UE Physical Therapy Evaluation
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
what does the patient history do?
it should tell us 80-90% of what is wrong with the patient to help determine what examination is needed
what are the steps of clinical reasoning?
patient history
initial clinical hypothesis
screening examination
focused examination
what does the history/subjective examination tell us?
Severity: rate pain 0-10 (describing ten as the worst imaginable pain); how the pain affects their daily life/how limiting it is
Irritability: how quickly it comes on and how long it takes to ease
Nature of symptoms: annoyance, impairment, or disability; what you think may be going on; what tissue is the issue
Stability of disorder: getting worst, better, or staying the same
Stage of disorder: acute (goal is pain management), subacute, chronic (goal is general exercise)
Pain mechanism: nociceptive (MSK issue), neurogenic (nerve issue), nociplastic (pain that doesnt fit a clearcut pattern)
what is ECHOWS?
a framework used to assess the effectiveness of physical therapy student patient interviews
what are the components of ECHOWS?
E: establish rapport/therapeutic alliance
C: chief complaint
H: health history
O: obtain psychosocial persepective— how it is affecting their daily life
W: wrap up the interview asking “what other questions do you have for me or is there something I didnt ask that you would want me to know”
S: interviewing skills
what skills are evaluated during the S part of ECHOWS?
attending to patient comfort
avoiding jargon
maintaining interview flow
checking for patient understanding
documenting without disrupting interaction
what is our goal when doing the upper quarter screen and considering differential diagnosis?
not to diagnose the condition but to decide whether it is safe and appropriate to continue with a physical therapy examination
what are the possible mechanisms of viscerogenic pain?
convergence of visceral and somatic afferents in the spinal cord
visceral-somatic cross sensitization
shared neural pathways and spinal segment overlap
discuss hoffmans test
purpose: to screen for a possible upper motor neuron involvement related to cervical spinal cord pathology
procedure: flick the distal phalanx of the middle finger while holding it into extension
positive test: reflexive thumb flexion and or index finger flexion
how can we interpret a positive hoffmans sign?
it may suggest cervical spinal cord compression, cervical myelopathy, or upper motor neuron involvement
however, it should not be used as a stand alone diagnostic test, rather being interpreted within the full neuro screen
consider additional findings such as hyperreflexia, clonus, gait distrubance, balance changes, or bilateral symptoms
when should a positive hoffmans raise concerns?
progressive neuro symptoms
bilateral hand symptoms
loss of dexterity
gait changes
bowel/bladder changes
consider medical referral for possible cervical myelopathy
what is the question we shoudl ask ourselves every visit?
does this person belong in my clinic?
when a patient presents with upper quarter symptoms, our first responsibility is _______ not just examination. therefore, what should be our steps to dtermine what to do?
clinical decision making
listen to the patient
screen for red flags
screen for the neurological system
decide the next steps: treat if MSK, expand screening if unsure, refer out if red flags
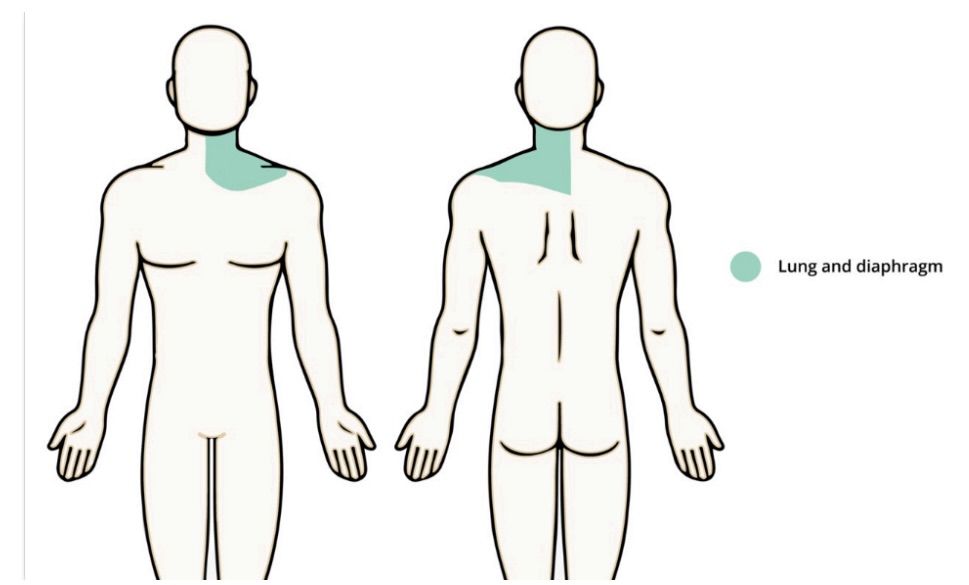
what is the referral pattern and possible signs and symptoms of the respiratory system?
