DSA13/15(L) - OMM: Cranial Osteopathy: Strain Pattern Diagnosis & Treatment
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
39 Terms
Somatic dysfunctions of the SBS, occurring when normal physiologic motions of flexion and extension are altered; Named by the motion of the sphenoid and characterized as physiologic or pathologic (non-physiologic)
Define Strain Pattern
head (or lightly resting above bregma)
During the Vault Hold, the thumbs should be off the ()
great wings of sphenoid
During the Vault Hold, the Index fingers should be over the ()
Zygomatic portion of temporal bone [aka on the squamous portion of temporal bone]
During the Vault Hold, the Middle fingers should be anterior to the the ()
mastoid portion of temporal bone
During the Vault Hold, the Ring fingers should be on the ()
squamous portion of the occiput
During the Vault Hold, the little fingers should be on the ()
forearms
During the Vault Hold, the fulcrum should be at the ()
SBS
Flexion and Extension of the cranium is named for the motion at the ()
-One through the body of the sphenoid
-One through the occiput
As the SBS rises in flexion & falls in extension, the motion occurs around two parallel transverse axes:
–External rotation of paired structures
–Elevation of SBS
–Widening side to side, increase distance between palms
–Narrowing A-P
–Shortening superior-inferior axis
What are the motions associated with Cranial Flexion?

When the SBS is raised, the fingers on the sphenoid move reciprocally
Why do the 4 fingers move inferiorly/caudad with Cranial Flexion?
Posteriorly (counternutation) + caudally directed wave-like motion
Which way does the Sacral base move with SBS Flexion?
–Internal rotation of paired structures
