N3TT3 - Shutting Down
1/236
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
237 Terms
College of Nurses of Ontario (2017). Consent.
The Health Care Consent Act (HCCA) #1
- The goals of the HCCA include promoting individual authority and autonomy, facilitating communication between health care practitioners and their clients, and ensuring a significant role for family members when the client is incapable of consenting
- The HCCA deals separately with consent to treatment, consent to a care facility and consent to a personal assistance service. In all cases, consent must be given by a capable person
- Consent to treatment, and assessing the capacity to consent to treatment, must relate to a specific treatment or plan of treatment. A person could be capable of giving consent to one treatment, but incapable with respect to another
- Consent to treatment involves an ongoing process that can change at any time
- Health care practitioners have no authority to make treatment decisions on behalf of clients, except in an emergency when no authorized person is available to make the decisions. Similarly, they have no authority to make a decision to consent to the admission of a client to a care facility, except in a crisis
- Assessing the client's capacity to make a treatment decision is the responsibility of the health care practitioner proposing the treatment
The Health Care Consent Act (HCCA) #2
- An evaluator determines client capacity to make a decision about admission to a care facility or a personal assistance service. Registered Nurses (RNs), Registered Practical Nurses (RPNs) and Nurse Practitioners (NPs) may be evaluators
- The client has the right to ask the Consent and Capacity Board (CCB) to review the finding of incapacity
- Minor adjustments to a treatment plan for an incapable client can be made without having to seek repeated consent from a substitute decision-maker
- One health care practitioner can propose a plan of treatment and obtain consent to the plan on behalf of all the health care practitioners involved in the plan
- When a health care practitioner finds a client is incapable of making a treatment decision, the legislation requires the practitioner to provide the client with information about the consequences of the finding. This provision of information must be performed in accordance with guidelines established by the practitioner's governing body
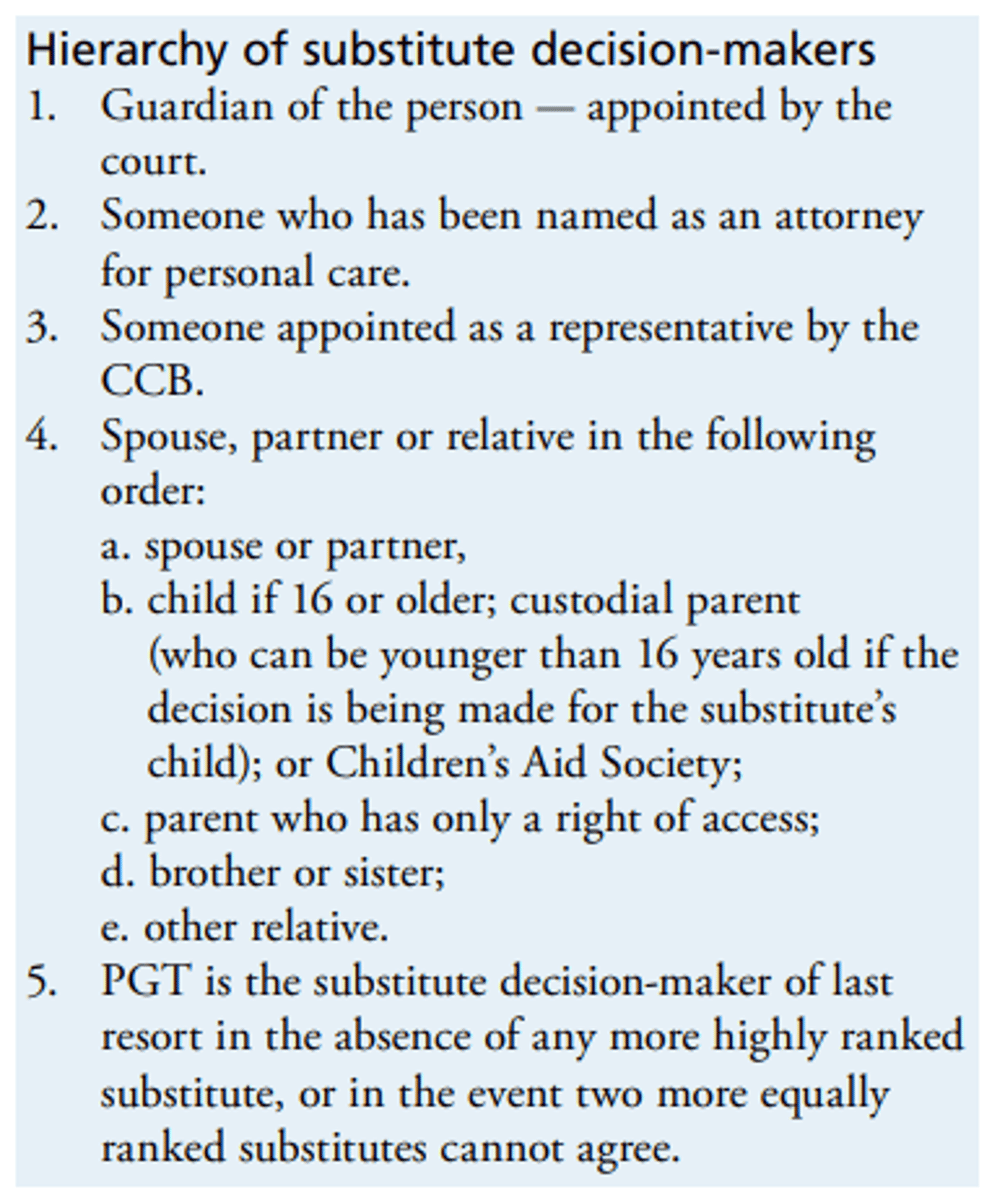
- A family member acting as a substitute decision-maker is not required to make a formal statement verifying his/her status. The legislation does contain a hierarchy of substitute decision-makers
- A person's wishes about treatment, admissions or personal assistance services may be expressed orally, in writing, in any other form, or they may be implied
Substitute Decision Act (SDA)
- Whereas the HCCA is concerned with the capacity to make decisions in relation to specific treatment, admission to care facilities or personal assistance services, the SDA is concerned with persons who need decisions made on their behalf on a continuing basis
