Sodium and Water Discussion
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
what is antidiuretic hormone?
aka vasopressin: a hormone synthesized in the hypothalamus (HTH) and released from the posterior pituitary in response to increased blood (ECF) osmolality (detected at the HTH) and decreased blood volume (detected as hypotension at aortic arch baroreceptors and signaled via neurons to the HTH, and detected as decreased renal perfusion leading to increased renin and increased angiotensin II)
what is the action of ADH
1) restricts urinary H2O loss by increasing the number of aquaporin channels in the medullary collecting duct for reabsorption of H2O from the urinary filtrate back into the bloodstream
2) causes arteriole vasoconstriction to increase BP
serum sodium concentration ([Na+]s) is a reflection of what? and determines what states?
reflection of total body H2O (TBW) and determines hyponatremia, eunatremia, and hypernatremia
why does a change in the serum Na+ concentration reflect the amount of water in the body
because water moves freely across all the body compartments (intracellular, extracellular, and blood) and Na+ is regulated across the body compartments
serum sodium concentration reflects total body water, and fluid status reflects Na+ISF (interstitial fluid). too little water means?
hypernatremia
serum sodium concentration reflects total body water, and fluid status reflects Na+ISF (interstitial fluid). too much salt means?
edema
serum sodium concentration reflects total body water, and fluid status reflects Na+ISF (interstitial fluid). too little salt means?
volume depletion
serum sodium concentration reflects total body water, and fluid status reflects Na+ISF (interstitial fluid). too much water means?
hyponatremia
what is hypernatremia
high sodium due to too little water
what is edema
water follows Na+, so if you have too much salt, this manifests as too much fluid in the extracellular space
what is volume depletion
if your "bag of salt water" is too small, this will manifest as "volume depletion" - hypotension, poor skin turgor
what is hyponatremia
low sodium due to too much water
how can you correct these water and sodium imbalances: hypernatremia
drink/administer water, decrease diuresis, turn on ADH
how can you correct these water and sodium imbalances: edema
decrease salt intake, administer a diuretic to lose sodium
how can you correct these water and sodium imbalances: volume depletion
increase salt intake, administer 0.9% saline
how can you correct these water and sodium imbalances: hyponatremia
stop drinking/administering water, increase diuresis to lose water, turn off ADH
water imbalance and salt imbalance are NOT mutually exclusive, they can occur ?
simultaneously
use this case for the following questions:
18 y/o admitted to hospital following 4 days of abdominal cramps and severe diarrhea (8-10 watery stools/day). she has been drinking water but has no appetite for anything else. no edema, but skin turgor is poor, oral mucosal tissues appear dry, and BP is 85/50 lying down and 70/40 standing. her weight is down 4 kg from normal. serum Na+ is 135 (normal is 140).
is the pt's problem ECV (low Na+), water balance, or both?
water balance problem secondary to severe diarrhea!
explain why the pt has a water balance problem secondary to severe diarrhea
pt clearly is Na+ (ECV) depleted (orthostatic BP: drop in BP from lying down to standing), from having lost both Na+ and H2O from diarrhea. she has replaced some of her losses by continued water intake (in excess relation to Na+), and in the setting of decreased free water excretion, she has developed hyponatremia - relative water excess compared to sodium
what about ADH levels in this patient?
recall that ADH is simulated by both hyperosmolality (high levels of solutes) and volume depletion; note that the pt's ADH is increased
in this case, does the hypoosmolality "win" and turn OFF the ADH release, or does the volume depletion "win" and stimulate ADH release?
volume depletion overrides osmolality as a stimulus for ADH release. there is increased ADH due to ECV (extracellular volume) depletion (decreased BP is signaled in the aortic arch baroreceptors). thus, even if a pt is hyponatremic (hypo-osmolar), ADH will still be secreted if the pt is markedly volume depleted. the presence of ADH will prevent the kidney from excreting a dilute urine. thus, as she drinks more and more water it will be retained and will dilute the serum sodium concentration further, making her even more hypo-osmolar
what is the appropriate treatment for this patient?
pt needs to have her ECV replenished, which will treat both the salt and water problems. by giving her normal saline:
- her salt deficit will be corrected
- added volume will turn off the stimulation of ADH, thereby allowing her to pass a dilute urine and return her intracellular volume to normal
use this case for the following questions:
you recently hired a 68 y/o to clean your dental office on friday evenings. upon returning to your office on monday morning, you find him lying in the hallway between operatories - conscious, but unable to move the R side of his body, including the muscles of facial expression, indicating that he has had a stroke. based on his normal schedule, you quickly deduce that he has been down on the floor for 48 hours and is unable to take anything by mouth
PE: T 38.6 C, HR 86, BP 140/90, RR 18. right hemiplegia, skin rubrous, hot and dry, good turgor. tongue is dry, not shrunken. heart RRR, lungs clear.
hypernatremic!
