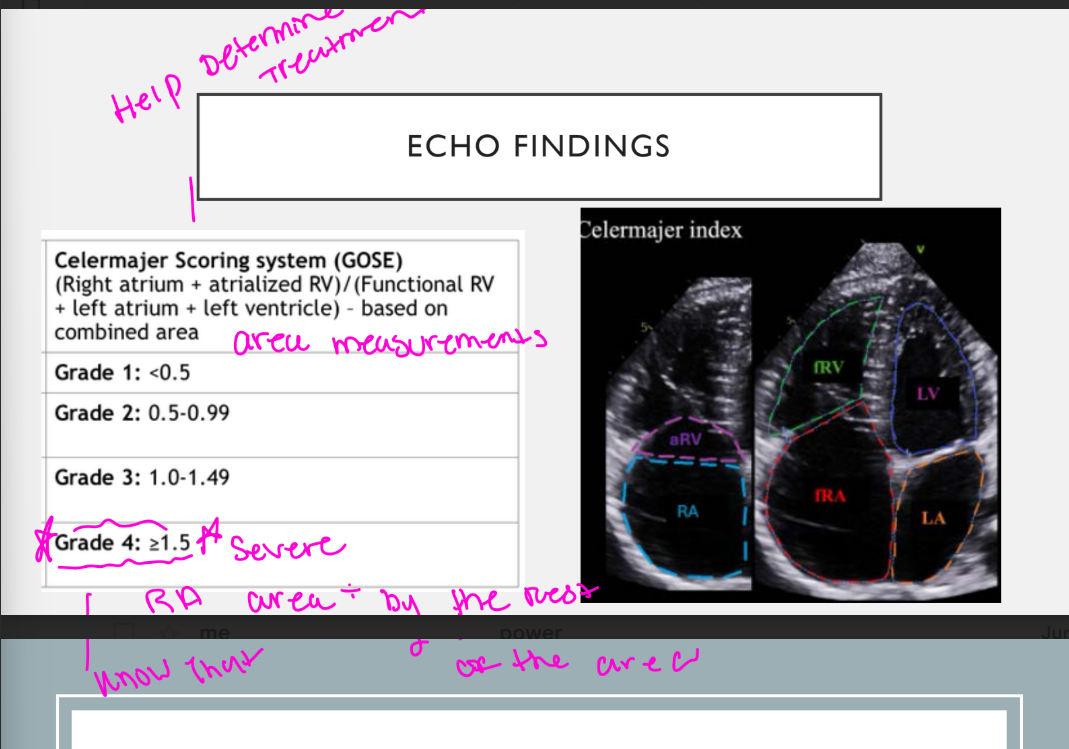
Celermajer index (based on echocardiographic chamber size ratios).
These systems help determine prognosis and guide surgical intervention
What does the apical displacement index measure?
It measures the displacement between:
Measuring the distance between the hinge point of the anterior mitral valve leaflet
^ & The displaced hinge point of the septal tricuspid valve leaflet
The distance is then divided by the patient’s body surface area.
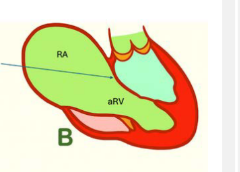
List the 3 findings of Carpentier Type A Ebstein’s anomaly.
Is this Mild, Moderate, or severe apical displacement of the septal and posterior leaflets?
What is the size of the atrialized RV for Type A?
How is the function of the RV
Mild apical displacement of the septal and posterior leaflets
Small atrialized RV
Adequate functional RV function
List the 3 findings of Carpentier Type B Ebstein’s anomaly.
Is this Mild, Moderate, or severe apical displacement of the septal and posterior leaflets?
What is the size of the atrialized ventricle & function?
How is the volume, and how is the function of the functional right ventricle
Moderate apical displacement
Moderately enlarged atrialized RV with reduced function
Reduced functional RV volume but adequate function
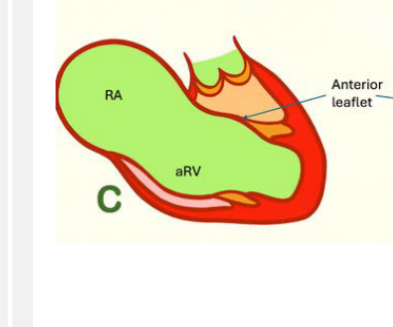
List the 4 findings of Carpentier Type C Ebstein’s anomaly.