cough, sputum, blood and sputum
chest pain
pain with deep breathing
body sweats, itching
cyanosis or clubbing of fingernails
history of smoking, pulmonary disorder
sinus/facial pain
loss of smell, nasal discharge, nose bleeds
difficulty breathing, wheezing, shortness of breath, snoring
foul odor
what is the referral pattern and possible signs and symptoms of the ears, nose, throat, and mouth?
ears
change in hearing
ringing in ears
ear pain/discharge
vertigo
masses/lumps
nose
sinus/facial pain
nosebleed or nasal discharge
itching
post-nasal drip
difficulty breathing
loss of smell or foul odor
throat/mouth
change in voice/hoaseness
sore throat or pain when swallowing
jaw pain
sores/ulcers
difficulty swallowing
masses/lumps
tooth pain
gum bleeding
what is the referral pattern and possible signs and symptoms of the MSK system?
referal pattern will be localized pain to the area of interest
signs and symptoms
· Reproducible pain or symptoms
· Tenderness to palpation
· Swelling or tightness
· Positive special tests
· Visible deformities or gait abnormalities
· History of MOI
· Pain described as aching, soreness, tightness, dull (no concerning descriptors like boring or deep pain)
· Limitations in ROM and MMT
· Pain that is relieved with rest and worse with activity
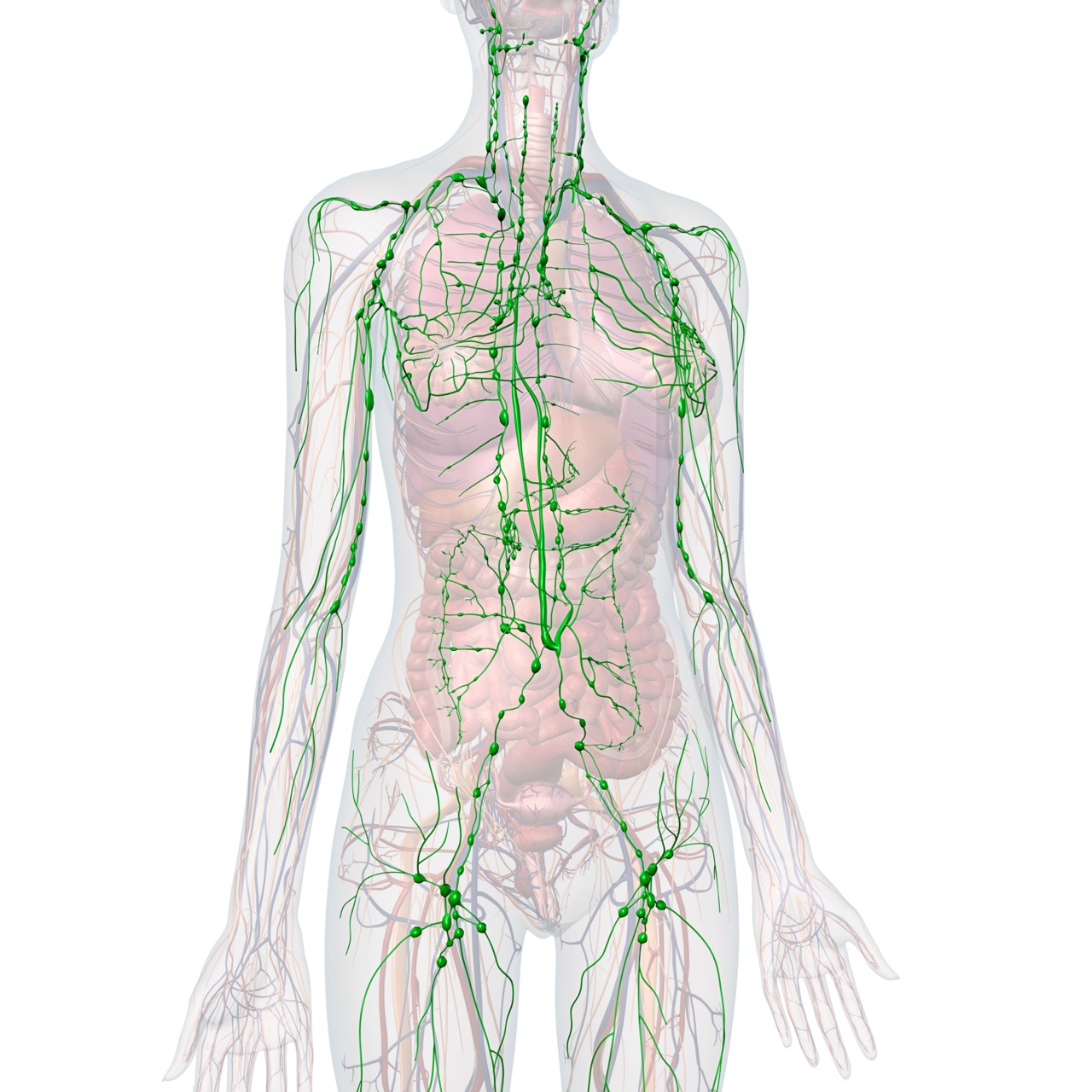
what is the referral pattern and possible signs and symptoms of the lymphatic system?
abnormal bruising
weight changes or fatigue
growths, lumps, bumps
limb edema
abdominal or left shoulder pain
changes in skin color or nails
heart palpitations
history of cancer or blood transfusions
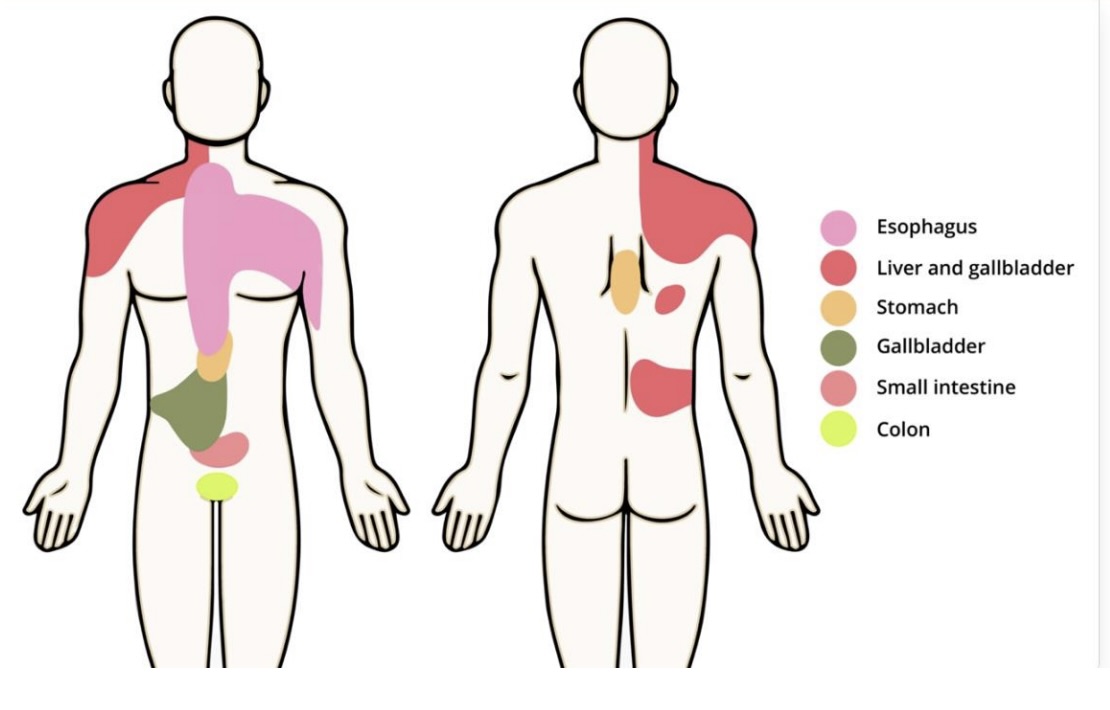
what is the referral pattern and possible signs and symptoms of the GI system?
