Misa test 4
1/98
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
99 Terms
What is cardiomyopathy?
A group of diseases affecting the heart muscle, with varied causes, symptoms, and treatments.
How can cardiomyopathy develop?
It can be acquired (from another disease or condition) or inherited; sometimes the cause is unknown.
What are the three main types of cardiomyopathy?
Dilated cardiomyopathy
Hypertrophic cardiomyopathy
Restrictive cardiomyopathy
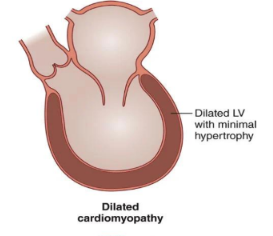
What is Dilated Cardiomyopathy?
Ventricular chamber enlargement with impaired systolic contractile function.
What is Dilated Cardiomyopathy?
Ventricular chamber enlargement with impaired systolic contractile function.
What are common causes (etiologies) of Dilated Cardiomyopathy?
diopathic or familial (genetic)
Inflammatory (secondary)
Viral myocarditis (infectious)
Connective tissue diseases (noninfectious)
Toxic (chronic alcohol use, chemotherapeutic agents)
Metabolic (e.g., hypothyroidism)
What is the typical pathology of Dilated Cardiomyopathy?
Marked enlargement of all four cardiac chambers; sometimes limited to the left or right side.
What is the hallmark feature of Dilated Cardiomyopathy?
Ventricular dilatation with decreased contractile function; usually both ventricles are impaired, sometimes only the left or right.
How does Dilated Cardiomyopathy affect cardiac performance?
Stroke volume and cardiac output decline due to impaired myocyte contractility.
What are the consequences of valvular regurgitation in Dilated Cardiomyopathy?
Excessive volume and pressure cause atrial dilation.
Blood regurgitates into the left atrium, reducing forward stroke volume.
Regurgitation returns to the LV during diastole, increasing volume load on the dilated LV.
What is the primary effect of the cause of Dilated Cardiomyopathy?
It results in reduced contractility, which leads to reduced stroke volume.
What are the consequences of reduced stroke volume in DCM?
Decreased cardiac output → fatigue, weakness
Left ventricular (LV) dilatation → mitral regurgitation
What happens when ventricular filling pressures increase in DCM?
Pulmonary congestion → dyspnea, orthopnea
Systemic congestion → hepatomegaly, edema
What are common clinical findings in Dilated Cardiomyopathy?
Congestive heart failure
Fatigue
Lightheadedness
Exertional dyspnea
What diagnostic studies are used for Dilated Cardiomyopathy?
EKG: Detects arrhythmias (commonly atrial fibrillation and ventricular tachycardia)
Echocardiography: Shows dilated chambers and mitral/tricuspid valve regurgitation
Cardiac catheterization: Determines if coronary artery disease contributes to impaired ventricular function
What are the main goals of treatment for Dilated Cardiomyopathy?
Relieve symptoms
Prevent complications
Improve long-term survival
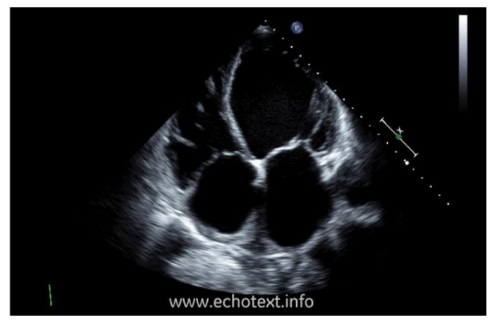
What is this?
Apical 4 chamber view of DCM

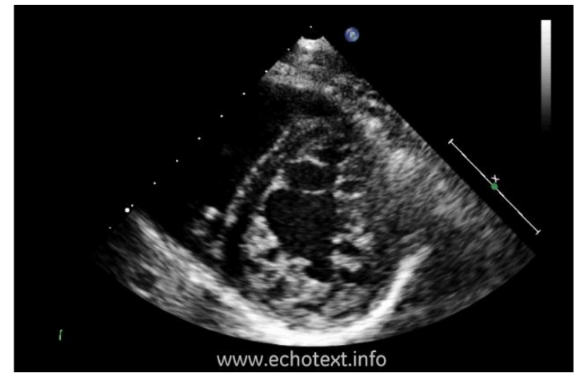
What is this?
