Lecture 23 (Bonus Lecture): Hip and Shoulder Review
1/82
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
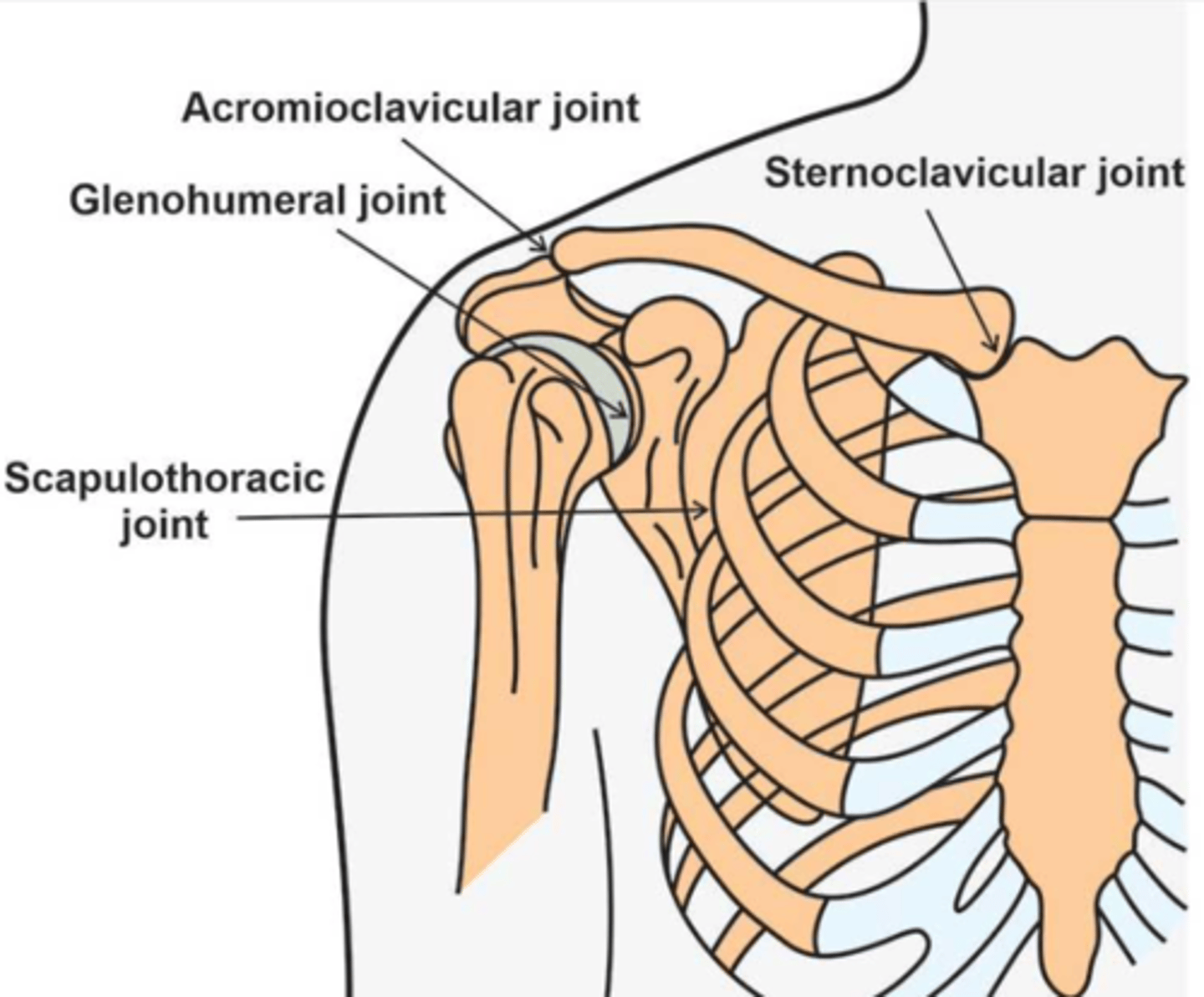
Shoulder articulations
- Sternoclavicular
- Acromioclavicular
- Scapulothoracic
- Glenohumeral
Sternoclavicular joint
- Saddle joint
- Convex clavicle sup/inf
- Concave clavicle ant/post
Acromioclavicular joint
- Convex distal clavicle
- Concave acromion
Scpulothoracic joint is a ___ joint
Planar
Glenohumeral joint
- Convex humerus
- Concave glenoid
Maitland mobilizations: grade 1
Small amplitude out of resistance
Maitland mobilizations: grade 2
Large amplitude out of resistance
Maitland mobilizations: grade 3
Large amplitude into resistance
Maitland mobilizations: grade 4
Small amplitude into resistance
Maitland mobilizations: grade 5
High velocity thrust
GHJ motions: flexion
- Roll = anterior
- Glide = posterior
GHJ motions: extension
- Roll = posterior
- Glide = anterior
GHJ motions: adduction
- Roll = inferior
- Glide = superior
GHJ motions: abduction
- Roll = superior
- Glide = inferior
GHJ motions: IR
- Roll = anterior
- Glide = posterior
GHJ motions: ER
- Roll = posterior
- Glide = anterior
- Only with frozen shoulder, do a posterior glide
A 19 year old female patient is being seen in a PT clinic for pain which has worsened during the swimming season. She complains of dullness and heaviness in the shoulder, and pain with prolonged activity. She tests 7/9 on a Beighton score test. What is the best intervention for her initial treatment session?
A. Modified planks and side planks
B. Light multidirectional perturbations of the arm held at 90 degrees flexion in supine
C. Inferior and posterior grade III mobilizations of the GHJ
D. Moist heat to the shoulder at the beginning of the session for pain modulation
B. Light multidirectional perturbations of the arm held at 90 degrees flexion in supine
Beighton Scale
- Palms to floor
- Hyperextend elbow
- Hyperextend knee
- Thumb to forearm
- Pinky finger bent to 90 deg