Is this Mild, Moderate, or severe apical displacement of the septal and posterior leaflets?
How does Type C obstruct and what does it Obstruct
what is the size of the "atrialized" ventricle with what function
whats the functional RV function?
Severe apical displacement
Abnormal attachments that restrict anterior leaflet mobility, potentially RVOT obstruction
• large "atrialized" ventricle with reduced function
• small functional right ventricle
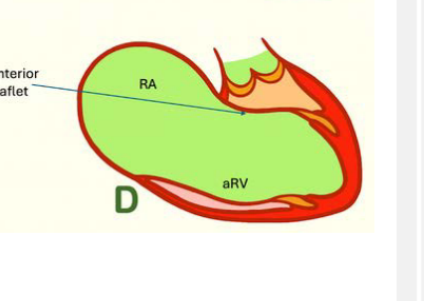
List the 3 findings of Carpentier Type D Ebstein’s anomaly.
How is this type classified?
What happened with the tricuspid valve leaflets
What is the size of the "atrialization" of the right ventricle, this type has a exception of a small insuffucuent with what component?
Extensive (tricuspid valve sac)
Complete failure of tricuspid leaflet delamination
Almost complete "atrialization" of the right ventricle with the exception of a small insufficient infundibular component
Complete non-delamination means the valve leaflets did not separate/free themselves from the inside wall of the RV at all during development.
Type D = the TV is basically stuck down into the RV like a sac, so almost the whole RV acts like atrium instead of a pumping ventricle.
Atrialized RV = upper RV, acts like atrium/reservoir, poor contraction.
Functional RV = lower RV, still acts like ventricle, pumps to lungs.
The more atrialized RV there is, the smaller the functional RV becomes, so the patient can have worse right-sided heart function.
GOSE SCORE: Celermajer index
whats the formula and what is Grade 4 value?
Grade 4 greater then or equal to 1.5 (massively atrialized RV)
Celermajer index (based on echocardiographic
chamber size ratios).
List the 4 factors that determine the physiology of Ebstein’s anomaly.
Degree of valve displacement
Degree of RV atrialization
RVOT obstruction
RV dysfunction
The degree of RV atrialization dictates the amount of what about the RV List 2?
A what size atrialized right ventricle is unable to generate enough what to exceed the what?
The greater the atrialized portion, the more severe the RV dilation and dysfunction.
A severely atrialized right ventricle is unable to generate enough pressure to exceed the pulmonary artery pressure.
<
Is the pulmonary valve normal? what flaw does it have due to this^?
Where will the Lungs reveive blood from ?
• The pulmonary valve is normal but does not open well
• The lungs will receive blood from the PDA
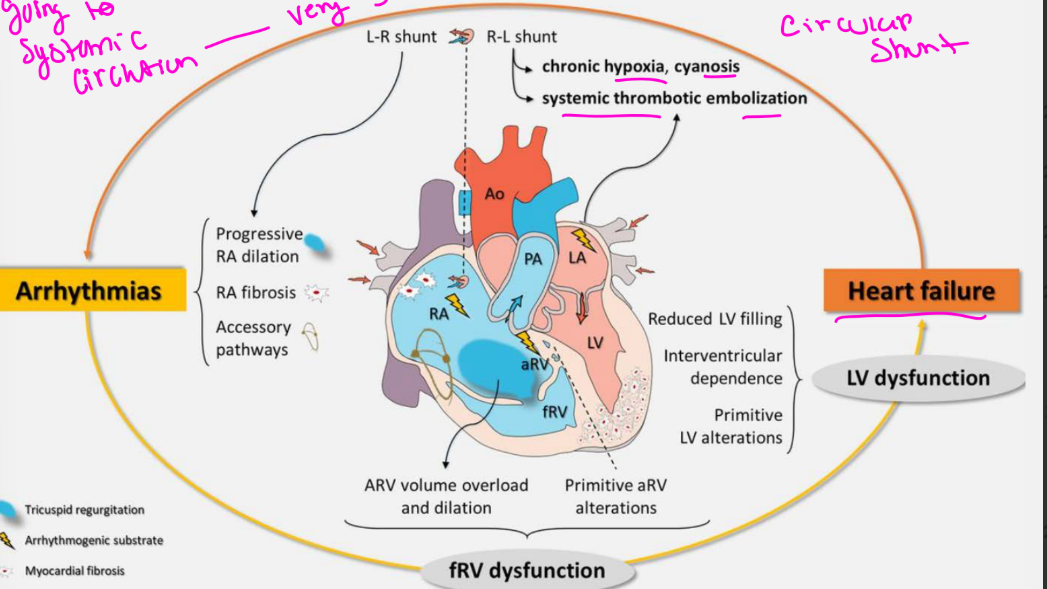
Severe Ebstein’s demonstrates what shunt physiology?