–Depression of SBS
–Narrowing side to side, palms approximate
–Widening A-P
–Lengthening superior-inferior axis
What are the motions associated with Cranial Extension?
When the SBS is depressed, the fingers on the sphenoid move reciprocally
Why do the 4 fingers move superiorly/cephalad with Cranial Extension?
Anteriorly (nutation) + cephalad directed wave-like motion
Which way does the Sacral base move with SBS Extension?
Physiologic cranial strain pattern; can be caused by birth/trauma, blow to anterior quadrant (maxilla), or blow to posterior quadrant (parietal/occiput);
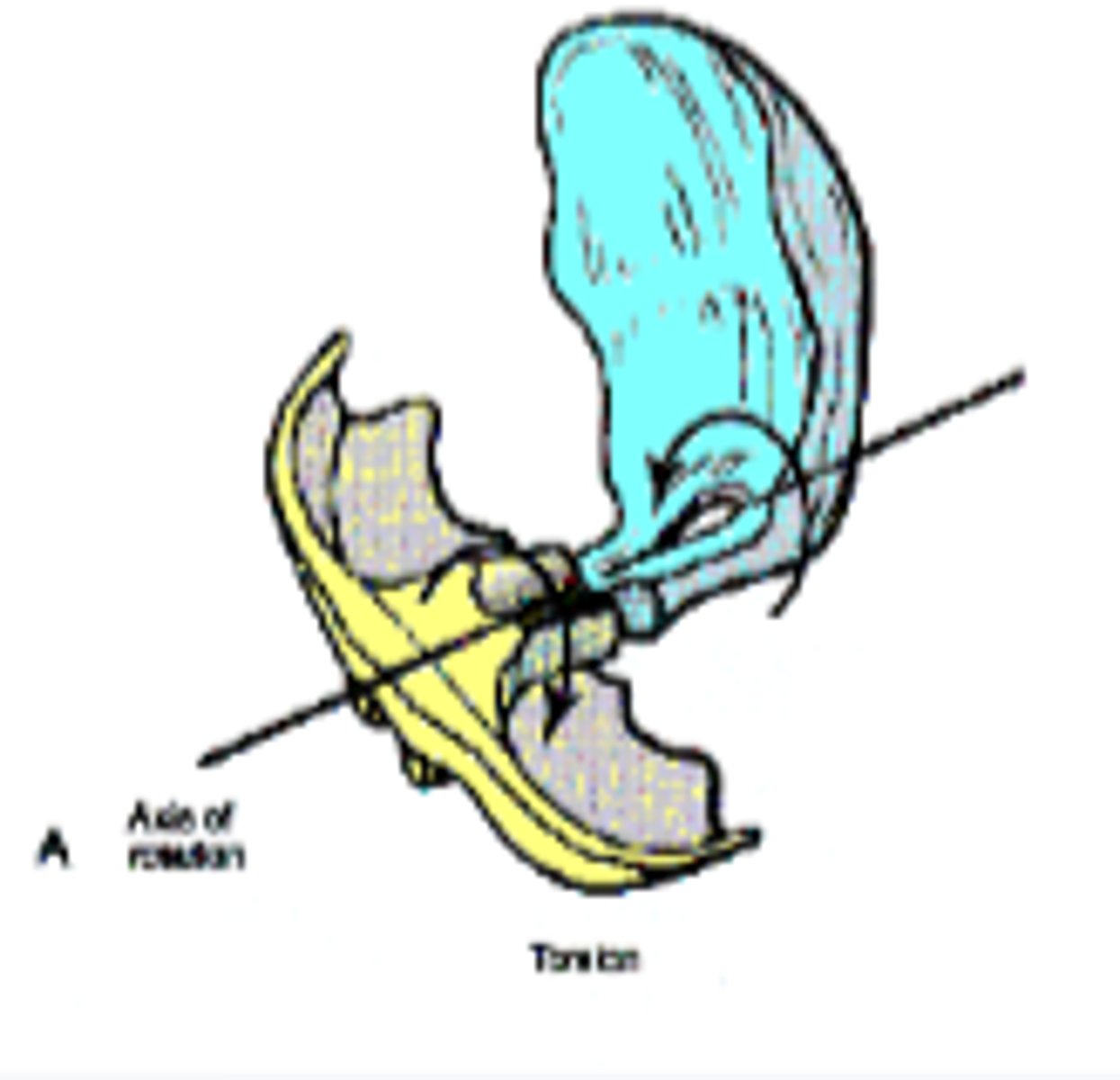
When the Sphenoid & Occiput TWIST in opposite directions
Define Cranial Torsion
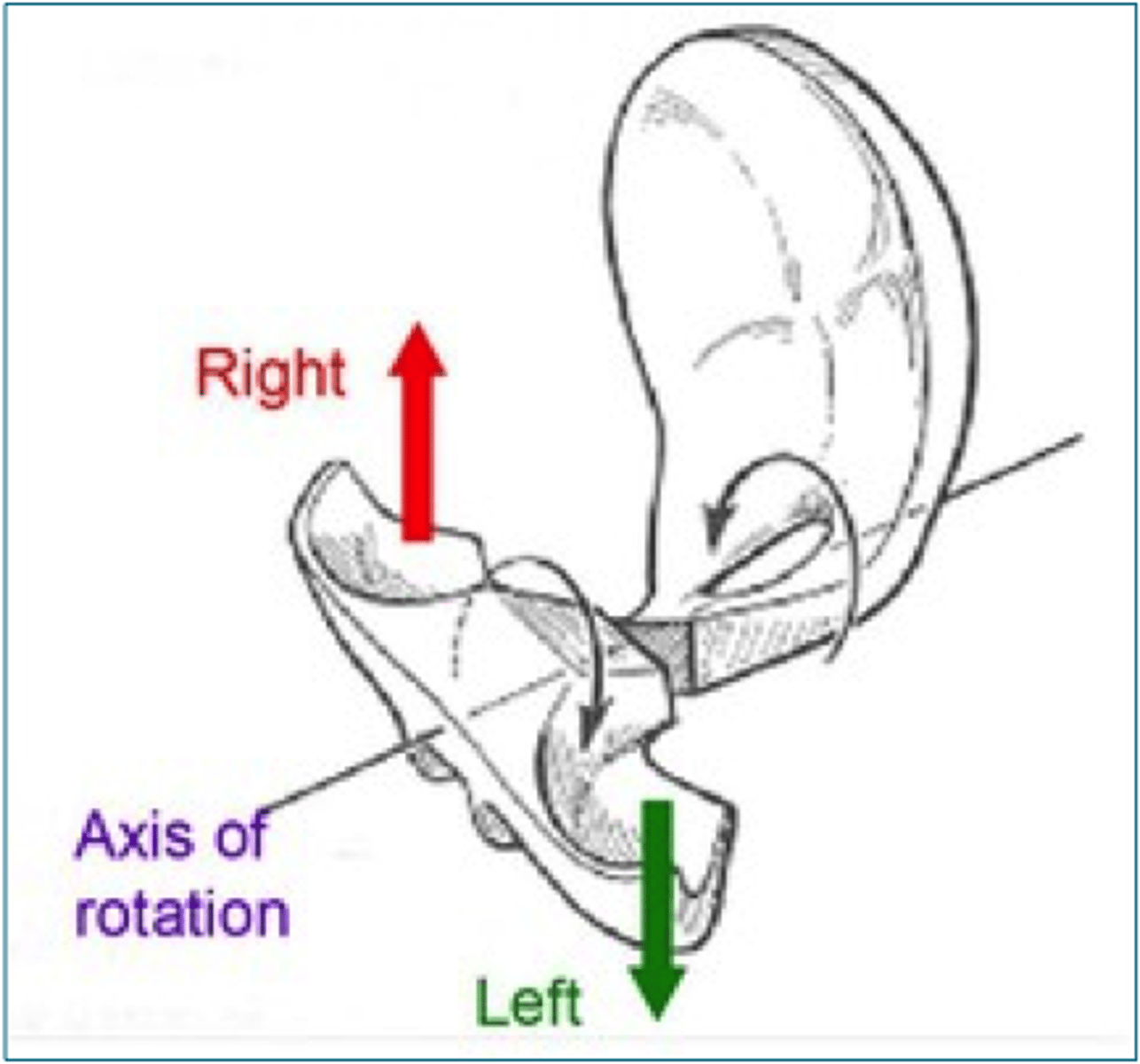
An AP axis running through SBS from Nasion (body of sphenoid) to Opisthion (foramen magnum)