- Assess L and R
- 5/9 = hypermobile
RTC impingement: stage 1
- Intermittent pain
- Age 35
RTC impingement: stage 2
- Mild to mod pain
- Pain with activity
RTC impingement: stage 3
- Pain at rest or with activity
- May have night pain
- Weakness of RTC and/or scap muscles
RTC immobilization: small tear (
- Sling 1-2 weeks
- Removal for exercise the day of surgery or 1 day post op
RTC immobilization: medium to large (1-5 cm)
- Sling or abduction orthosis/pillow for 3-6 weeks
- Removal for exercise 1-2 days post op
RTC immobilization: massive (> 5 cm)
- Sling or abduction orthosis/pillow for 4-8 weeks
- Removal for exercise 1-3 days post op
Mobilization to increase flexion at: SCJ
Inferior glide
Mobilization to increase flexion at: ACJ
- Posterior glide + posterior rotation
- Clavicle getting out of the way so the arm can come up and forward
Mobilization to increase flexion at: STJ
Upward rotation + posterior tilt
Mobilization to increase flexion at: GHJ
Posterior glide
How long do you perform PROM for large RTC?
6-8 weeks
Which position do you start performing PROM of shoulder for RTC?
Supine
Following large RTC, AROM flexion and abduction must be done without
Shoulder hiking
Large RTC, perform gentle mobilizations in ___ pack position to prevent translation in which directions?
- Open
- Anterior and superior
Strengthening post RTC
- RTC strength must be addressed before large primary movers
- Initiate strengthening with isometrics
How long should you wait to perform closed chain exercises following RTC tear of any size?
6 weeks
How long should you wait to perform dynamic strengthening exercises following small RTC tear?
8 weeks
How long should you wait to perform dynamic strengthening exercises following large RTC tear?
12 weeks
Caution with resisted ER and passive IR if these 2 muscles are repaired
- Supraspinatus
- Infrapsinatus
Caution with resisted IR and passive ER if this muscle is repaired
Subscapularis
Supraspinatus and infraspinatus are IR's or ER's?