- An individual may designate a specific person to make decisions about his/her personal care or treatment in the event that he/she becomes incapable. The person may also express his/her wishes about the kinds of decisions to be made or factors to guide decisions
- The Office of the PGT is the government department that deals with personal care and property matters
- Only trained capacity assessors may determine capacity for the purpose of the SDA (i.e. the capacity to make decisions on an ongoing basis). The HCCA requires assessment of capacity to make decisions about a specific treatment
- A power of attorney for personal care comes into effect when the person who granted it becomes mentally incapable, unless it states otherwise
- A person under statutory guardianship may apply to the CCB for a review of a finding of incapacity
Substitute Decision-Maker
- A person identified by the HCCA who may make a treatment decision for someone who is incapable of making his/her own decision
- The HCCA provides a hierarchy to determine who is eligible to be a substitute decision-maker
- The substitute decision-maker is usually a spouse, partner or relative
- A power of attorney for personal care is not necessarily required to act as a substitute decision-maker
Consent & Capacity Board (CCB)
- A board established by and accountable to the government. Its members are appointed by the government
- The Board considers applications for review of findings of incapacity, applications relating to the appointment of a representative, and applications for direction regarding the best interests and wishes of an incapable person
Spouse
- Two persons who are married to each other, or who are living in a conjugal relationship and have cohabited for at least a year, or who are the parents of a child or who have a cohabitation agreement under the Family Law Act
Power of Attorney for Personal Care
- A legal document in which a capable person gives someone else the authority to make decisions about his/her personal care in the event that he/she becomes incapable
- The document could also contain specific instructions about particular treatment decision
Continuing Power of Attorney for Property
- The same as the power of attorney for personal care, except relating to decisions about property
Need for Consent
- Nurses are accountable for obtaining consent whether the intervention or service relates to a treatment (as defined in the HCCA or as required in common law), admission to a facility, or the provision of a personal assistance service
Consent to Treatment
Consent is required for any treatment except treatment provided in certain emergency situations. The consent must:
- Relate to the treatment being proposed
- Be informed
- Be voluntary
- Not have been obtained through misrepresentation or fraud
Consent to Admission to a Care Facility
- The HCCA does not specify that consent to a personal assistance service is required
- It does, however, provide that if an evaluator finds a recipient of a personal assistance service incapable of giving consent, and the person providing the service wants to obtain consent, it may be obtained from a substitute decision-maker using the hierarchy set out in the Act
Informed Consent
