Anatomy Lecture Ch. 7 - Bone Tissues
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
Osteology
the study of bone
Bones and teeth are the most durable remains of a body
Living skeleton is made of dynamic tissues, full of cells, nerves, and blood vessels
Continually remodels itself and interacts with other organ systems of the body
bones are in a constant state of fluctuation
Skeletal System
composed of bones, cartilages, and ligaments
Cartilage is the forerunner of most bones
Covers many joint surfaces of mature bone
bones start out as hyaline cartilage
ligaments —hold bones together at joints
dense regular tissue in ligaments
tendons —attach muscle to bone
7 Functions of the Skeleton
Support —limb bones and vertebrae support body; jaw bones support teeth; some bones support viscera
Protection —of brain, spinal cord, heart, lungs, and more
Movement —limb movements, breathing, and other movements depend on bone
Electrolyte balance —calcium and phosphate levels
stored in EC matrix of the bone
Acid–base balance —buffers blood against large pH changes by altering phosphate and carbonate salt levels
helps us resist changes in the pH of our bloodstream
Blood formation —red bone marrow is the chief producer of blood cells
Bone (osseous tissue)
connective tissue with the matrix hardened by calcium phosphate and other minerals
Individual bones (organs) consist of bone tissue, bone marrow, cartilage, adipose tissue, nervous tissue, and fibrous connective tissue
Mineralization (calcification)
the hardening process of bones
Long Bones
longer than wide
has rigid levers acted upon by muscles
crucial for movement
only long bones have the marrow cavity
Short Bones
Approximately equal in length and width
Glide across one another in multiple directions
completely filled with spongy bone
Flat Bones
Thin, curved plates
protects soft organs
completely filled with spongy bone tissue
Sandwich-like construction
Two layers of compact bone enclosing a middle layer of spongy bone called the diploe
absorbs shock
Irregular Bones
Elaborate shapes that do not fit into other categories
Compact Bone
dense outer shell of bone
skeleton is ¾ compact bone
completely filled with minerals
people who are physically active or weigh more have more compact bone tissue
has concentric lamellae that surround a Central Canal
Perforating canals —transverse or diagonal passages in bone that allows blood vessels and nerves to pass through