What is the axis for Cranial Torsions?
For side of the more superior greater wing of sphenoid
Ex: If basisphenoid rotates superior on right, greater wing moves on right (occiput moves opposite on same side)
How is the Cranial Torsion named?
Physiologic cranial strain pattern that can be caused by trauma
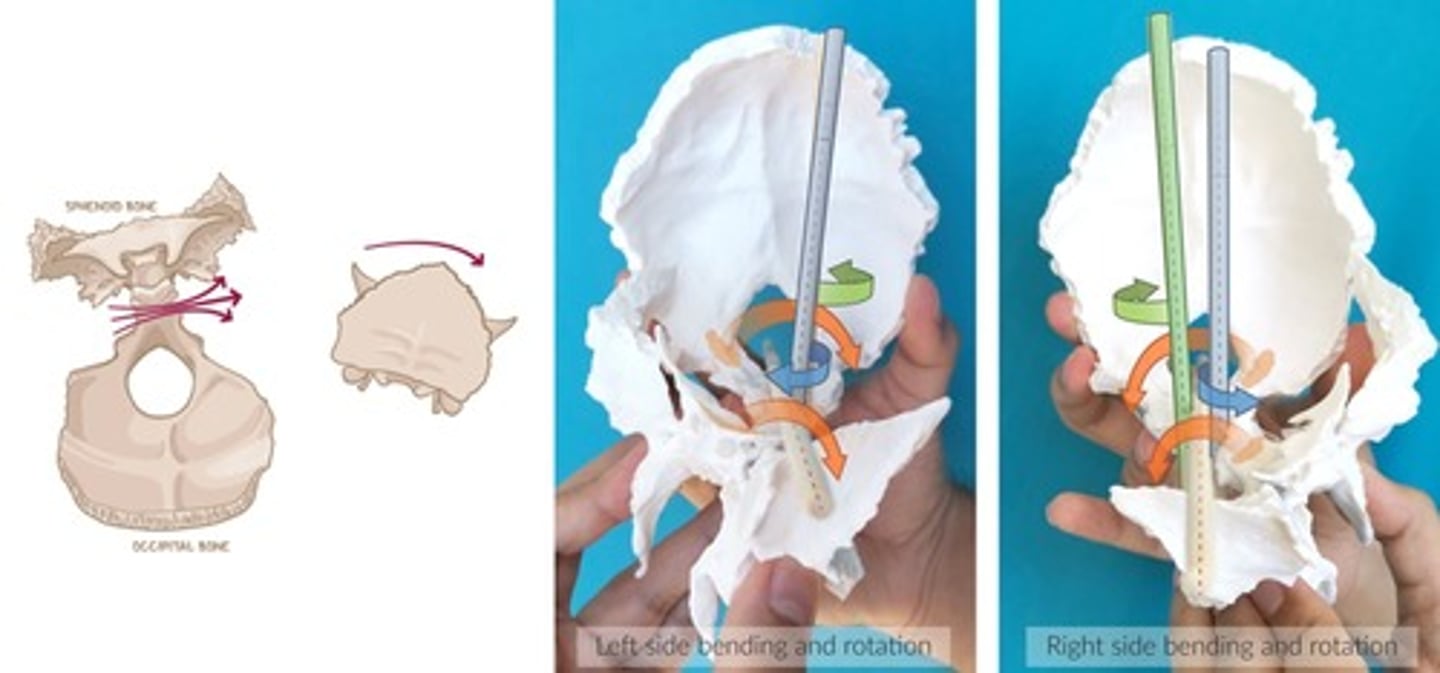
Blow to one side causes side-bending/rotation to opposite side + Sphenoid & Occiput "drop" inferiorly on AP Axis (Nasion to opisthion through the SBS)
Define Cranial Side-Bending Rotations
-One vertical axis through Sphenoid
-One vertical axis through Foramen Magnum
-1 AP axis (Nasion to Opisthion thru SBS)
What are the axes for Cranial Side-Bending Rotations?
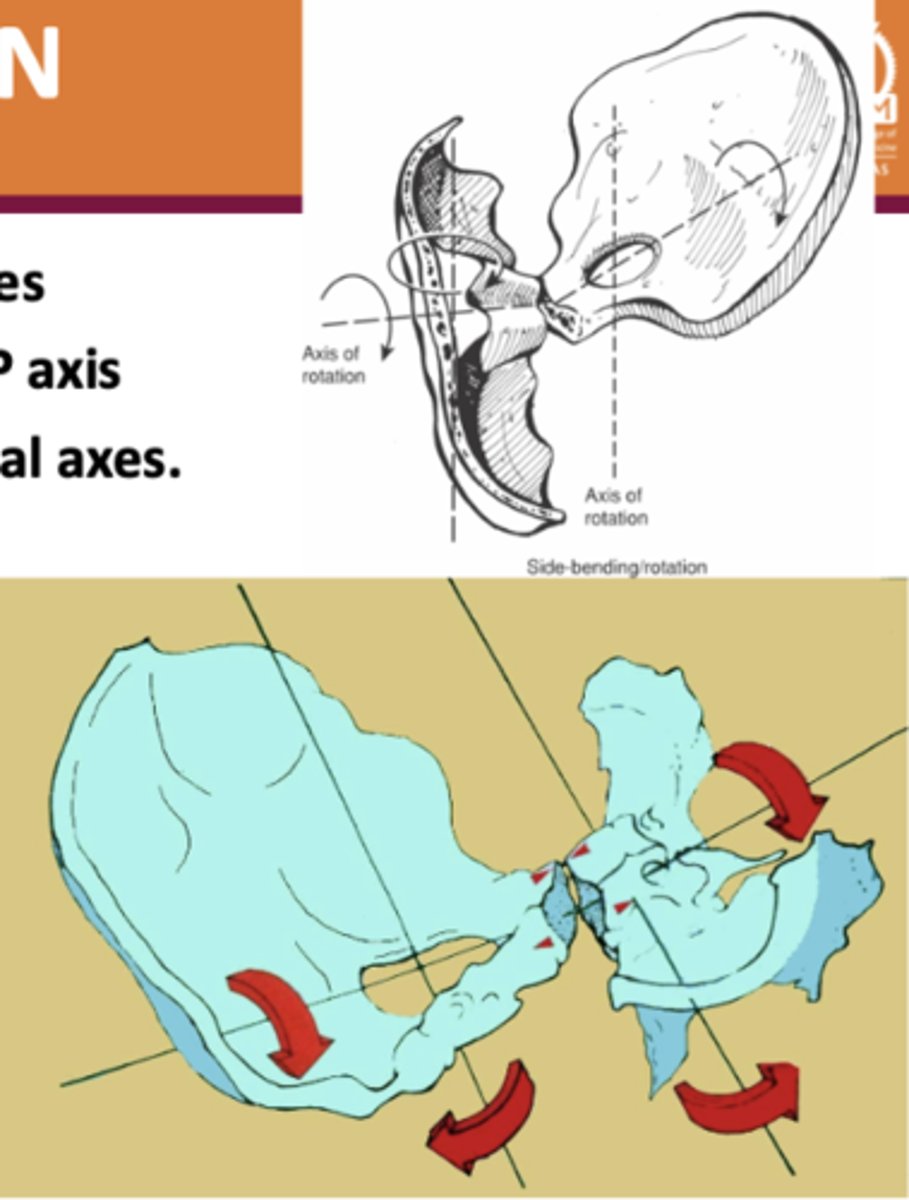
-Sphenoid rotates counterclockwise (own axis)
-Occiput rotates clockwise (own axis)
-Both sidebend around same axis
Describe the motions for Cranial Side-Bending Rotations
For side of the CONVEXITY of SBS (whichever side opens up more)
How is the Cranial Side-Bending Rotation named?
SBS remains intact during these motions
Why are Cranial Torsions & Side-Bendings still considered "physiologic" patterns, rather than "pathologic" patterns?
Disruption in synchronized flexion-extension movement of SBS (shearing or compression); often indicate previous trauma
Define Non-Physiologic (Pathologic) Strain Patterns
Non-Physiologic Strain Pattern in which the sphenoid and occiput rotate in same direction around transverse axes
Define Vertical Strain
Two transverse axes (one through base of sphenoid, one through foramen magnum/occiput)
What are the axes for Vertical Strain?

Named for position of body of sphenoid relative to base of occiput
How is the Vertical Strain named?