What is informed consent? Consent is informed if, before giving it:
- The person received the information about the treatment that a reasonable person in the same circumstances would require to make a decision
- The person received responses to his/her requests for additional information about the treatment
The information must include the:
- Nature of the treatment
- Expected benefits of the treatment
- Material risks and side effects of the treatment
- Alternative courses of action
- A likely consequences of not having the treatment
Step #1: Assess Capacity - Steps to Obtain Consent
Capacity:
- A person is capable of giving consent to a treatment, admission to a care facility and personal assistance services if he/she: Understands the information that is relevant to making a decision concerning the treatment, admission or personal assistance service; Appreciates the reasonably possible consequences of a decision or lack of a decision
Age of consent:
- There is no minimum age for giving consent
- Health care practitioners and evaluators should use professional judgment, taking into account the circumstances and the client’s condition, to determine whether the young client has the capacity to understand and appreciate the information relevant to making the decision
Role of Evaluator:
- An evaluator must determine capacity in the case of admission to a care facility or provision of personal assistance services
- The evaluator may be the person proposing the admission or services, or the evaluator may be identified by facility or agency policies
- Nurses and some other health care professionals may be evaluators
Role of Capacity Assessor:
- A capacity assessor conducts assessments of capacity on persons who need decisions made on their behalf on a continuing basis
- NPs and RNs are eligible to become capacity assessors
- Designation will require the successful completion of a capacity assessor education or training course approved or required by the attorney general
Incapable Person:
- Incapable person If a person is incapable, the consent (or refusal to give consent) is to be obtained from the highest-ranked available substitute decision-maker from the HCCA hierarchy who is willing to make the decision
- If there is no other substitute decision-maker, the PGT is the substitute decision-maker of last resort
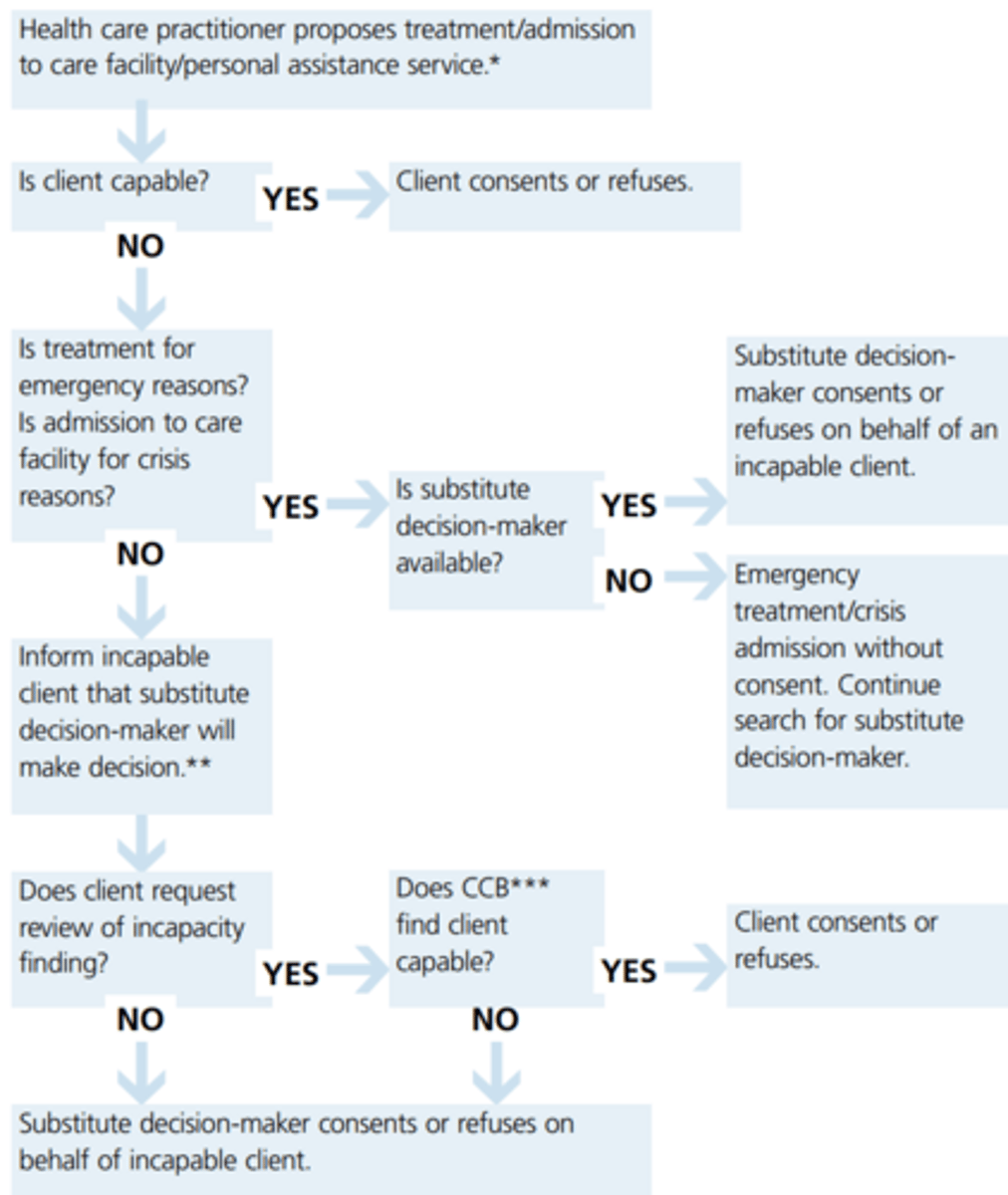
Step #2: Provide Emergency Treatment or Crisis Admission - Steps to Obtain Consent
Treatment in an emergency can be provided immediately:
- If the person is capable of giving consent and provides the consent
- In situations where: Communication can’t take place because of a language barrier or disability; Reasonable efforts to overcome the barrier or disability have been made, but a delay will prolong the suffering the person is apparently experiencing or will put the person at risk of sustaining serious bodily harm, and there is no reason to believe the person does not want the treatment
- Incapable with respect to the treatment decision but a substitute decision-maker is available to give consent