ER's
Subscapularis is an IR or ER?
IR
After completing an examination of a patient with shoulder pain, the PT concludes that the cause is subscapularis tendinitis. The clinical finding supportive of this conclusion is:
A. Tenderness at the greater tubercle of the humerus
B. Painful resisted shoulder adduction
C. Pain provoked with active glenohumeral external rotation
D. Pain provoked with passive glenohumeral external rotation
D. Pain provoked with passive glenohumeral external rotation
Subscap is an IR. Pain with contraction of that muscle and when stretching the affected muscle. Have an IR, so stretching it into ER would be painful.
Tendonitis results in pain with
- Contraction of the muscle
- Stretching of the muscle
Hip arthrokinematics
- Convex femoral head
- Concave acetabulum
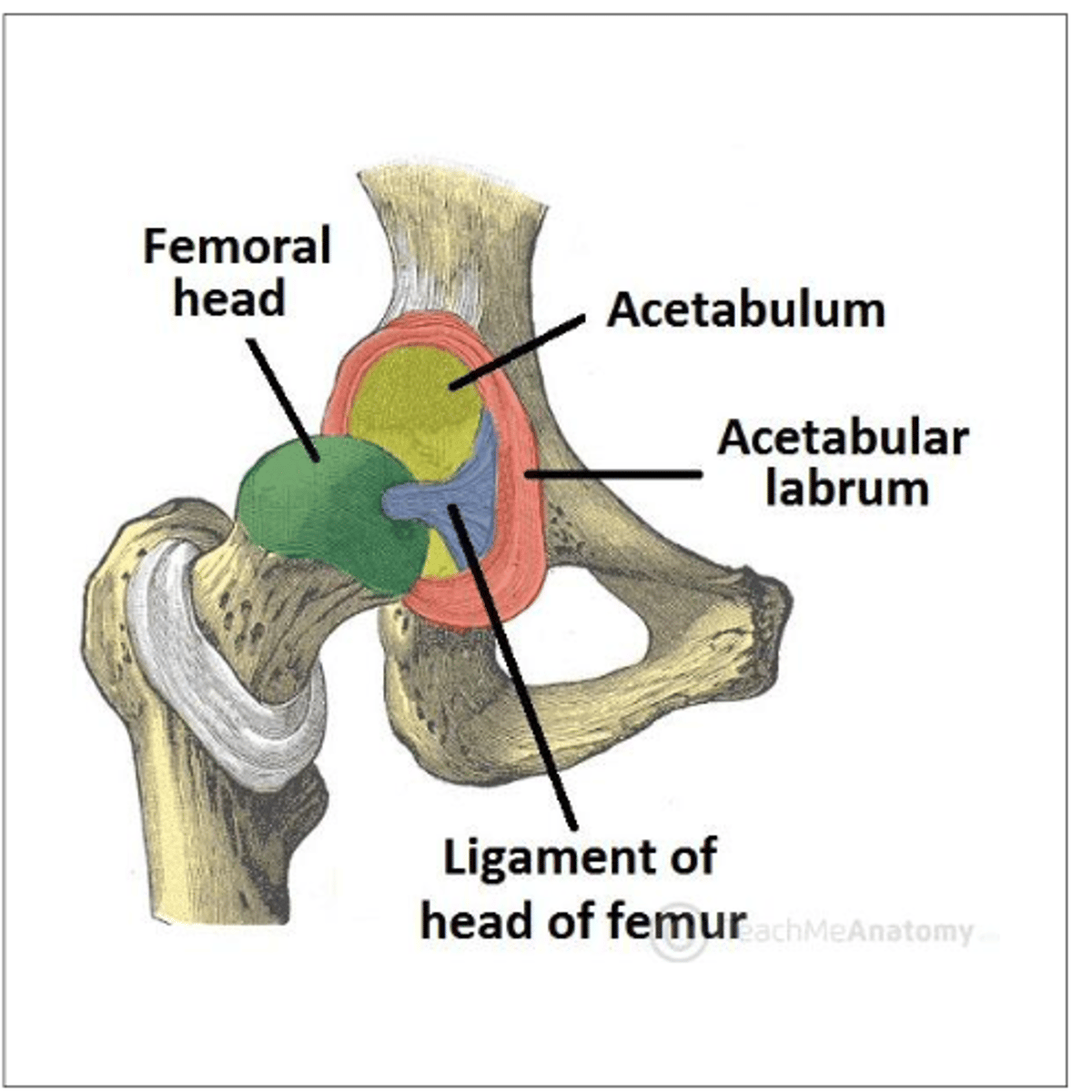
Hip joint is a ___ and ___ joint
Ball and socket
What deepens the insertion of the femur into the acetabulum and thus providing more stability?