Periosteum
external sheath covering most of bone
Outer fibrous layer of collagen
Some fibers are continuous with tendons
Perforating fibers—penetrate into bone matrix
Inner osteogenic layer of bone-forming cells
Important to bone growth and healing of fractures
Osteogenic Cells
stem cells found in the endosteum and inner layer of periosteum
Arise from embryonic mesenchyme
Multiply continuously and give rise to most other bone cell types
Osteoblasts
bone-forming cells
Forms a single layer of cells under endosteum and periosteum
Synthesizes soft organic matter of matrix which then hardens by mineral deposition
Stress stimulates osteogenic cells to multiply rapidly and increase the number of osteoblasts which reinforces the bone
Osteocytes
former osteoblasts that have become trapped in the matrix they deposited
osteocyte is the maintenance cell of the bone tissue
Act as strain sensors —when stressed, they produce biochemical signals that regulate bone remodeling (shape and density changes that are adaptive)
Osteoclasts
bone-dissolving cells found on the bone surface
the cleaning crew
removes EC matrix
if not enough calcium, osteoclasts dissolves some of the EC matrix and puts the calcium into the blood stream
Very large cells formed from fusion of several stem cells
Have multiple nuclei in each cell
Cells often reside in resorption bays (pits in bone surface)
Dissolving bone is part of bone remodeling
osteoclasts raise and decrease calcium to maintain homeostasis
The Matrix of Osseous (Bone) Tissue
Matrix of osseous tissue is about one-third organic and two-thirds inorganic matter
Organic matter—synthesized by osteoblasts
Collagen, carbohydrate–protein complexes, such as glycosaminoglycans, proteoglycans, and glycoproteins
Inorganic matter
hydroxyapatite (crystallized calcium phosphate salt)
calcium carbonate
Other minerals (fluoride, sodium, potassium, magnesium)
Mineral portion gives stiffness
Polymer (protein) gives some flexibility
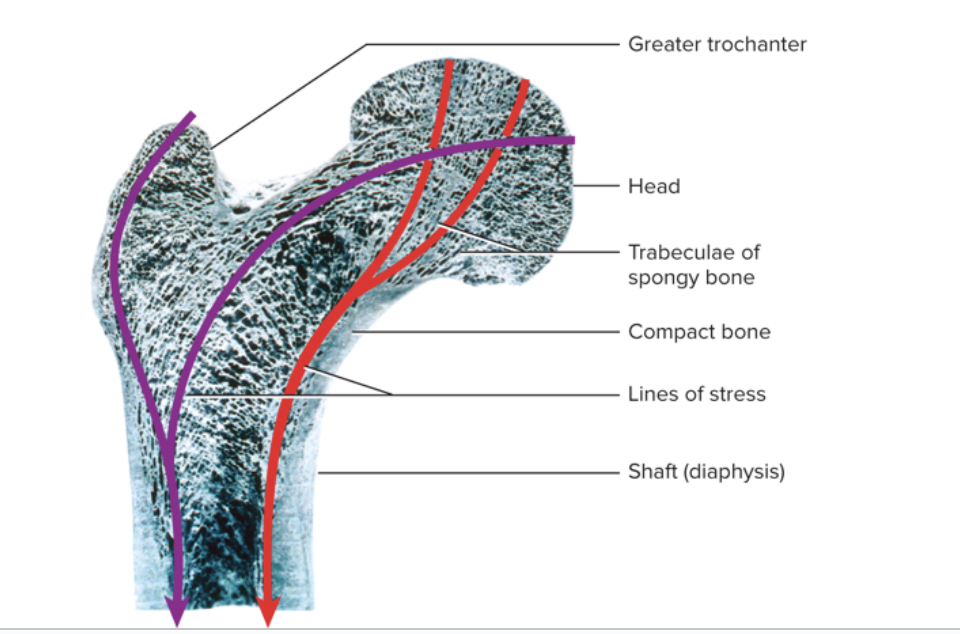
Spongy (Cancellous) Bone
loosely organized bone tissue
Found in the center of ends and center of shafts of long bones and in the middle of nearly all other bones
Covered by more durable compact bone
Spongy bone consists of:
Lattice of bone covered with endosteum
Thin plates of bone called trabeculae
Spaces are filled with red bone marrow
has few osteons and no central canals
All osteocytes are close to the bone marrow
