HIP & PELVIS- POSITIONING NOTES & DEMO
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
pelvis nontrauma views
AP & FROG
pelvis trauma views
AP & BOTH OBLIQUES
Hip nontrauma views
AP & FROG
hip trauma views
AP & LATERAL
a cross table lateral should be obtained if….
obvious fracture is present on AP image or pt is unable to do frog
pelvis techniques
85 kVp, 12.5 mAs, outer cells
AP pelvis overview
Collimation- 17x14 CW
center to level of soft tissue depression (1.5”) above greater troch (bisect ASIS & symph)
top of light 1.5” above crest
MEDIALLY ROTATE LEGS IN 15-20 DEGREES to tuck the lesser
AP pelvis centering: on avg size patient scenter of IR is about…
2” inferior to ASIS & 2” superior to symph
sid & breathing for all pelvis & hip
40”
SUSPENDED RESPIRATION
AP pelvis evaluation criteria (for me to remember)
*Narrowed obturator foramina indicates rotation in that direction
*from crest to symph!!!
entire pelvis w/ proximal femora
sacrum & coccyx aligned w/ symph
greater in profile
AP pelvis, if lesser troch is visible it means
legs are not medially rotated in
AP pelvis, if rotated…
ala would be turned & obturator foramen will not be equal looking
AP pelvis additional note
proximal orthopedic devices should be seen in entirety
AP oblique modified cleaves method “frog lateral” overview: pelvis
Collimation- 17x14 CW
centering- same as AP
Long axis of femur should form 60-70 degree angle from table
Abduct both thighs 45 degrees, turning feet inward
AP oblique modified cleaves method “frog lateral”- evaluation criteria
Acetabulum, femoral head and femoral neck clearly demonstrated
RH: As much of the femoral neck should be seen as possible without overlap of the greater trochanter
Femoral axes extended from the hip bones at equal angles.
merrills note evaluation criteria for frog lateral pelvis
femoral neck WITHOUT superimposition by greater troch
excessive abduction causes greater to obstruct the neck
additional nontrauma pelvis frog notes
if patient has an orthopedic device, entire device must be seen on the AP and frog views
Exception to above: If patient has an intramedullary femoral rod, only the proximal aspect of the prosthesis needs to be included.
merrills centering for frog lateral pelvis
center at MSP & 1” superior to symph
pelvis frog lateral: over abduction/ over flexed
femoral necks are superimposed by greater
pelvis frog lateral: rotation
ilioischial column pops out & opposite obturator is more narrow
pelvis RPO & LPO judet method overview
Collimation- 17x14 CW
Patient 45 degrees
Center 1.5”-2” (V-space) medial to elevated ASIS
Top of light field should be 1-1.5” above crest of elevated ilium
Mark side down for each view, place horizontally in upper corner
pelvis RPO & LPO judet method evaluation criteria
Entire pelvis up to and including the lesser trochanters visualized on both sides
The broad surface of the iliac wing closest to the IR should be demonstrated without rotation
The acetabulum closest to the IR should be seen in profile
The hip joints, proximal femur and sacroiliac joint should be clearly demonstrated
pelvis RPO & LPO judet method: under rotation
iliopubic column not SCOOPED, ilioischial column can NOT see spine
pelvis RPO & LPO judet method: over rotated
on pelvis going OVER the other side of symph
merrills note for pelvis RPO & LPO judet method
ilioischial column & anterior acetabular rim visualized on side DOWN
iliopubic column & posterior acetabular rim visualized on ELEVATED HIP
additional trauma RPO & LPO pelvis judet method notes
If patient presents due to injury or some type of trauma, you always do trauma routine regardless of patient mobility.
If patient has an orthopedic device, entire device must be seen on the AP and oblique views
Exception to above: If patient has an intramedullary femoral rod, only the proximal aspect of the prosthesis needs to be included.
merrills note for centering for judet method oblique pelvis
perform a unilateral hip view
centering 2” inferior to elevated ASIS
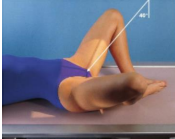
superioinferior inlet (BRIDGEMAN)-pelvis
40 degree CAUDAD ASIS
pelvis ring & inlet entirely
what special view is this?
superoinferior axial inlet (Bridgeman method)
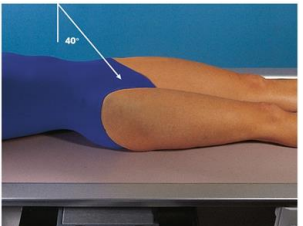
outlet taylor pelvis
cephalad angle to see rami without foreshortening
males= 20-35 degrees
females= 30-45 degrees
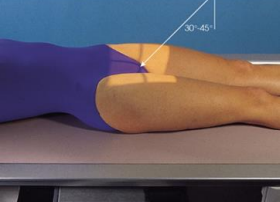
what pelvis special view is this?