Severe Ebstein’s demonstrates circular shunt physiology (D-TGA)
Explain circular shunt physiology in severe Ebstein’s anomaly.
Severe TR directs blood into the right atrium
(TR) Blood travels right-to-left through the ASD
Blood moves forward (antegrade) through the LVOT and aorta
Blood travels backward (retrograde) through the PDA into the pulmonary artery
Severe pulmonary regurgitation sends blood back into the RV
Severe Ebstein’s demonstrates circular shunt physiology:
This circular shunt may lead to what in utero or neonatally and carries a very what outcome?
This circular shunt may lead to rapid deterioration in utero or neonatally and carries a very poor outcome ( Chronic hypoxia, cyanosis, systemic thrombotic embolization, HF)
When can Ebstein’s anomaly first present? & what is it depending on?
Presentation can occur from the prenatal period through late adulthood, depending on severity.
How may mild Ebstein’s anomaly present? & when might this be disgnosed?
Patients may be asymptomatic and may not be diagnosed until adulthood.
List the 7 common clinical signs and symptoms of Ebstein’s anomaly.
Murmur
Split second heart sound
Holosystolic murmur from TR
Systolic ejection murmur from RVOT obstruction
Cyanosis (circular shunt physiology)
Clubbing of the digits (circular shunt physiology)
Dyspnea on exertion
List the 2 rare signs of advanced right-sided congestion.
Hepatomegaly
Jugular venous distention
What chest X-ray finding is associated with Ebstein’s anomaly? & what is the nickname this is called on X-ray imaging?
Cardiomegaly with a severely enlarged right atrium, producing a large box-shaped heart.
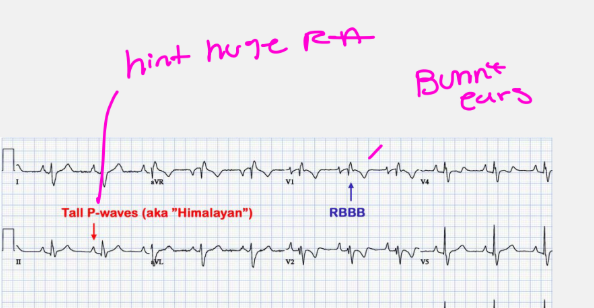
List the 2 ECG or rhythm findings associated with Ebstein’s anomaly. The most common ones!
Wolff-Parkinson-White syndrome in approximately 30%**
Right bundle branch block in approximately 90%** (the bunny ears)
(Pre-excitation, Tall P waves from RA enlargement, called Himalayan P waves, Prolonged PR interval, & Atrial fibrillation or atrial flutter)
List the 3 common associated defects of Ebstein’s anomaly.
ASD or PFO********
PDA
What Type of shunt causes cyanosis?
Right to left shunt causing cyanosis (ASD/PFO)
List the 3 common associated defects of Ebstein’s anomaly. for a PDA
Pulmonary valve stenosis
Pulmonary atresia
Pulmonary artery hypoplasia
PDA:
What causes functional pulmonary atresia?
How can the leaflets also cause obstruction?
What leads to pulmonary artery hypoplasia?
RV is so small it causes functional pulmonary atresia
The displaced leaflet can also cause obstruction
Lack of pressure to open the PV may also lead to pulmonary artery hypoplasia
List the number 1 and 2nd additional congenital heart conditions associated with Ebstein’s anomaly.