Provides strength with minimal weight
Trabeculae develop along bone’s lines of stress
Bone Marrow
soft tissue occupying marrow cavities of long bones and small spaces of spongy bone
red and yellow bone marrow
Red Bone Marrow (myeloid tissue)
Contains hemopoietic tissue—produces blood cells
In nearly every bone in a child
In adults, this is found in the skull, vertebrae, ribs, sternum, part of pelvic girdle, and proximal heads of humerus and femur
red marrow burns through a lot of ATP
Yellow Bone Marrow
Fatty marrow that does not produce blood
found in adults
Can transform back to red marrow in the event of chronic anemia
fat storage
Ossification or Osteogenesis
the formation of bone
In the human fetus and infant, bone develops by two methods
intramembranous ossification
endochondral ossification
Ossification continues throughout life with the growth and remodeling of bones
Bones grow in two directions
Length
Width
Intramembranous Ossification
Produces flat bones from connective tissue
Thickens long bones throughout life
Endochondral Ossification
how we make primarily long bones
exclusive to youth
During infancy and childhood, the epiphyses fill with spongy bone
Cartilage is limited to the articular cartilage and epiphyseal plate
Epiphyseal plate persists through childhood and adolescence
Serves as a growth zone for bone elongation
by late teens to early 20s, all remaining cartilage in the epiphyseal plate is generally consumed
Gap between epiphyses and diaphysis closes
Primary and secondary marrow cavities unite into a single cavity
Bone can no longer grow in length
Bone Elongation
Bone elongation is a result of cartilage growth within the epiphyseal plate
length comes from epiphyseal plate
the growth from within is called interstitial growth
width comes from interstitial growth
Epiphyses close when cartilage is gone
epiphyseal line of spongy bone marks site of former epiphyseal plate
Lengthwise growth is finished
Occurs at different ages in different bones
the cell type that is active first in long bone growth is a chondroblast
Epiphyseal Plate
cartilage transitions to bone
Functions as growth zone where bone elongates
Has hyaline cartilage in the middle with transition zones on each side where cartilage is replaced by bone
Metaphysis is zone of transition facing the marrow cavity
Achondroplastic Dwarfism
Long bones stop growing in childhood
Normal torso, short limbs