AP axial OUTLET projection (Taylor method)
axiolateral cleaves: pelvis
cephalad to femoral shafts(25-45 degrees)
what pelvis special view is this?
axiolateral (original cleaves method)
pelvis special view: lateral (left or right) purpose
lateral lumbosacral junction, sacrum, coccyx, & superimposed hip bones & upper femora
what pelvis special view is this?
lateral pelvis
AP hip & oblique frog lateral technique
85 kVp, 10 mAs, center cell
AP hip overview:
Collimation- 10x12 LW
medially rotate legs 15-20 degrees inward
Centering
PERPENDICULAR TO FEMORAL HEAD
1.5” distal to midpoint of bisection of ASIS & symph
AP hip evaluation criteria:
SYMPH
Proximal one-third of the femur
Femoral head, penetrated and seen through the acetabulum
Any orthopedic appliance should be demonstrated in its entirety
merrills centering for AP hip/ frog lateral
femoral neck (2 ½” distal to bisection of ASIS & symph)
hip note: if patient has hardware…
entire device must be on both hip views
unless a femoral rod, only proximal aspect
AP oblique modified cleaves method (FROG LATERAL) overview:
Collimation- 10x12 LW
Long axis of femur 60-70 degrees from table
45 degree abduction of thigh (use sponge to support)
Centering (SAME AS AP)
The way techs do it: Have pt bend knee & center where hip joint is
1.5” distal (4 fingers) to bisection of ASIS & symph
AP oblique modified cleaves method (FROG LATERAL) evaluation criteria:
No rotation of the pelvis
Acetabulum, femoral head, and femoral neck clearly demonstrated
Lesser trochanter visible on the medial side of the femur
RH: As much of the femoral neck should be seen as possible without overlap of the greater trochanter
Excessive abduction causes the greater trochanter to obstruct the neck
Femoral axes extended from the hip bones at equal angles
AP oblique: modified cleaves method: merrills note for criteria
femoral neck WITHOUT superimposition by greater troch
rotation for hip frog: too much abduction/ flexion
greater superimposes neck & head
rotation for hip frog: too little abduction/ flexion
greater still in profile
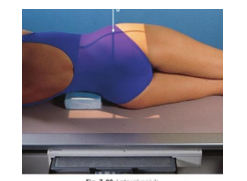
axiolateral danelius miller method (cross table lateral hip): technique
90 kVp, 32 mAs, center cell
axiolateral danelius miller method (cross table lateral hip):
40” SID- gridded free detector
56-60” fwall bucky
12×10 CW
axiolateral danelius miller method (cross table lateral hip): collimation:
12×10 CW
axiolateral danelius miller method (cross table lateral hip): centering : wall bucky
rotated foot end of bed 45 degrees AWAY from IR, center to groin (buttcheek)
axiolateral danelius miller method (cross table lateral hip): centering: free detector
Angle inferior border of detector away from the body 45 degrees so it is parallel with the femoral neck. Angle central ray 45⁰ into the groin to maintain alignment with the free detector. Adjust the detector and beam so they maintain 40” SID and alignment.
joint center note for ischial tuberosity
does NOT need to be included at joint center
hip- special view: modified axiolateral (Clements-nakayama method) purpose
lateral view for fractures or dislocation
hip- special view: modified axiolateral (Clements-nakayama method) angle
15 degree posterior angle
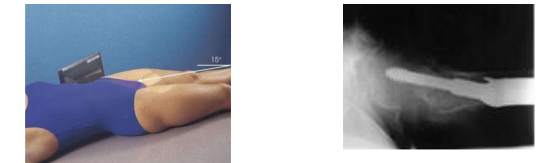
what hip special view is this?
modified axiolateral (Clements-nakayama method)
If a patient presents to the ED with a possible hip fracture with hip/ pelvis and chest x-ray orders…
hip/pelvis images should be obtained prior to a chest x-ray!