- Incapable with respect to a treatment, a substitute decision-maker is not readily available, it is not reasonably possible to obtain a consent or refusal from the substitute, and a delay will put the person at risk of sustaining serious bodily harm
Crisis Admission:
- For the purpose of an admission to a care facility without consent, a crisis relates to the condition or circumstances of the person who is to be admitted to the care facility
- Admission to a care facility without consent may be authorized if: The person who has been deemed incapable requires immediate admission as a result of a crisis; It is not reasonably possible to obtain immediate consent or refusal on the incapable person’s behalf
Step #3: Inform the Client that a Substitute Decision-Maker will Make Decision - Steps to Obtain Consent
- When the decision is made that the client is incapable and a substitute decision-maker will make the treatment decisions, or the decision to admit to a care facility, a nurse needs to follow the specific guidelines relating to advising clients of their rights
Step #4: Identify a Substitute Decision-Maker - Steps to Obtain Consent
- If a health practitioner or evaluator finds that a person is incapable of making a decision about a treatment or admission to a care facility, consent must be obtained from a substitute decision-maker
- A spouse, partner or relative who is present when the treatment is proposed may make the decision unless there is another person appointed, or people present are not willing to assume responsibility
- A formal statement that the person is the substitute decision-maker is not necessary to give or refuse consent to a treatment, admission to a care facility or a personal assistance service on behalf of an incapable person
Step #5: Obtain Consent from the Substitute Decision-Maker - Steps to Obtain Consent
- The substitute decision-maker giving or refusing consent is expected to make decisions based on the client's known wishes, which the client expressed when he/she was 16 years of age or older and capable
If such wishes are not known, or are impossible to comply with, then the substitute decision-maker decides in the client's best interests, taking into account:
- The client's values and beliefs
- The impact of the treatment on the client's condition or well-being
- Whether the benefit outweighs the risk of harm
- Whether a different treatment would be as beneficial
Hierarchy of Substitute Decision-Makers
Partners
- Two persons who have lived together for at least one year and have a close personal relationship that is of primary importance in both persons' lives
Relatives
- Two persons related by blood, marriage or adoption
Public Guardian & Trustee (PGT)
- The PGT is the substitute decision-maker of last resort for a mentally incapable person
- The court will not appoint the PGT as guardian of property or guardian of the person unless there is no other suitable person available and willing to be appointed
Advocating for Clients
- Nurses are professionally accountable for acting as client advocates and for helping clients understand the information relevant to making decisions to the extent permitted by the client's capacity
Advocating for Clients by Legislation