Labrum
The labrum assists in negative pressure to prevent excess
Distraction
Age of onset: Legg-Calve-Perthes disease
4-8
Age of onset: Slipped capital femoral epiphysis
10-15
Pathology of Legg-Calve-Perthes disease
- Deformity/flattening of femoral head due to loss of blood supply
- Femoral head necroses, fragments, and reossifies
Pathology of Slipped capital femoral epiphysis
Displacement of femoral head due to slippage from the growth plate
Patient population: Legg-Calve-Perthes disease
- Short stature
- Males
Patient population: slipped capital femoral epiphysis
- Overweight
Symptoms of Legg-Calve-Perthes disease
- Pain worsens with activity
- Limping
- Stiffness
Symptoms of slipped capital femoral epiphysis
- Pain worsens with activity
- Stiffness
- Difficulty WB'ing
- Typically in externally rotated position
Treatment of Legg-Calve-Perthes disease
Conservative
Treatment of slipped capital femoral epiphysis
Surgical treatment to stabilize
SCFE
- "Ice cream falling off cone"
- Most often happens during peak growth velocity

Legg-Calve-Perthes Disease
Avascular necrosis of the femoral head

What is Thomas test used for?
- Test for hip flexor length
- Patient sits on edge of bed, assist patient to supine and passively flex single knee to chest
- Pt then holds knee into chest and therapist assesses position
Thomas test, flexed hip
- Iliopsoas tight
- One joint hip flexor
Thomas test, extended knee
- Rectus femoris tight
- 2 joint muscle
Thomas test, abduction
- Tight TFL or ITB
Thomas test, tibial ER
- Biceps femoris tight
- Attaches laterally, which pulls it into ER at femoral head
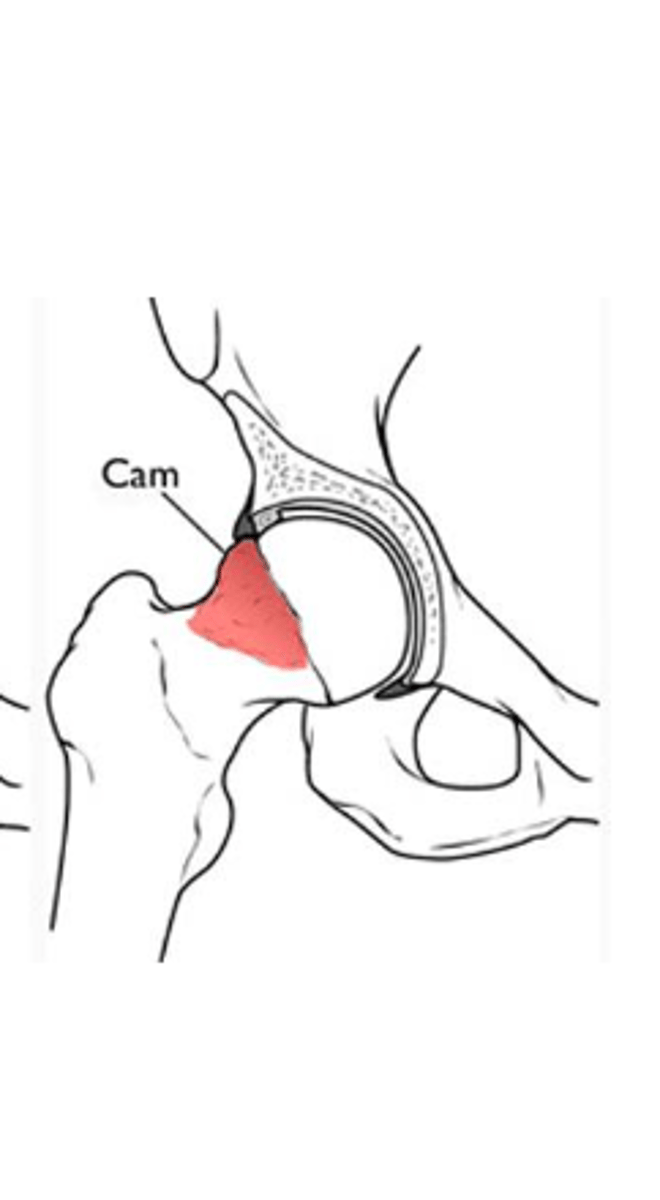
Hip impingement
- Can be asymptomatic, symptoms arise when cartilage or labrum damage occurs
- Pain worsens over time
- Groin pain
- Pain with activity, repetitive flexion, and at end range flexion and IR
- (+) FADIR
Cam impingement is more common in
Males