Failure of cartilage growth in metaphysis
Spontaneous mutation produces mutant dominant allele
bone ossification happens early bc epiphyseal plate has defects
Pituitary Dwarfism
Lack of growth hormone
Normal proportions with short stature
pituitary dwarfism is easy to treat with growth hormones
Appositional Growth
the continual growth in diameter and thickness of bones (increasing width)
occurs at bones surface in the periosteum
is a form of intramembranous ossification
How it works:
Osteoblasts of inner periosteum deposit osteoid tissue
osteoblast becomes trapped as tissue calcifies
it lays down the matrix in layers parallel to the surface
Forms circumferential lamellae
Osteoclasts of endosteum enlarge the marrow cavity
Bone Remodeling
we remodel our bones throughout life (about 10% of our skeleton per year)
Repairs microfractures, releases minerals into blood, and reshapes bones in response to use and disuse
Remodeling is a collaborative and precise action of osteoblasts and osteoclasts
Wolff’s Law of Bone Remodeling
the architecture of bone is determined by mechanical stresses placed on it
Bony processes grow larger in response to mechanical stress
A mature bone remains…
metabolically active
has a large influence over the rest of the body by exchanging minerals with tissue fluid
Mineral Deposition (mineralization)
process in which calcium, phosphate, and other ions are taken from the blood and deposited in to the bone (to harden bone)
Osteoblasts produce collagen fibers that spiral the length of the osteon
the collagen fibers become encrusted with minerals
Mineral Resorption
process of dissolving bone and releasing minerals into blood
Performed by osteoclasts at ruffled border (HCl at the border)
HCl dissolves bone minerals
Acid protease enzyme eats the collagen
Phosphate in the body
involved in bone structure, DNA, RNA, ATP, phospholipids, and pH buffers
Calcium in the body
involved in bone structure, neuron communication, muscle contraction, initiates blood clotting, and exocytosis
majority of the calcium in our body is stored in our bones
About 18% of skeletal calcium is exchanged with blood each year
there is calcium in blood plasma that can diffuse across capillary walls and tissues
Minerals are stored…
in the skeleton and withdrawn when they are needed for other purposes
Hypocalcemia
not enough calcium in the blood
Changes membrane potentials and causes overly excitable nervous system and tetany (muscle spasms)