- If the nurse proposing a treatment or evaluating capacity to make an admission or personal assistance service decision determines the client is incapable of making the decision, then the nurse informs the client that a substitute decision-maker will be asked to make the final decision. This is communicated in a way that takes into account the particular circumstances of the client's condition and the nurse-client relationship
- If there is an indication that the client is uncomfortable with this information, then the nurse explores and clarifies the nature of the client's discomfort. If it relates to the finding of incapacity, or to the choice of substitute decision-maker, then the nurse informs the client of his/her options to apply to the CCB for a review of the finding of incapacity, and/ or for the appointment of a representative of the client's choice
- If there is an indication that the client is uncomfortable with the finding of incapacity when the finding was made by another health care practitioner, then the nurse explores and clarifies the nature of the client's discomfort. If it relates to the finding of incapacity, or to the choice of substitute decision-maker, then the nurse informs the health care practitioner who made the finding of incapacity and discusses appropriate follow-up
- The nurse uses professional judgment and common sense to determine whether the client is able to understand the information. It would not be reasonable in these circumstances for the nurse to inform the client that a substitute decision-maker will be asked to make a decision on his/her behalf
- The nurse uses professional judgment to determine the scope of advocacy services to assist the client in exercising his/her options
Decision Tree for Obtaining Consent Under the Health care Consent Act, 1996
College of Nurses of Ontario (2022). Confidentiality and Privacy-Personal Health Information.
Personal Health Information Act, 2004
- Governs health care information privacy in Ontario
- Information is collected, used and disclosed. PHIPA sets consistent rules for the management of personal health information and outlines the client's rights regarding his/her personal health information
- This legislation balances a client's right to privacy with the need of individuals and organizations providing health care to access and share health information
- PHIPA permits the sharing of personal health information among health care team members to facilitate efficient and effective care
- PHIPA applies primarily to personal health information in the hands of health information custodians
Information Privacy
- The client's right to control how his/her personal health information is collected, used and disclosed
Quality of Care Information Protection Act, 2016
- Provides broad protection to quality of care information produced by a health care facility or a health care entity, or for a governing or regulatory body
- To promote open discussion of adverse events, peer review activities and quality of care information, while protecting this information from being used in litigation or accessed by clients
Personal Health Information
- Any identifying information about clients that is in verbal, written or electronic form