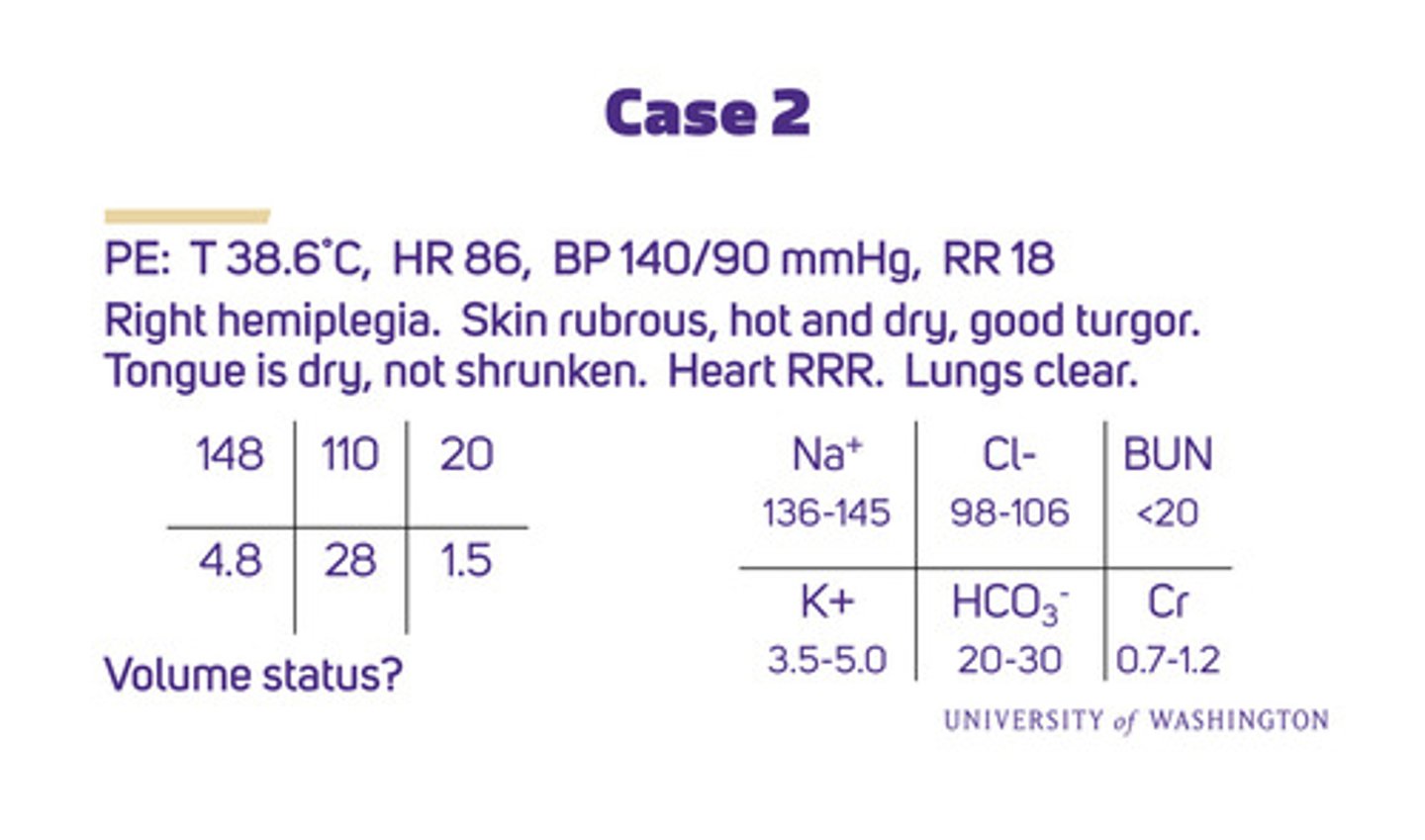
what is the pt's volume status
PE results indicate that pt is not volume depleted. however, from blood tests, his hypernatremia reveals that he does have a "free water deficit". in cases of hyponatremia or hypernatremia, establish the volume status first to discover the cause and plan a treatment
what is the status of this pt's urine electrolytes
he is hyperosmolar (serum Na+ 148) hence:
- ADH should be turned on, leading to a concentrated urine (eg a urine osmolality of at least 600 mOsm/kg - recall normal is 285 mOsm/kg)
- kidneys will attempt to conserve Na+ loss for water resorption and protect extracellular volume, leading to low urine Na+ (eg <10 mEq/L)