Caused by vitamin D deficiency, diarrhea, thyroid tumors, and under-active parathyroid glands
Pregnancy and lactation cause an increased risk of hypocalcemia
Hypercalcemia
too much calcium in the blood
Makes ion channels less responsive and thus nerve and muscle are less excitable
Can cause emotional disturbance, muscle weakness, sluggish reflexes, cardiac arrest, or kidney stone formation
this rarely occurs
Calcium Homeostasis
Calcium homeostasis depends on a balance between dietary intake, urinary and fecal losses, and exchanges between osseous tissue
Calcium homeostasis is regulated by three hormones:
Calcitriol
Calcitonin
Parathyroid hormone (PTH)
loss of calcium homeostasis disrupts functions of other organ systems, especially electrically active tissues
Calcitriol
a hormone that is the most active form of vitamin D and raises blood calcium level
it increases calcium absorption using the small intestine
digestive absorption is the primary method to absorb calcium into bloodstream
It also increases calcium resorption from the skeleton by stimulating osteoblasts to release a chemical that stimulates production of more osteoclasts
It weakly promotes kidney reabsorption of calcium ions, so there is less lost in urine
synthesized from UV light, then gets processed through the skin, liver, and then to the kidney to get calcitriol
necessary for bone deposition—helping provide enough calcium and phosphate
Inadequate calcitriol results in abnormal softness of bones in children (rickets) and in adults (osteomalacia)
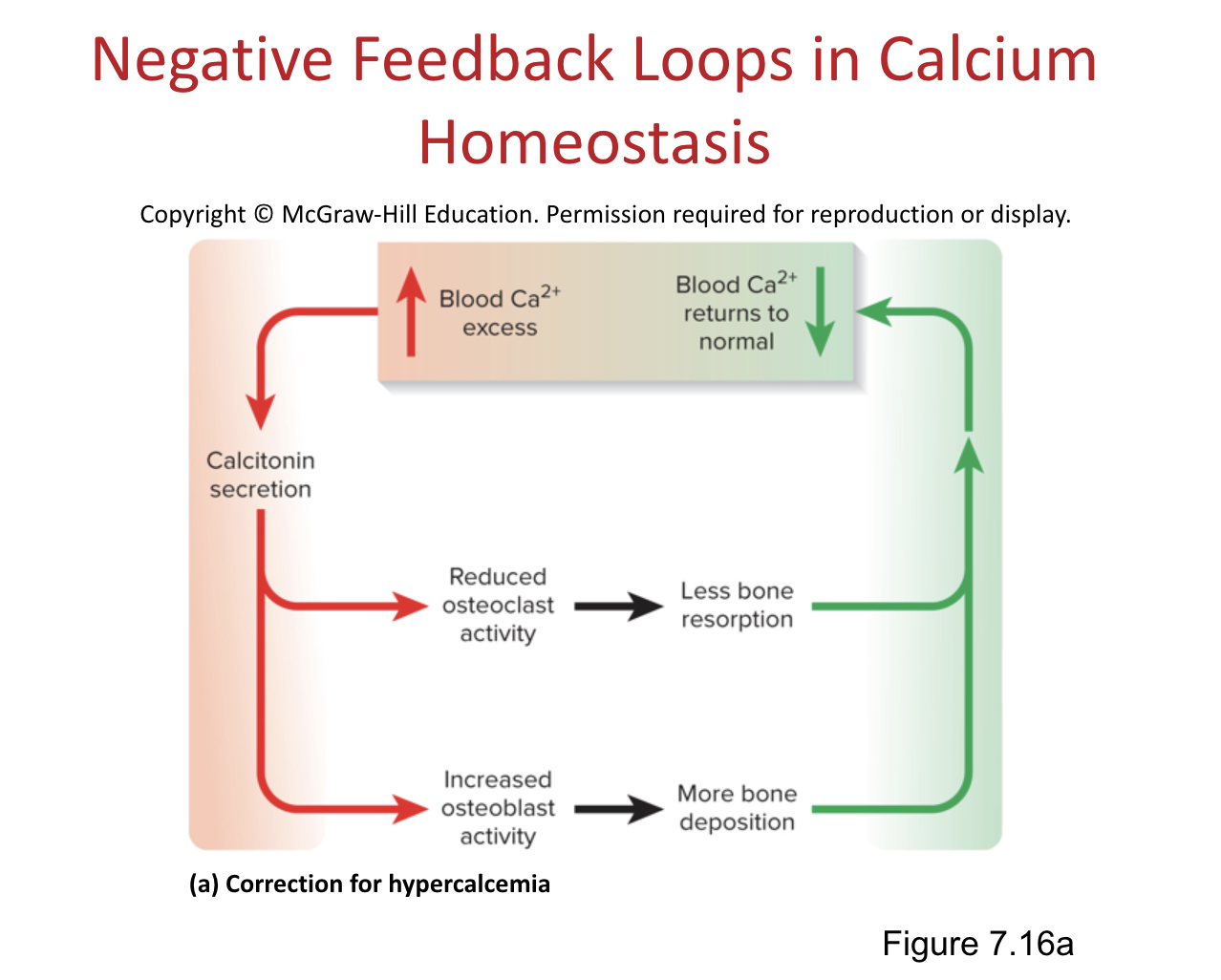
Calcitonin
a hormone secreted by C cells (clear cells) of the thyroid gland when blood calcium levels rise too high
Lowers blood calcium concentration in 2 ways:
inhibits osteoclasts thereby reducing bone resorption
stimulates osteoblasts to deposit calcium into bone
is important in children, but has a weak effect in adults
Osteoclasts are more active in children due to faster remodeling
helps inhibit bone loss in pregnant and lactating women
Negative feedback loop to correct hypercalcemia:
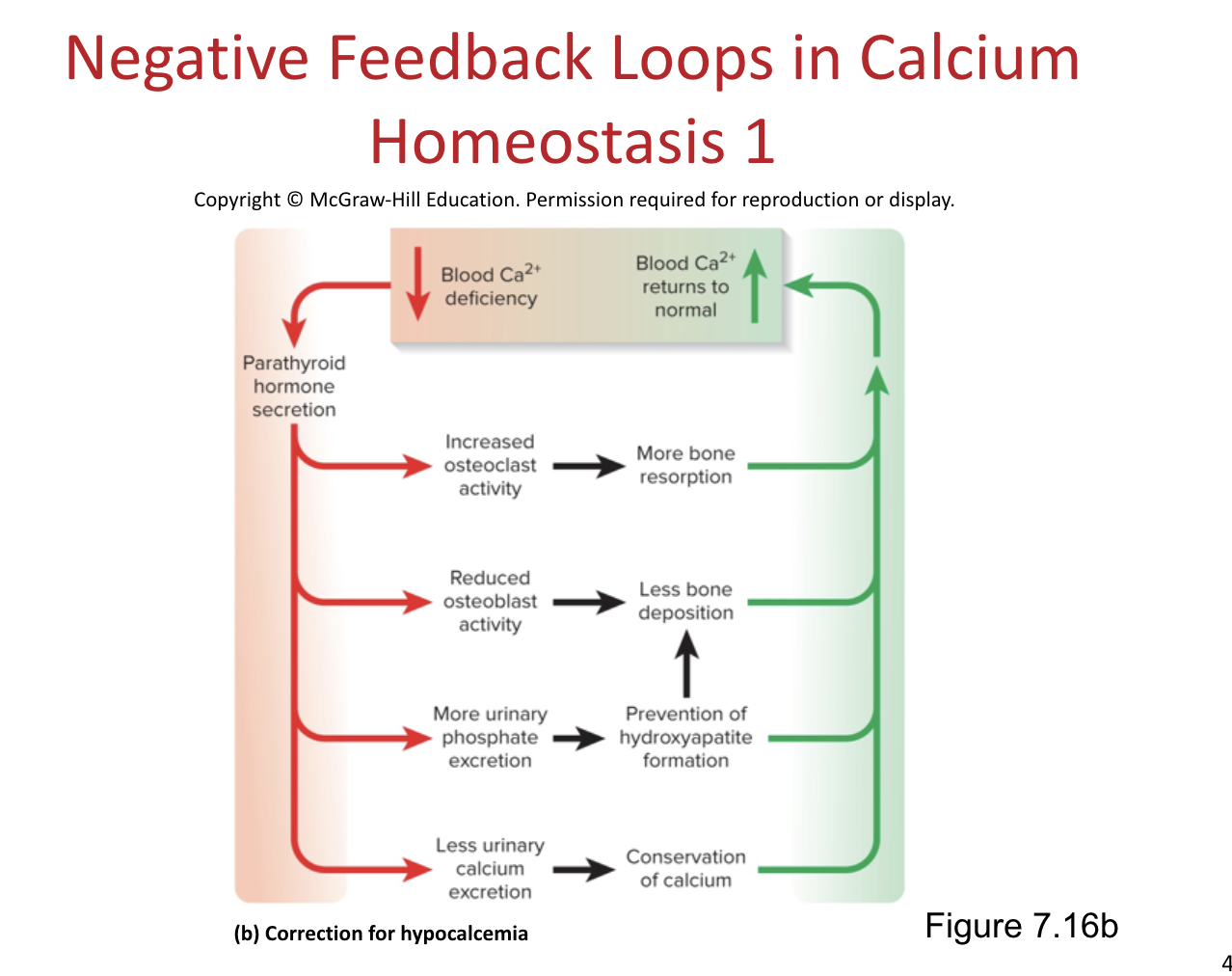
Parathyroid Hormone (PTH)
a hormone secreted by parathyroid glands on the posterior surface of the thyroid
PTH is released when calcium levels are low in the blood
PTH raises calcium blood level by 4 mechanisms:
Increasing osteoclast population and bone resorption
Promotes calcium reabsorption by kidneys, so less lost in urine