difficulty or painful swallowing
indigestion/heartburn
excessive burping or passing of gas
change in appetite or food intolerance
nausea/vomiting
abdominal pain/distention
change in skin color
skin changes like rash or itching
change in urine color
consitpation or diarrhea
change in bowel habits
change in stool color
rectal bleeding or pain with defecation
history of GI disorders
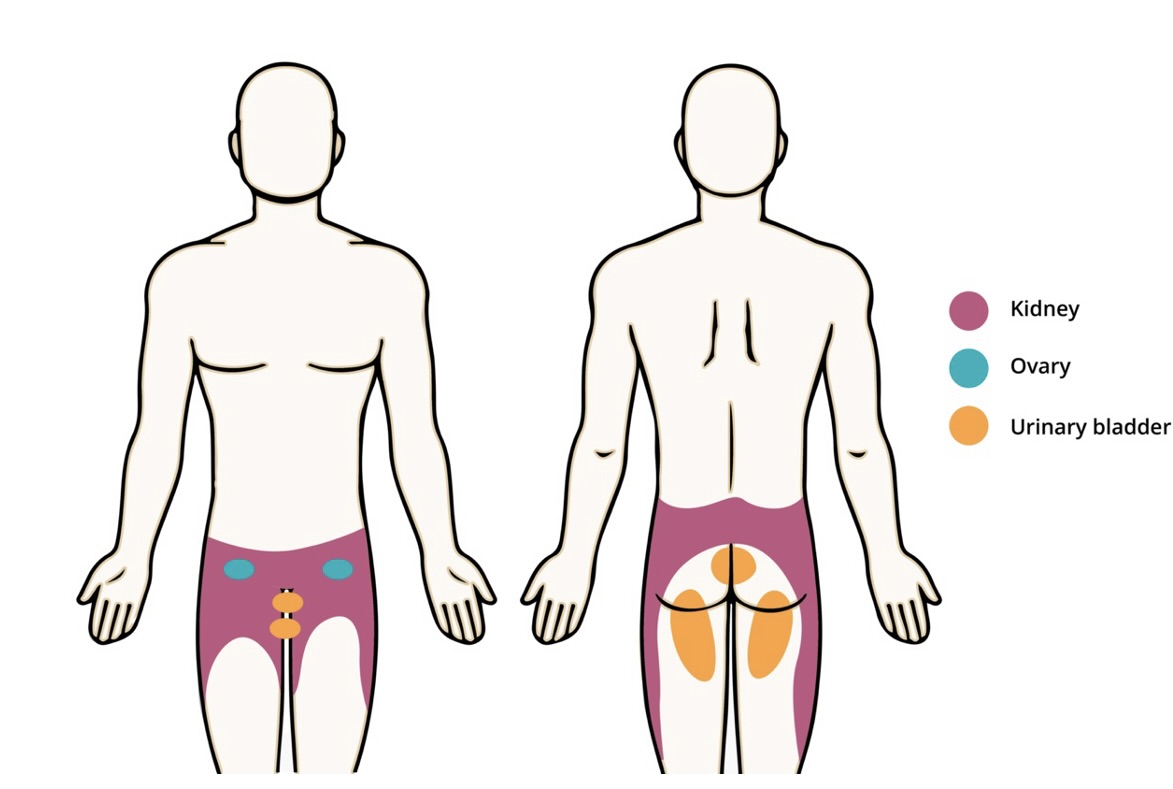
what is the referral pattern and possible signs and symptoms of the genitourinary and reproductive systems?