Sphenoid & Occiput rotate ANTERIORLY around transverse axes:
Occurs due to downward blow posterior to SBS OR upward blow anterior to SBS
*Index fingers move inferiorly, 5th digits move superiorly (WRISTS MOVE AWAY FROM YOU)*
Describe SUPERIOR Vertical Strain
Sphenoid & Occiput rotate POSTERIORLY around transverse axes:
Occurs due to downward blow anterior to SBS OR upward blow posterior to SBS
*Index fingers move superiorly, 5th digits move inferiorly (WRISTS MOVE TOWARD YOU)*
Describe INFERIOR Vertical Strain
Occurs as result of direct lateral blow; sphenoid and occiput rotate in same direction around vertical axes --> Shearing Force around SBS
Define Lateral Strain
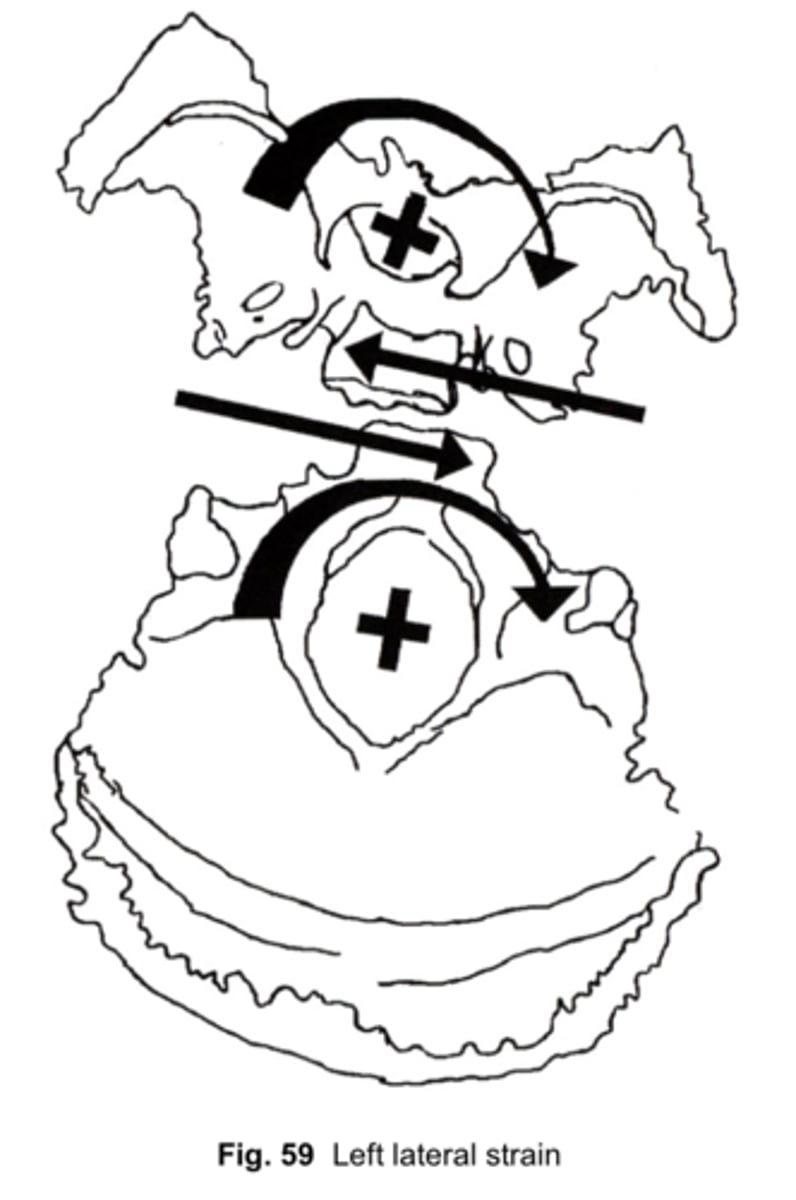
Two vertical axis axes (one through foramen magnum, one through sphenoid)
What are the axes for Lateral Strain?