Promotes the final step of calcitriol synthesis in the kidneys, enhancing calcium-raising effect of calcitriol
Inhibits collagen synthesis by osteoblasts, inhibiting bone deposition
Negative feedback loop to correct hypocalcemia:
Phosphate Homeostasis
most of our phosphate is stored in our bones
we have phosphate in our blood plasma, but not as much as there is calcium
Phosphate levels are not regulated as tightly as calcium levels
Calcitriol raises phosphate levels by promoting its absorption by the small intestine
PTH lowers blood phosphate levels by promoting its urinary excretion
Bone Growth in Puberty
Bone growth is especially rapid in puberty and adolescence
Surges of growth hormone, estrogen, and testosterone occur and promote ossification (bone building)
These hormones stimulate the multiplication of osteogenic cells, matrix deposition by osteoblasts, and chondrocyte multiplication and hypertrophy in metaphyses
Girls grow faster than boys and reach full height earlier because estrogen has a stronger effect than testosterone on bone growth
Males grow for a longer time and also taller
Anabolic Steroids
cause growth to stop
Epiphyseal plate “closes” prematurely
Results in abnormally short adult stature
Orthopedics
branch of medicine dealing with prevention and correction of injuries and disorders of bones, joints, and muscles
Includes the design of artificial joints and limbs and the treatment of athletic injuries
Stress Fracture
a break caused by abnormal trauma to a bone
ex) in a fall
Pathological Fracture
break in a bone weakened by disease (such as bone cancer or osteoporosis)
Usually caused by a stress that would not break a healthy bone
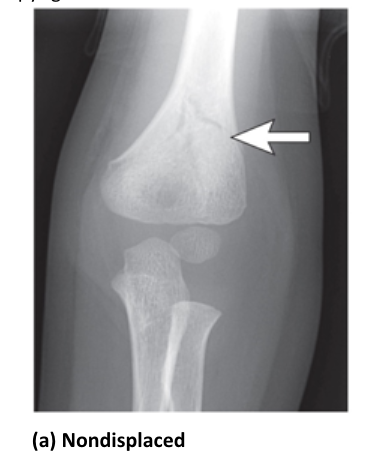
Non-Displaced Fracture
the fragments of the fracture are still aligned
Displaced Fracture
fracture with shifted fragments
bone needs to be set before healing

Comminuted Fracture
fracture with more than 2 pieces

Greenstick Fracture
a partial fracture
mostly seen only in young children

Compound Fracture
broken bone sticks out of the skin
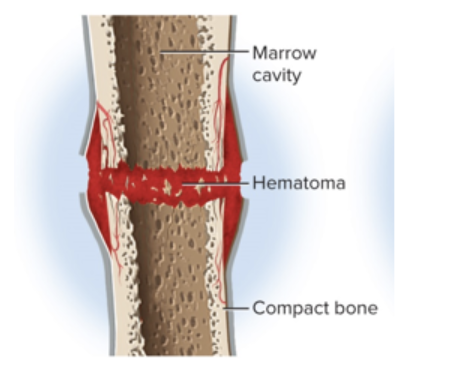
Steps to Healing a Fracture
Hematoma formation
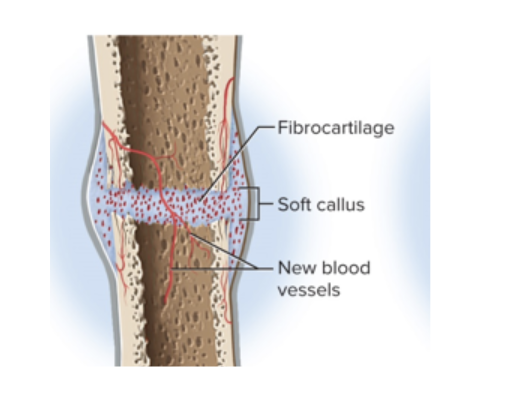
Soft callus formation
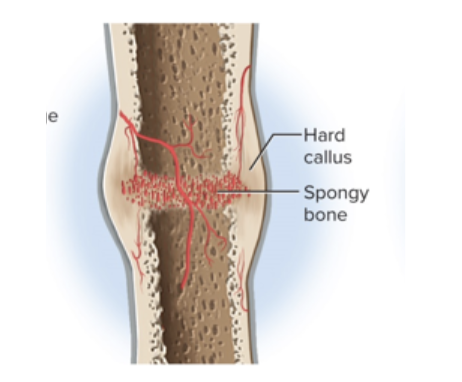
Hard callus formation
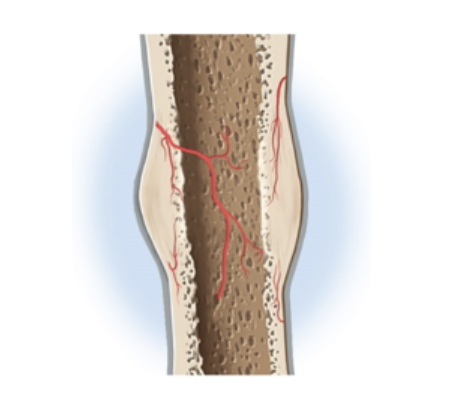
Bone Remodeling
Hematoma Formation
The hematoma is converted to granulation tissue by the invasion of cells and blood capillaries