Genitourinary
Painful or burning with urination (dysuria)
Change in urinary frequency (decreased, excessive, urination at night)
Change in urinary control (incontinence, urgency, difficulty initiating)
Change in urinary flow or force
Blood in urine (hematuria)
Change in urine color
Suprapubic pain
Flank pain
History of genitourinary disorders (urinary tract infections, kidney infections/stones etc)
Reproductive
Male
Discharge or sores on penis
Testicular/scrotal pain, swelling or masses
Painful intercourse/ejaculation
History of sexually-transmitted infection
Female
Vaginal discharge, sores, masses
Breast pain, swelling, warmth or redness
Nipple pain or discharge
Painful intercourse
Menstruation (frequency, length of cycle, dysmenorrhea)
History of pregnancy and delivery
Menopause (peri/postmenopausal vaginal bleeding)
History of sexually-transmitted infection
what is the referral pattern and possible signs and symptoms of the neurologic system?
Changes in mood, attention, or speech
Changes in orientation, insight, or judgement
Memory changes
Headache
Lightheaded or dizziness or fainting
Vertigo
Changes in vision or hearing
History of head or spine trauma
Numbness, tingling, or weakness
Paralysis
Fall or change in balance
Tremors
Intentional movements
Seizures or loss of consciousness
Change in bowel or control of bladder
Change in muscle tone or loss of muscle
History of; neurological disease, recent surgery, or cancer
what are possible signs and symptoms of possible psychiatric problems?
Client feels sad, depressed or anxious much of the time
Alcohol or drug use/abuse
Changes in memory, confusion, etc
Nervousness, tension, irritability or sudden changes in mood
Changes in personal habits (appetite, bathing, self-care, etc.)
Suicidal ideations or intent to harm self or others
Stress levels
Sleep disturbance
History of mental health illness or treatments
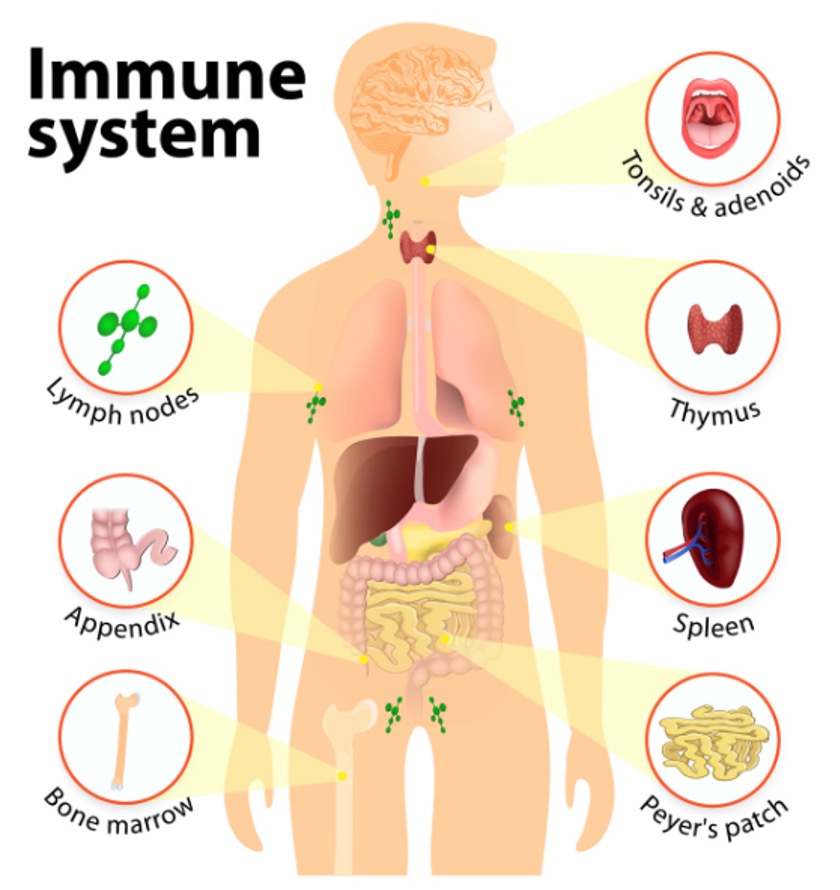
what is the referral pattern and possible signs and symptoms of the immune system?