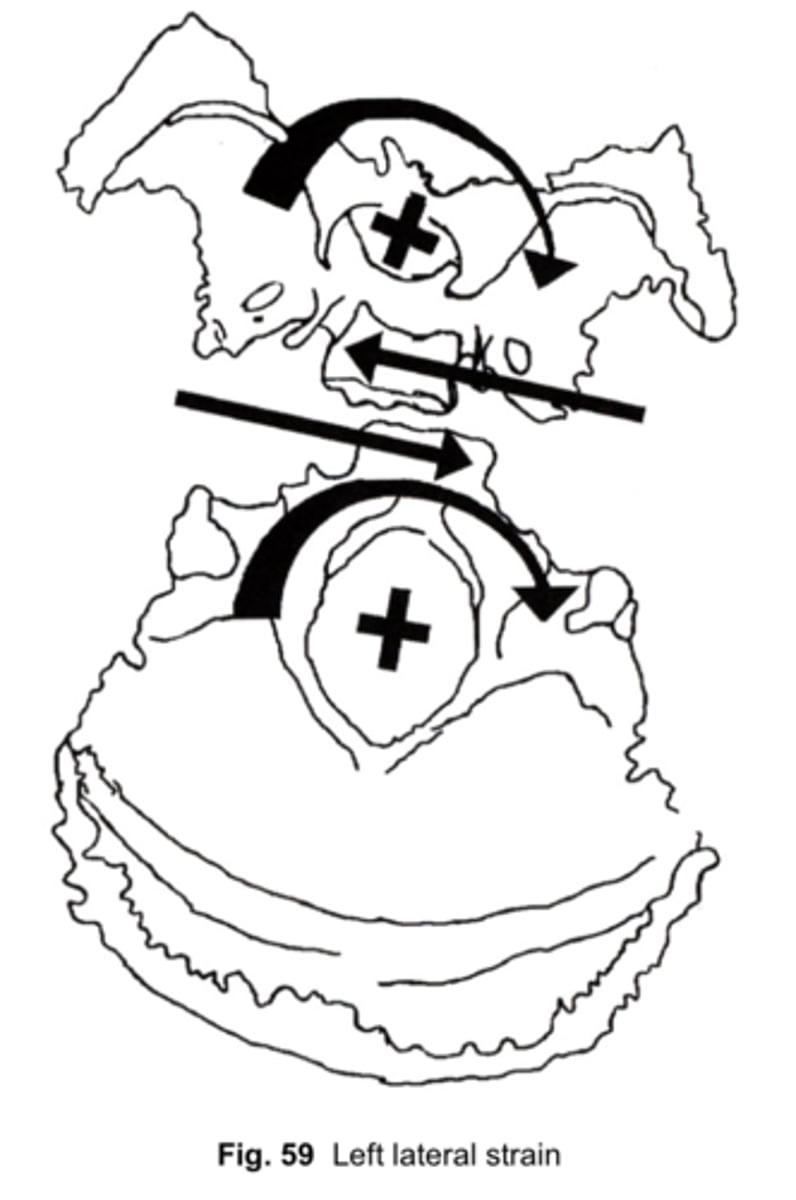
Named for position of the base of the sphenoid relative to base of occiput
How is the Lateral Strain named (using the "Rotatory Model")?
When wings of the sphenoid move to the left, while the body of the sphenoid moves to the right
Body of occiput moves to left as squama of occiput moves to right
-Index fingers move to left (right fingers move anterior)
-Pinky fingers move to right
Describe RIGHT Lateral Strain (using the "Rotatory Model")
When the Sphenoid & Occiput are compressed together (limited motion during Flexion & Extension)
Caused as result of the sphenoid and occiput being pushed together, as in a blow onto the forehead, with the force directed posteriorly and slightly inferiorly
Define SBS Compression
Named for the relationship of the body of the sphenoid to the base of the occiput (sphenobasilar synchondrosis)
How is the SBS Compression named?
-Lack of motion in both phases ("feels like a bowling ball")
-CRI decreased
-Patients may have headache, low energy, difficulty concentrating, short attention span, sluggish thinking
What are the usual findings for SBS Compression?
To balance the reciprocal tension membrane at the hypoglossal canal, permitting normalized function of Cranial nerve 12
What is the objective of the "Decompression of Occipital Condyles" technique?
Physician puts index & middle fingers (or middle & ring) as far caudad on occiput as soft tissues & C1 allows --> initiates gentle lateral & cephalad force at base of occiput, maintaining until release is felt --> Reassess CRI
How is the Decompression of Occipital Condyles performed?
-Finger pads placed in suboccipital region (find occipital ridge and move inferiorly until fingers fall into suboccipital region)
-Apply upward pressure into tissues and hold
How is Suboccipital Release performed?