PSSA MV view of DCM with LV thrombus
What medications are used for the medical treatment of heart failure in DCM?
Diuretics
ACE inhibitors
How are arrhythmias prevented and treated in DCM?
Maintain serum electrolytes, especially potassium and magnesium
Implantable cardioverter-defibrillator (ICD) reduces arrhythmic deaths
What other treatments help prevent complications in DCM?
Prevention of thromboembolic events
Cardiac transplantation for advanced cases
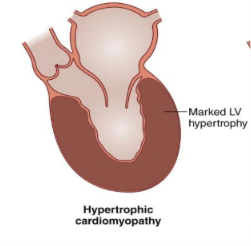
What is Hypertrophic Cardiomyopathy (HCM)?
A condition where the ventricular wall becomes abnormally thick with impaired diastolic relaxation but usually normal systolic function.
Which part of the heart is typically affected in HCM?
Usually the left ventricle, though one or both ventricles can be involved.
What causes Hypertrophic Cardiomyopathy?
Genetic mutations in proteins that control heart muscle contraction, leading to thickening and scarring over time; it is usually familial and autosomal dominant.
What is the most common pattern of hypertrophy in HCM?
Asymmetric hypertrophy of the ventricular septum, causing impaired diastolic compliance and filling.
How is the histology of HCM different from hypertrophy caused by hypertension?
Myocardial fibers show extensive myocyte disarray, leading to ventricular arrhythmias and possible sudden death.
What happens when HCM causes left ventricular outflow obstruction?
Thickened septum narrows the outflow tract.
Blood flow during systole pulls the anterior mitral leaflet toward the aortic valve, obstructing flow.
Results in increased LV pressure and pulmonary congestion (dyspnea, fluid in lungs).
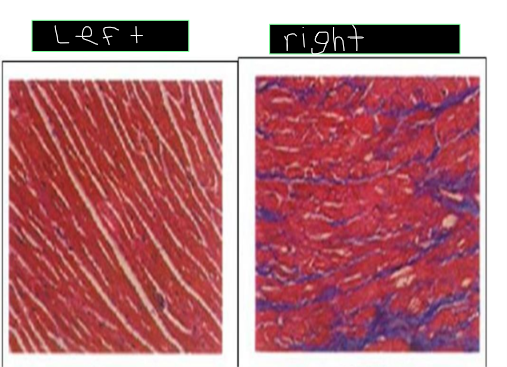
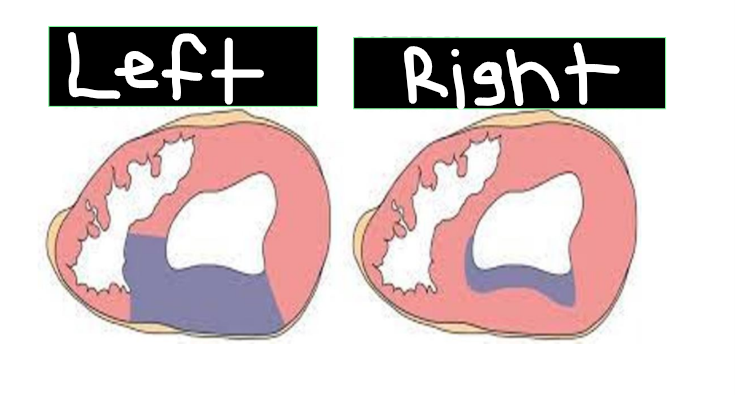
What is on the left and the right?
The left is normal and the right is HCM
What is the typical age of presentation for Hypertrophic Cardiomyopathy?
The average age of presentation is mid‑20s.
What are common symptoms of HCM?
Range from none to severe physical limitations
Dyspnea (most frequent)
Angina due to high oxygen demand and narrowed coronary arteries
Syncope from arrhythmias caused by abnormal myofibers
What is the most serious potential manifestation of HCM?
Ventricular fibrillation leading to sudden cardiac death.
What are the main treatments for HCM?