Number 1 . Congenitally corrected transposition of the great arteries*
2nd Left ventricular noncompaction (LVNC)
ECHO FINDINGS for Ebstein’s anomaly:
List the 2 assessment goals from the subcostal four-chamber view.
Interrogate the atrial septum for what list 2, with 2D, color, & Doppler
How do you estimate the RAP?
Interrogate the atrial septum for a PFO or secundum ASD with 2D and color Doppler (Determine shunt direction)
Assess the IVC to estimate right atrial pressure
List the 4 findings assessed from subcostal short-axis.
Interrogate the atrial septum for what shunts list 2
what severity should be assessed (hint remeber we are talking about Ebstein’s anomaly Think of the leaflets on that side)
What Valve should be Interrogated with 2D, Color PW, and CW?
What are some findings you may expect to find in this valve list 3 and what question should you ask yourself about the flow across this valve?
PFO or secundum ASD shunting
TR severity & Tricuspid stenosis severity
Interrogate Pulmonary valve with 2D, color, PW, and CW
• Pulmonary regurgitation, Obstruction, & PDA… Interrogate Pulmonary valve forward flow across the pulmonary valve
List the 3 PLAX findings associated with Ebstein’s anomaly.
Septal flattening from RV volume overload (in diastole)
Banana-shaped LV
Tricuspid and mitral valves appearing at the same level
What should be assessed in the PLAX RV inflow view? List 3
Sweep through the tricuspid leaflets to evaluate:
Leaflet morphology
Level of attachment
Tricuspid regurgitation
List the 5 findings assessed at the PSAX great-vessel level.
Look at the IAS for what shunt list two?
List two severity you should look for?
What function should evaluated?
What valve should you Interrogate with 2D, color, PW, and CW?
What are some findings you may expect to find in this valve list 3 and what question should you ask yourself about the flow across this valve?
IAS for PFO or secundum ASD shunt
TR severity & Tricuspid stenosis severity
RV function
Interrogate Pulmonary valve with 2D, color, PW, and CW
Pulmonary regurgitation, Obstruction, & PDA… Interrogate Pulmonary valve forward flow across the pulmonary valve?
List the 3 findings assessed at the PSAX ventricular level.
RV function
Septal flattening
En face tricuspid valve anatomy
What is the best view for defining most features of Ebstein’s anomaly?***
The apical four-chamber view.
List the 7 Echo findings assessed from the apical four-chamber view.
List 3 sizes your looking at? List 2 severity’s you should look for? What should you Measure? What is happening to the IAS and this is something you should capture? What shunts are you looking for in the IAS with color doppler?
Assess Right atrial size, True RV & Atrialized RV
TR and tricuspid stenosis severity
Measure True tricuspid annulus
Rightward bowing of the atrial septum
PFO or secundum ASD with color Doppler
List the 4 measurements used to assess RV function in A4C?
Fractional area change (FAC%)
TAPSE
S′ tissue Doppler velocity
Tei index (RIMP & LIMP)
What additional findings should be assessed from the apical view?
(what should you capture of the IVS? interroagte leaflet what?)
Interventricular septal flattening
Tricuspid leaflet tethering
What should be interrogated from the suprasternal notch view? (SSN)
PDA interrogation
List the 5 measurements or calculations performed during echo assessment.
Displacement index (In A4C)
Carpentier classification (In A4C)
Celermajer index (In A4C)
Qp:Qs
RVSP
Displacement Index:
In what view should this done in? and during when in the cardiac cycle?
Displacement of the what hinge of the which leaflet in what view?
Measure the distance from the insertion of the what leaflet to the insertion point of which leaflet in what cardiac cycle? this = what?
In the apical four-chamber view during systole, measure from:
Measure the distance from the insertion of the
anterior mitral valve leaflet to the insertion point of
the septal tricuspid leaflet in systole = displacement
distance
What displacement measurements support Ebstein’s anomaly:*****
Diameter measurement in adult?
Diameter measurement in peds?
Next step is to take this measurement and divide by the what and = displacement index what value support Ebstein’s anomaly in this step?
Adults: greater than 20 mm or 2.0cm
Pediatric patients: greater than 15 mm or 1.5 cm
Displacement index: greater than 8 mm/m² after dividing by BSA
List the 3 differentials for Ebstein’s anomaly.