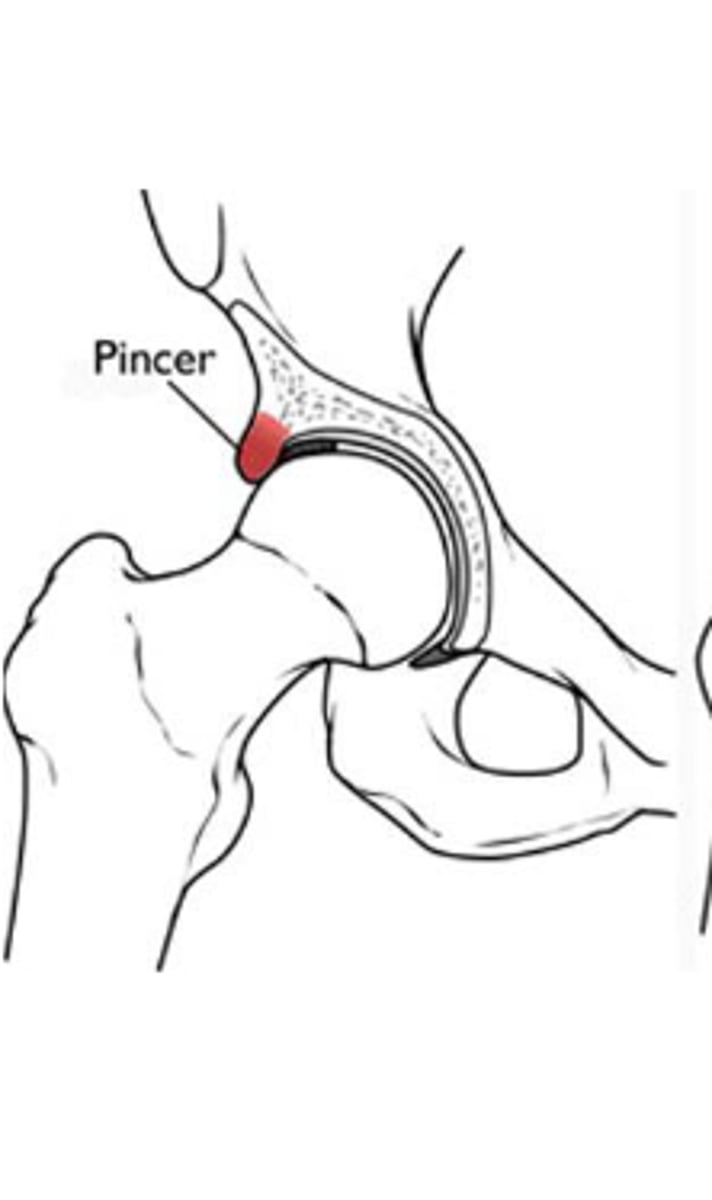
Pincher impingement is more common in
Females
Trochanteric bursitis
- Inflammation of deep trochanteric bursa due to direct blow, irritation by ITB, or biomechanics/gait abnormalities causing repetitive micro trauma
- Tenderness over lateral aspect of greater trochanter
Symptoms of trochanteric bursitis
- Hip may rest in abduction or favor abduction with movement
- Asymmetrical standing
- Pain with stairs
- Tightness in ITB
- (+) Ober's
- Popping or crepitation felt at GT with flexion/extension of hip (biking, running)
Treatment of trochanteric bursitis
- RICE
- Activity modification, decrease repetitious activity
- ITB stretching
- Steroid injection
Tendonitis: rectus femoris
- Pain usually located at origin of ASIS, or just distal
- Patient often complains of groin pain during sprinting or extending the knee
Tendonitis: iliopsoas
- Groin pain, which can radiate into anterior thigh
- Resisted hip flexion and ER are often painful
Tendonitis: glut med
- Tenderness just proximal to greater trochanter
- Pain reproduced by resisted abduction of hip
- D/D for trochanteric bursitis
Tendonitis: piriformis
- Tenderness to deep palpation near hook of greater trochanter or in muscle belly
- Pain reproduced by piriformis stretch
- Sciatic symptoms are possible
A 19 year old patient is being seen in PT after sustaining an injury doing hurdles a week and a half ago. She reports she felt a pop and instant pain and loss of function in the R hip. She reports pain with walking, tenderness when sitting, and she lacks terminal knee extension during gait. Which of the following treatment plans is most appropriate for this session?
A. Ice and estim, education on AC use, RICE, and gentle core activation
B. Submax isometrics, cross friction massage, gentle hip stretching
C. Single leg standing and balance activities to regain WBing tolerance, submax isometrics, cross friction massage