- This includes information collected by nurses during the course of therapeutic nurse-client relationships
- Clients do not have to be named for information to be considered personal health information
- Information is "identifying" if a person can be recognized, or when it can be combined with other information to identify a person
- The legislation recognizes that personal health information belongs to clients and is simply being housed in health care facilities
- Clients have the right to give, refuse or withdraw their consent to the collection, use and disclosure of their personal health information
- Clients also have the right to correct their personal health information
- This means clients can request changes if they believe the record is inaccurate or incomplete (only those in writing can be corrected under the Act)
Examples of Personal Health Information
- A personnel record containing a note from a physician or an NP supporting an absence from work is not considered personal health information
- However, a description of the employee's symptoms and treatment noted by an occupational health nurse (OHN) when providing care is considered personal health information
- If the OHN's records contain health and non-health information, then it is a "mixed record"
Lockbox Provision
- Clients also have the right to instruct that a part of their personal health information not be shared with other providers
- If a client instructs a nurse not to release a part of his/her health information to another practitioner, the nurse must advise the practitioner that some relevant information has been withheld at the direction of the client
Custodian vs. Agent
- Nurses who are employees or volunteers, or contracted or credentialed by health care organizations (ex. clinics, laboratories, CCACs, hospitals and long-term care facilities), are considered "agents" of a custodian
- The legislation defines agents as people authorized to act for, or on behalf of, a custodian
- An agent cannot act on her/his own behalf with regard to personal health information
Custodians are responsible for practices and policies that ensure the confidentiality and security of personal health information, and complying with and informing the Act and PHIPA
Compliance Under the Act
- Designating a contact person to facilitate compliance with the Act and to respond to requests, inquiries and complaints from the public
- Providing a written public statement generally describing information practices, how to reach the contact person, the process for accessing records or requesting corrections, and the complaint process for client
- Ensuring information practices comply with the Act and its regulations
- Ensuring information is accurate, complete and up-to-date
- Ensuring information is secure
Collection
- Nurses may only collect as much personal health information as is needed to meet the purpose of the collection
- Information may be collected indirectly without consent (ex. from a relative or significant other) when the client cannot provide it (ex. he/she is unconscious), if there is a question as to the accuracy of the information that the client provides, or when obtaining consent would affect the timeliness of the care