Food allergies
Seasonal allergies
Swollen lymph nodes
Anaphylaxis or allergic reactions
Frequent infections
Changes in skin or nails
Fever, chills, night sweats, weight changes, fatigue or malaise
Joint or muscle pain, swelling, stiffness, weakness
Recent travel
History of HIV/AIDs
History of cancer
History of known rheumatological or autoimmune disorder
what are possible signs and symptoms of possible eye problems?
eye pain
red eyes
dry/teary eyes
itching eyes
eye discharge
blurred vision
double vision
loss of vision
what are possible signs and symptoms of possible integumentary problems?
skin
rashes, lumps, sores, lesions, wounds
itching, sweating, dryness, or changes in color
easily bruised
changes in color or size of moles
history of known skin disease
hair
decrease or increase in hair growth or quality
history of thyroid disease
nails
change in nail beds
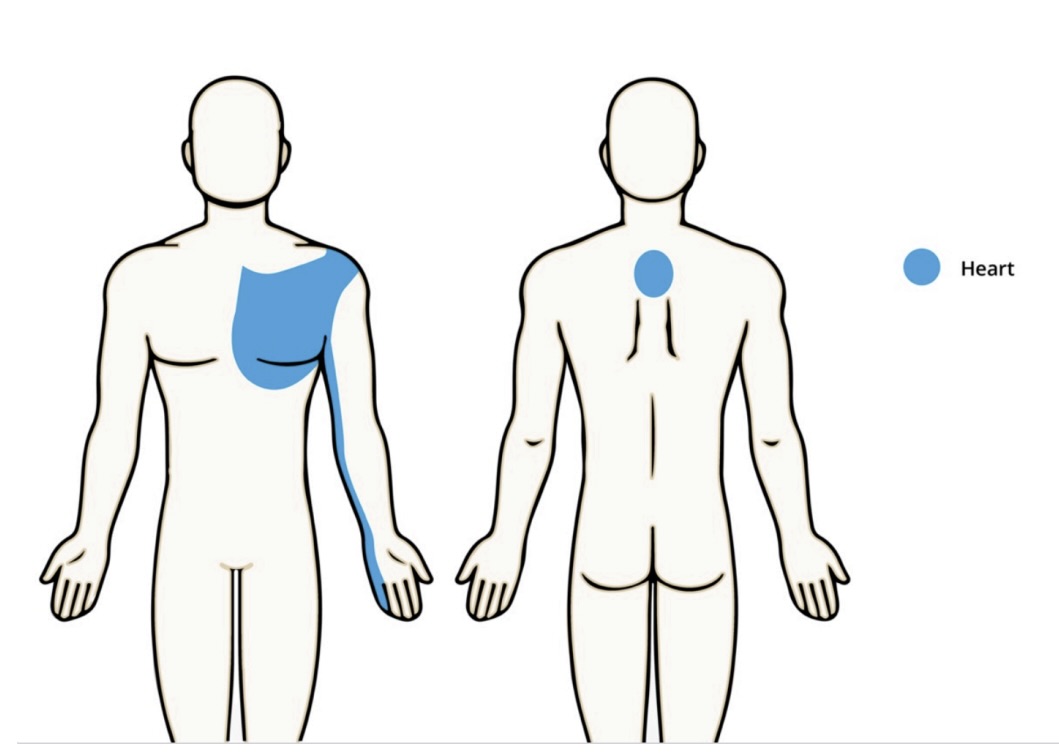
what is the referral pattern and possible signs and symptoms of the cardiovascular system?
chest pain/heaviness/discomfort
palpitations or irregular heartbeat
fatigue
lightheadedness, dizziness, or fainting
severe sudden headache
difficulty talking or swallowing
double vision
pulsating or throbbing pain
shortness of breath
high or low blood pressure
limb pain, swelling, or discoloration
limb pain during activity
wound/ulcers in legs or slow to heal
history of CV disease
what bones make up the shoulder girdle?