D. RICE, pelvic tilts, gentle hip stretching
A. Ice and estim, education on AC use, RICE, and gentle core activation
Hamstring strain MOI
- Distinctive
- Immediate pain during sprinting or while decelerating
- May report tearing sensation
Hamstring strain symptoms
- Tenderness elicited with passive stretching of hamstrings
- Posterior thigh pain, often near the buttock
- Pain worsened with resisted knee flexion
- Tenderness to palpation at ischial tuberosity or along length of HS belly or distal insertions
- Can be due to dominance of HS over glut max, decrease muscle endurance, flexibility limitations
If patient experienced hamstring strain as a result of dominance of HS over glut max, what is a key part of rehab?
Strengthening gluts
Hamstring strain rehab: phase I
- RICE
- No stretch or strain on muscle
- Lumbopelvic control and alignment
Hamstring strain rehab: phase II
- Submit isometrics
- Massage/cross friction massage
- Trunk stabilization
- GENTLE stretching
- Progress stability and control exercises
- CKC and WB'ing
- Muscle endurance
- Avoid fatigue and compensation patterns
Hamstring strain rehab: phase III
- Balance
- Eccentrics
- Controlled speed
- Dynamics
- Plyometrics
Hamstring strain rehab: prevention
- Mobility
- Warm up/cool down
- Glut strength
- Posture/pelvic tilt
Hip OA prediction
- Self-reported squatting as an aggravating factor
- Active hip flexion causing lateral hip pain
- Scour Test with adduction causing lateral hip or groin pain
- Active hip extension causing pain
- Passive internal rotation of less than or equal to 25°
- More factors present, greater chances of having OA
- Variables are positive when there is pain or limited ROM in the tests
Which of the following does not increase the likelihood of a patient being diagnosed with hip OA?
A. Pain with squatting
B. Passive IR of 20 degrees
C. Passive ER of 30 degrees
D. Pain with stair ambulation
C. Passive ER of 30 degrees