Beta blockers (reduce myocardial demand by slowing heart rate)
Drugs for atrial fibrillation
Septal myectomy if symptoms persist despite medication
Heart transplant in severe cases
What is the prognosis for HCM?
Sudden death rate in adults is less than1% per year
About 5% develop adverse LV remodeling and progressive systolic decline
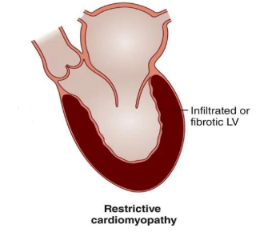
What is Restrictive Cardiomyopathy (RCM)?
A rare condition where ventricles become rigid (not thickened), impairing diastolic filling but with normal or near‑normal systolic function.
What is the most common recognized cause of RCM?
Amyloidosis, where abnormal amyloid fibrils accumulate in tissues and disrupt normal function.
What are other causes of RCM?
Infiltration of abnormal substances (amyloid fibrils)
Storage diseases (iron overload)
Myocardial fibrosis (after radiation)
What are etiologic conditions associated with RCM?
Infiltrative diseases: amyloidosis, sarcoidosis
Scleroderma
Storage diseases: hemochromatosis
Endomyocardial fibrosis, metastatic tumors, radiation
What is the pathophysiology of RCM?
Reduced ventricular compliance → increased diastolic filling pressures → atrial pressure rise → venous congestion
Decreased ventricular filling → reduced cardiac output
What are symptoms and prognosis of RCM?
Symptoms: edema, hepatomegaly, jugular vein distention, weakness, fatigue
Prognosis: generally poor, except when treatment targets the underlying cause
What is Left Ventricular Noncompaction
A rare congenital abnormality where the myocardium is thickened with prominent trabeculae and deep recesses extending from the LV cavity into intertrabecular spaces..
How does Left Ventricular Noncompaction affect heart function?
The abnormal myocardial regions contract poorly and have impaired diastolic relaxation, which weakens overall heart performance.
What is the recommended approach to caring for someone with Left Ventricular Noncompaction?
Treatment focuses on managing symptoms and complications, as there is no corrective therapy.
What is Arrhythmogenic Cardiomyopathy (ARVC)?
A genetic form of cardiomyopathy where the right ventricular (and sometimes left ventricular) myocardium is replaced by adipose and fibrous tissue, causing rhythm disturbances and contractile dysfunction.
What is the main cause of ARVC?
Genetic mutations affecting heart muscle structure and function.
What are common symptoms of ARVC?
Ventricular arrhythmias
Syncope
Palpitations
Sudden death
What is Ischemic Heart Disease (IHD)?
A condition caused by an imbalance between myocardial oxygen supply and demand, most often due to atherosclerosis of the coronary arteries.
What happens during ischemia?
The heart muscle’s demand for oxygenated blood exceeds the supply, usually because of partial or complete blockage (stenosis) from atherosclerotic plaque in the coronary arteries.
Why is Ischemic Heart Disease significant?
It affects millions of Americans and is the leading cause of death in industrialized nations.
How does the normal heart maintain oxygen balance?
The heart always gets the oxygen it needs because coronary arteries increase oxygen delivery whenever demand rises, like during exercise.
When does most coronary perfusion occur?
Unlike other arteries that fill during systole, coronary perfusion get most of their blood flow during diastole.
Why is coronary flow unimpaired during diastole?
Because the relaxed myocardium does not compress the coronary vasculature, allowing blood to flow freely.
How does heart rate affect myocardial oxygen demand?
When heart rate increases (e.g., during exercise), oxygen consumption rises, leading to higher oxygen demand.
How does contractility influence myocardial oxygen demand?
Increased contractility (inotropic state), such as from certain drugs, raises oxygen consumption and demand.
What happens when coronary vessel stenosis is less than 60%?
It means the artery is not narrowed enough to cause ischemia, so blood flow is still good even during exercise.
What occurs when coronary vessel stenosis is greater than 70%?
Resting blood flow is normal, but maximum flow is reduced. During increased oxygen demand, coronary flow becomes inadequate, leading to myocardial ischemia.
What is the effect of greater than 90% stenosis?
Even with maximal vessel dilation, blood flow cannot meet basal requirements, causing ischemia even at rest.