periosteum helps keep the blood clot in place
Soft Callus Formation
the deposition (deposit) of collagen and fibrocartilage converts granulation tissue to a soft callus
Hard Callus Formation
Osteoblasts deposit a temporary bony collar around the fracture to unite the broken pieces while ossification (bone building) occurs
Bone Remodeling
Small bone fragments are removed by osteoclasts, while osteoblasts deposit spongy bone and then convert it to compact bone
where bone has been broken, compact bone replaces it
your bone becomes stronger after breaking it
Closed Reduction
procedure where bone fragments are manipulated into their normal positions without surgery
Open Reduction
involves surgical exposure of the bone and the use of plates, screws, or pins to realign the fragments
Traction
the act of applying a controlled pulling force to a broken bone or body part to realign it into proper position and stabilize it, often using weights and pulleys
used often for healing children’s femoral fractures
Osteoporosis
Severe loss of bone density
the most common bone disease
Bones lose mass and become brittle due to loss of organic matrix and minerals
brittle bones from osteoporosis fracture and heal slowly due to decreased protein synthesis
Affects spongy bone the most since it is the most metabolically active
Subject to pathological fractures of hip, wrist, and vertebral column
the loss is severe enough to compromise a person’s physical activity and health
Kyphosis
a deformity of spine due to vertebral bone loss
aka widow’s hump
Complications of loss of mobility are pneumonia and thrombosis
Estrogen
hormone that maintains bone density in both sexes
inhibits resorption by osteoclasts
Who is most at risk for osteoporosis?
Postmenopausal white women at greatest risk
Ovaries cease to secrete estrogen
White women begin to lose bone mass as early as age 35
can also be seen in young female athletes with very low body fat
Risk factors:
race, age, gender, smoking, diabetes mellitus, diets poor which are poor in: calcium, protein, vitamins C and D
Treatments for Osteoporosis
Estrogen replacement therapy (ERT)
slows bone resorption, but increases risk of breast cancer, stroke, and heart disease
Drugs Fosamax and Actonel
destroy osteoclasts
PTH injection
slows bone loss if given daily
prevention - the best treatment, includes exercise and good diet
Osteopenia
loss of bone mass