Personal Health Information Protection Act & Nurses
- The legislation does not change nurses' responsibilities to protect their clients' confidentiality and privacy
- Nor does it greatly affect their ability to collect and use personal health information to plan and deliver care
- Consent to use information to provide care can be assumed by the health care team
- Patient should be aware of his/her right to withhold or withdraw consent to the sharing of his/her personal health information with other members of the health care team
Implied Consent
- It is a custodian's obligation to fulfil conditions by posting a notice or providing a brochure that describes the purposes for the collection, use and disclosure of personal health information
- This kind of notice is one way to fulfil the conditions for implied consent
Express Consent
- PHIPA does not require a specific form of express consent, which may be given verbally or in written form
- It may be provided over the telephone or electronically if the nurse is sufficiently able to identify the person; however, express consent that is written helps avoid ambiguity
Needed when:
- Personal health information is to be disclosed outside of the health care team (ex. submitting personal health information on a claim form to an insurance company)
- Information is to be disclosed (within the health care team) for purposes other than providing, or helping to provide, care
- Personal health information is used for fundraising (ex. contact information can be provided without express consent)
- Personal information is being collected for marketing research or marketing activities
Substitute Decision-Makers
- If a client cannot provide consent, then a substitute decision-maker may make decisions and provide health information
- May be a spouse or the parent of a child under 16 who is unable to answer health questions or make decisions about treatment
Refusing Access to Personal Health Information
Possible grounds for refusing access include the following:
- The information is Quality Assurance information or that generated for a regulatory college’s Quality Assurance Program
- It is raw data from standardized psychological tests or assessments
- It may present a risk of serious harm to the treatment or recovery of the client, or of serious bodily harm to another person
- Access to the information would reveal the identity of a confidential source of information
Client requests to correct personal health information may be refused in the following circumstances:
- The request is frivolous, vexatious or made in bad faith
- The custodian did not create the record and does not have sufficient knowledge, expertise or authority to make the correction
- The information is a professional opinion or observation made in good faith
*Clients can complain to an organization’s contact person or to the Information and Privacy Commissioner about refusals to access requests or other breaches of PHIPA
Disclosure
- Making information available or releasing it to another custodian or person