What circulatory conditions can decrease myocardial perfusion and cause ischemia?
Hypotension (low perfusion pressure)
Hypovolemia (low blood volume from blood loss or dehydration)
Septic shock (infection‑induced low blood pressure)
How can blood oxygen content contribute to myocardial ischemia?
Severely decreased blood oxygen content
Marked anemia (low red blood cell or hemoglobin levels)
Impaired oxygenation by the lungs
What non‑coronary factors can trigger ischemia even without Coronary Artery Disease?
Rapid tachycardias
Acute hypertension
Severe aortic stenosis
What is the common result of these conditions?
Reduced oxygen delivery to the myocardium, leading to ischemic injury and potential heart failure.
What determines the consequences of myocardial ischemia?
The severity and duration of the imbalance between oxygen supply and demand
What were the previously understood outcomes of an ischemic episode?
Either irreversible myocardial necrosis (MI) or rapid and full recovery of myocyte function.
What is now known about possible outcomes of ischemia?
Ischemia can cause prolonged contractile dysfunction, with eventual recovery of normal function.
What is a stunned myocardium?
Myocardial tissue that shows prolonged systolic dysfunction after a brief, severe ischemic episode, even after normal blood flow returns.
What is a hibernating myocardium?
Chronic ventricular contractile dysfunction caused by persistently reduced blood supply (often from multivessel CAD); function can improve after revascularization.
What is a myocardial infarction (MI)?
A region of myocardial necrosis resulting from prolonged cessation of blood supply.
What is Angina Pectoris?
The most common manifestation of ischemic heart disease; means “strangling in the chest.” Pain may radiate to the chest, left shoulder, arms, or jaw.
What is Stable Angina?
Chest pain triggered by physical exertion or emotional stress, relieved by rest or medication.
What are key features of Stable Angina?
Predictable pattern
Pressure or tightness in chest
Relieved by rest
Lasts 1–5 minutes
What is Unstable Angina?
Chest pain that occurs suddenly at rest, more severe or frequent than before; not relieved by rest or medication and may indicate acute myocardial infarction.
What is Variant (Prinzmetal) Angina?
Chest pain at rest caused by coronary artery spasm, not increased myocardial demand.
What is Silent Ischemia?
Asymptomatic episodes of myocardial ischemia detected on Echo or Stress Echo testing.
What ECG changes occur during myocardial ischemia?
ST‑segment and T‑wave changes can appear, indicating altered electrical activity due to reduced oxygen supply.
What does STEMI indicate?
ST‑segment elevation myocardial infarction — complete coronary artery blockage causing transmural ischemia and extensive heart muscle damage.
What does NSTEMI indicate?
Non‑ST‑segment elevation myocardial infarction — partial blockage or temporary clot causing ST‑segment depression or T‑wave inversion (subendocardial ischemia).
What does ST‑segment depression on ECG signify?
Ischemia without infarction, often seen with left bundle branch block (LBBB) or ventricular hypertrophy.
What is on the left and on the right?
Left: ST‑Elevation Myocardial Infarction.
Right: Non‑ST‑Elevation Myocardial Infarction.
What is the purpose of a stress test in suspected CAD?
To evaluate heart function and detect ischemia by increasing workload through exercise or medication.
How is a standard exercise stress test performed?
The patient exercises on a treadmill or stationary bike at progressively higher workloads while being monitored for chest pain, dyspnea, or ECG changes.
When is a stress test stopped?
When angina develops
When ECG signs of ischemia appear
When target heart rate (85% of MHR = 220 − age) is reached
Or when the patient becomes too fatigued to continue
What is Coronary Angiography?
A procedure where a thin catheter is inserted into a blood vessel (usually in the groin or arm) and guided to the heart. A contrast dye is injected to make coronary arteries visible on X‑ray (fluoroscopy).
What is the purpose of Coronary Angiography?
It is the most direct method to identify coronary artery stenosis, allowing visualization of atherosclerotic lesions after injection of radiopaque contrast material.
What lifestyle changes help manage ischemic heart disease?
Quit smoking, eat a healthy diet, exercise, manage weight, and limit alcohol intake.
Why is quitting smoking important in ischemic heart disease?