Uhl’s anomaly**** (this Type creates a massive RT heart)
Tricuspid atresia
Arrhythmogenic right ventricular dysplasia (adult condition)
List the 3 medical management categories for Ebstein’s anomaly.
Heart failure treatment
Arrhythmia treatment (: Medicines may be prescribed to control rapid or irregular heartbeats like WPW & RBBB)
Infective endocarditis Antibiotic prophylaxis
List the 3 medications used to manage heart failure symptoms.
These are used to manage what retention, reduce the what on the heart, and relieve what.
Diuretics
ACE inhibitors
Digoxin
These are used to manage fluid retention, reduce
the workload on the heart, and relieve cyanosis.
What catheter-based procedure may be used to treat arrhythmias in Ebstein’s anomaly?
This minimally invasive procedure is often used to treat accessory electrical pathways (such as in which one) that cause rapid, abnormal heart rhythms
Radiofrequency ablation may be used to eliminate accessory electrical pathways, including pathways associated with WPW syndrome.
List the 4 surgical interventions for Ebstein’s anomaly. Which surgical interventions is preferred?
Cone procedure - preferred with Right atrial reduction, and ASD closure and RV plication
Tricuspid valve replacement
Permanent pacemaker placement
BT shunt (Blalock–Taussig shunt) followed by the Starnes procedure or Fontan pathway
RV plication means the surgeon folds and stitches part of the enlarged or poorly functioning right ventricle (RV) to make it smaller and improve its shape.
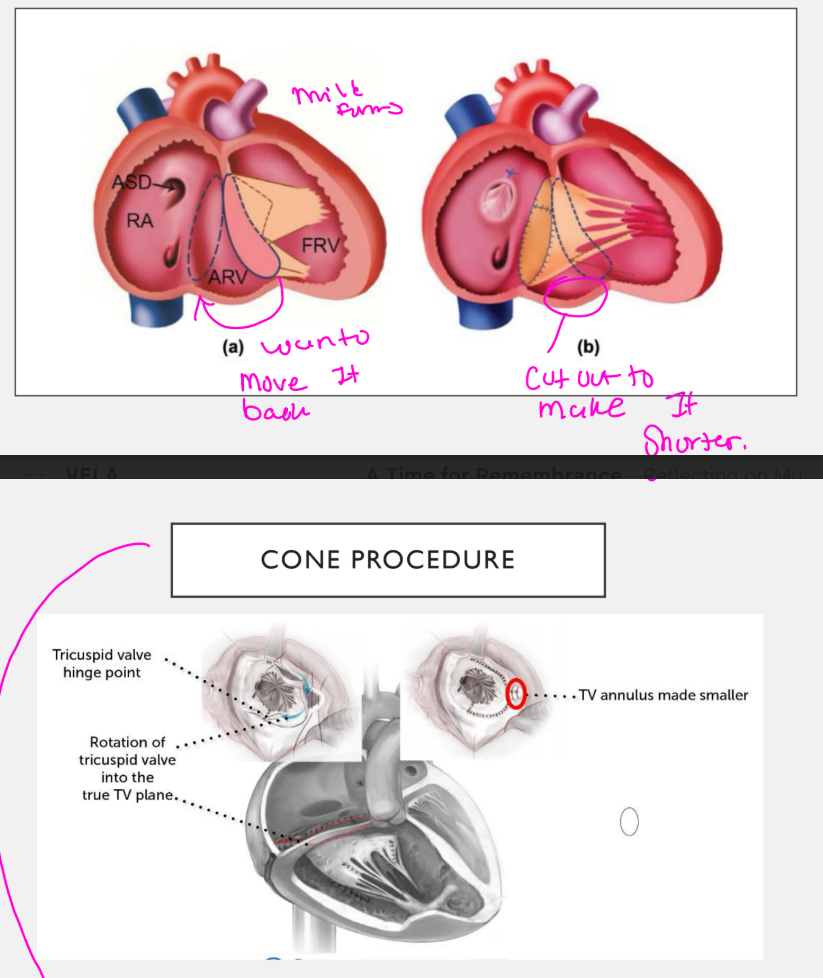
Why is the cone procedure preferred?