scapula, humerus, and clavical
what joints make up the shoulder girdle?
scapulothoracic, GHJ, acromioclavicular, sternoclavicular
where do we have the most passive support at the shoulder?
anteriorly and superiorly
where is the only place the shoulder girdle attaches to the rest of the body?
sternoclavicular joint— so it is very stable and cable of withstandings lots of force
what is the significance of the open packed position of the shoulder?
it allows for more movment of hte joint which can be helpful when trying to facilitate movement of ajoint without stressing the end range of tissues when one may be more irritable, making grade 1 and 2 mobilization more applicable. however, it needs more muscular support to stabalize
what is the significance of the closed packed position of the shoulder?
it creates more stability of the joint and brings tissues to end range which can be helpful when trying to stress stiff tisssues that are limiting motion, making grade 3 and 4 mobilizations more applicable. requires more passive stability support
what is the open and closed packed positions of the GHJ?
open: about 40 degress of abduction and 30 degrees of flexion witht he weight of the arm supported
closed: full abduction and ER
what is the open and closed pack position of the sternoclavicular joint?
open: standard anatomical position
closed: maximal posterior rotation (with the shoulder fully flexed)
what is the open and closed pack position of hte acromioclavicular joint?
open: standard anatomical position
closed: greater than 90 degrees of shoulder abduction
what makes up the arthrokinematics of the GHJ?
inert tissue (bones, capsules, and ligaments) + contractile tissue
what are the osteokinematics of the shoulder?
flexion: 0-180
abduction: 0-180
extension: 0-60
IR: 0-70
ER: 0-90
horizontal abduction: 0-45
horizontal adduction: 0-135
what allows for full flexion and abduction motion of the shoulder?
scapulohumeral rythm— the first 120 degrees comes from the GHJ while the remaining 60 degrees is achieved through scapular and clavicular upward rotation
what should the sum of shoulder IR and ER equal?
160 degrees
because of the acriomoclavicular joint, the scapula and clavicle move together how?
muscles move the scapula
the scapula pulls the clavicle along for the ride via the AC joint
the clavicle moves on the fixed sternum at the SC joint
what is happening at the clavicle during scapular upward rotation, elevation, and posterior tilt?
upward rotation (the distal end of the clavicle moves superiorly)
what is happening at the clavicle during scapular downward rotation, depression, and anterior tilt?
downward rotation (the distal end of the clavicle moves inferiorly)
what is happening at the clavicle during scapular protraction (abduction) and internal rotation (winging)?
protraction (distal end of the clavicle moves anteriorly)
what is occuring at the clavicle during scapular retraction (adduction) and ER?
retraction (distal end of the clavicle moves posteriorly)
our scapulohumeral musles serve to stabalize and move the GHJ. what are these muscles?
supraspinatus, infraspinatus, teres minor, and subscapularis
our scapulohumeral movers serve to produce strong movement at the GHJ. what are these muscles?
deltoid, teres major, biceps brachii, triceps brachii, coracobrachialis
our axioscapular muscles serve to stabalize and move the scapulothoracic joint. what are these muscles?
pec minor, serratus anterior, trapezius, levator scapulae, rhomboid major, rhomboid minor
our axiohumeral muscles are powerful movers of the shoulder girdle. what are these muscles?
pectoralis major and latissimus dorsi
what muscles are important in stabalizing our shoulder girdle against gravity?
rotator cuff
when do we care about static position of the shoulder girdle?
1.The patient’s functional limitation is related to a static position.
2.The patient’s pain changes when the static position is changed.
3.The patient’s static positions impacts tissue healing.
4.The patient cares about it.
what is the ideal position of the scapula?
positioned between T2-T7
medial border is parallel to the spine
medial border is around 3 inches from the spine
rests against the thorax
no tilting or winging
what is the ideal position of the clavicle?
AC joint should be higher than the SC joint
what is the ideal position of the humerus?
humeral head is no more than 1/3 anterior of the acromion
olecranon faces posteriorly
humeral shaft is parallel with the trunk