Smoking damages blood vessels and increases the risk of coronary artery disease.
How does regular exercise help ischemic heart disease?
Improves circulation, strengthens the heart, and reduces oxygen demand during activity.
What is the role of Beta Blockers in treatment?
They reduce heart rate and contractility, lowering oxygen demand and preventing angina.
What are Beta‑1 receptors responsible for?
they are responsible for increasing heart rate and increasing the strength of cardiac contraction when stimulated also they are found in cardiac muscle.
What are Beta‑2 receptors responsible for?
They are responsible for bronchodilation, because they’re found in bronchial smooth muscle and cause dilation when stimulated.
How do Calcium Channel Blockers work?
They block calcium entry into vascular smooth muscle, causing vasodilation and reduced workload.
What is the function of Nitrates?
Cause vasodilation of blood vessels, improving oxygen delivery and relieving chest pain.
What are common Antiplatelet medications used in ischemic heart disease?
Clopidogrel (Plavix) and Aspirin, which prevent platelet aggregation and reduce clot formation.
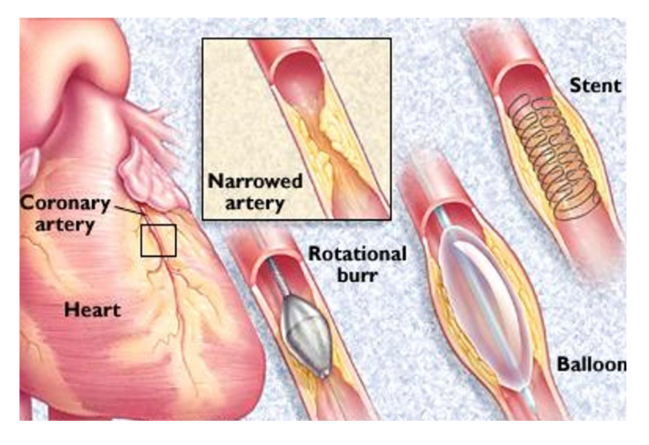
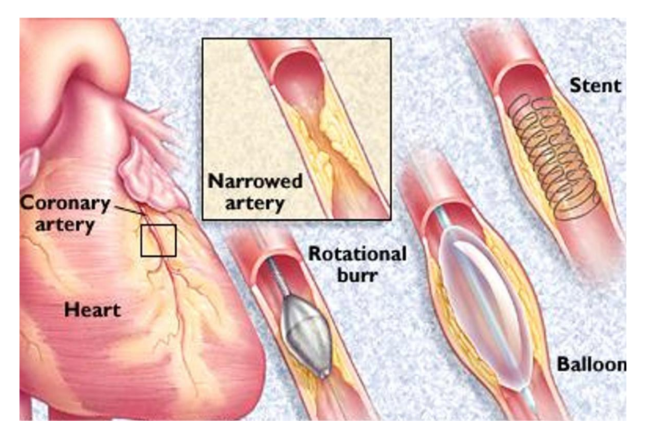
What is PCI (Percutaneous Coronary Intervention)?
A procedure where a thin catheter with a balloon is inserted into a narrowed artery; the balloon is inflated to widen the artery, and a stent is placed to keep it open.
What is CABG (Coronary Artery Bypass Graft)?
A surgery that uses a healthy blood vessel (from the leg, chest, or arm) to bypass a blocked coronary artery and restore blood flow to the heart.
What is the mortality rate associated with myocardial infarction?
About 250,000 deaths per year, with 30% mortality within the first 2 hours.
What happens after 45 minutes of ischemia?
Cardiac muscle death occurs.
How is myocardial infarction diagnosed?
Electrocardiographic changes (ST elevation)
Myocardial enzyme elevation: Creatine kinase, Troponin, C‑reactive protein
What is Cardiomyopathy in MI complications?
It is a disease of the heart muscle that weakens its ability to pump effectively after an MI.
What are major structural complications of MI?
Aneurysm (can cause hypotension, dyspnea, cardiogenic shock)
Thrombus formation
Scar tissue
Valve dysfunction
What are severe rupture-related complications of MI?
Cardiac rupture (free wall or septal)
Pericardial effusion
Septal rupture, leading to acute ventricular septal defect (VSD)