During a cone reconstruction, the surgeon is able to “artificially what” additional tricuspid valve tissue by dissecting the adherent components away from the underlying myocardium
During a cone reconstruction, the surgeon is able to “artificially delaminate” additional tricuspid valve tissue by dissecting the adherent components away from the underlying myocardium
Artificially delaminate means the surgeon carefully separates the tricuspid valve leaflet from the right ventricular wall.
In Ebstein’s anomaly, part of the valve leaflet is abnormally stuck to the RV muscle because it did not separate normally during development. During surgery, the surgeon cuts/frees that leaflet so it can move again and be reshaped into a functioning valve.
cone procedure:
Smaller leaflets are repaired with what material?
a what ring is attached
Leaflet tissue is sutured into a what
what happens to the atrialized portion of the right ventricle
what shunt is closed and excess/ redundant what is resected/removed
Smaller leaflets are repaired with Gore-Tex
An annuloplasty ring is attached
Leaflet tissue is sutured into a cone
The atrialized RV is plicated
The ASD is closed and excess right atrial tissue is removed
Plicated = folded and stitched down.
Atrialized RV plicated = the non-working stretched RV part is folded smaller so the heart shape/function improves.
When is the Starnes procedure used?
Starnes Procedure for circular shunt/severe Ebstein’s (Staged approach)
What is the purpose of the Starnes procedure:
It acts as a life-saving "____" by essentially taking the malformed ___side of
the heart out of what, allowing the ___side to do what?
It temporarily removes the malformed right side of the heart from circulation, allowing the left heart to recover.
The enlarged, poorly functioning RV remains inside the heart, but it is unloaded or “excluded” so it no longer receives a large amount of blood or pumps against the circulation. This allows it to shrink and reduces its pressure on the ventricular septum. The septum can move back toward normal, allowing the left ventricle to fill and pump better.
The Starnes procedure is used to stabilize the critically ill newborn. Later on,
once the right ventricle has what? Surgeons can "take down" the Starnes patch and perform a what repair to reconstruct which valve? Restoring what?
The Starnes procedure is used to stabilize the critically ill newborn. Later on,
once the right ventricle has shrunk and normalized in size, surgeons can "take
down" the Starnes patch and perform a Cone repair to reconstruct the
tricuspid valve, restoring normal two-ventricle blood flow
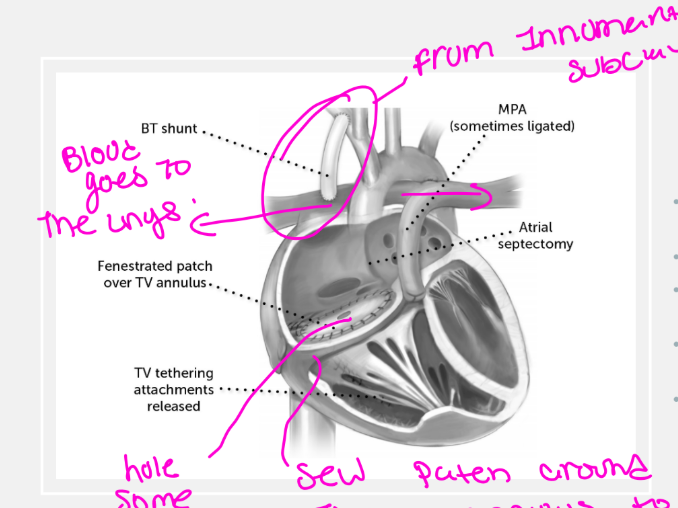
List the 5 components of the Starnes procedure.
what is placed over the true tricuspid annulus
what do they do to the RA?
What significantly improves LV preload
what do they do in cases of PR
what may be provided for pulmonary blood flow
Fenestrated patch placed over the true tricuspid annulus
Right atrial reduction plasty
Atrial septectomy to improve LV preload
Main pulmonary artery may be oversewn when severe pulmonary regurgitation is present
BT shunt or PDA stent provides pulmonary blood flow
List the 8 POST OP ECHO evaluation after Ebstein’s anomaly repair.
Tricuspid valve mobility
Tricuspid annulus size
Residual TR
RVSP
RV systolic function
(R/O) Tricuspid stenosis and its severity
(R/O) Pericardial effusion or thrombus
Pulmonary valve peak velocity and R/O obstruction
Residual PFO or ASD