- Express consent is needed when personal health information is disclosed outside of the health care team or is not used to provide health care
PHIPA includes provisions that permit a custodian to use personal health information without the consent of the client, some of these include:
- To manage risk
- To support quality of care programs
- To allocate resources
- To obtain payment
- To do research, if a research plan has been approved by a research ethics board
The Act also permits practitioners to disclose personal health information without obtaining consent in the following circumstances:
- If disclosure is needed to provide health care, and consent cannot be obtained quickly
- To contact a relative or friend of an injured, incapacitated or ill client for consent
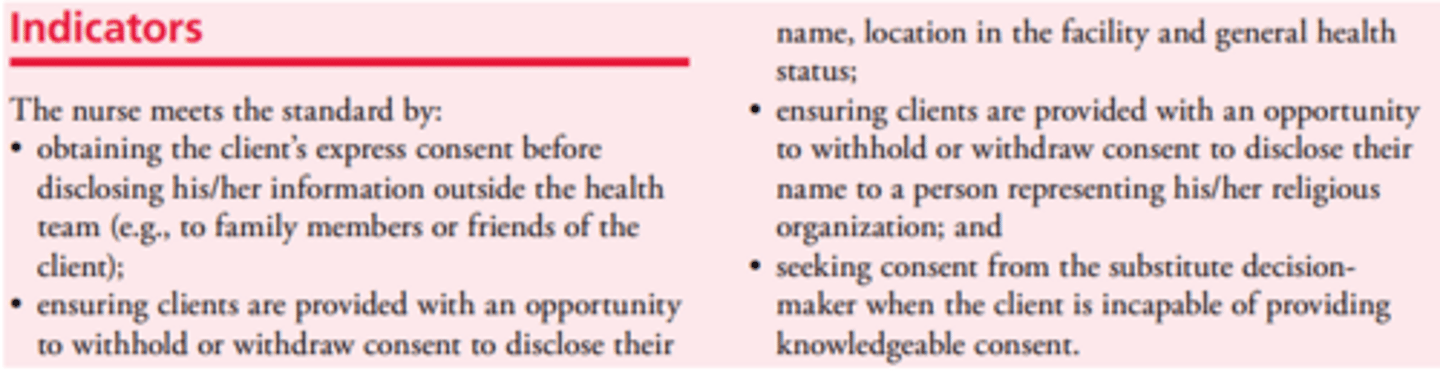
- To confirm that a client is a resident or client in a facility, provide his/her location and comment on his/her general health status (unless there is an express request not to do so)
- To eliminate or reduce a significant risk of harm to a person
Professional Misconduct
- Giving information about a client to a person other than the client or his or her authorized representative, except with the consent of the client or his or her representative, or as required or allowed by law
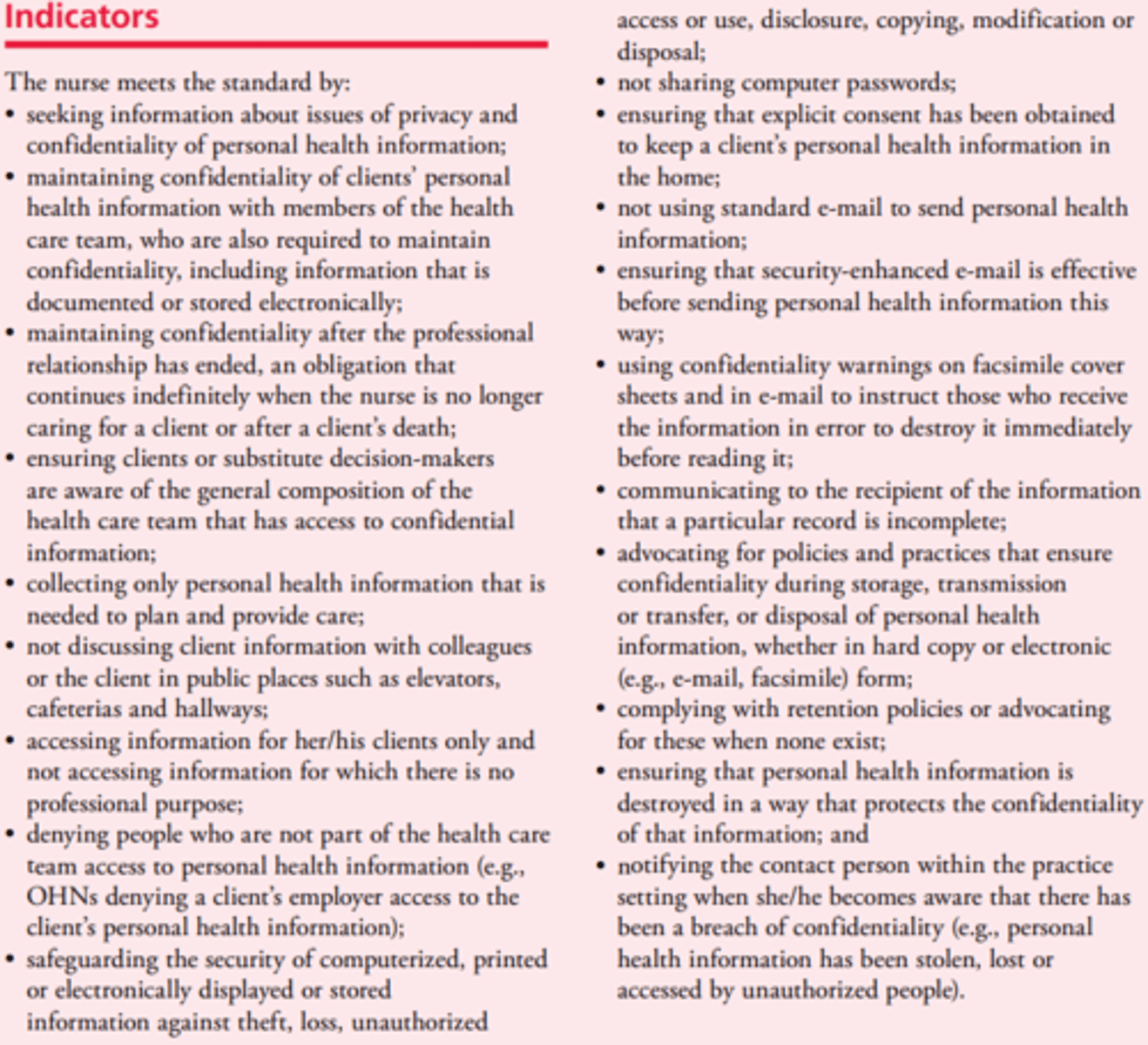
Personal Health Information Practices:
- Nurses share relevant information with the health care team, whose members are obliged to maintain confidentiality
- Nurses must explain to clients that information will be shared with the health care team and identify the general composition of the health care team
Knowledgeable Consent & Substitute Decision-Makers
- Nurses ensure that clients are aware of their rights concerning their personal health information and have expressly consented to the collection, use and disclosure of information outside the health care team
The Client's Right to Access & Amend His/Her Personal Health Information
- Nurses respect the client's right to see/obtain a copy of his/her health information, to see his/her health file and to request correction to the information
- The onus is on the client to prove that the record is incomplete or inaccurate, and any changes to the record must be tracked

Potential for Harm
- When a nurse learns information that, if not revealed, could result in harm to the client or others, she/he must consult with the health care team and, if appropriate, report the information to the person or group affected
Disclosure Without Consent
- Disclosure without consent Nurses adhere to legislation that requires them to reveal confidential information to others
- Ex. The Child, Youth and Family Services Act, 2017, requires all health care professionals to report suspected child abuse to the Children’s Aid Society; the Health Protection and Promotion Act permits reporting of certain conditions to the Medical Officer of Health
- Additionally, required reporting information may be disclosed to the Workplace Safety and Insurance Board
- The information CNO gathers during an investigation and shares with the members under investigation is confidential
Care Delivery Processes
- These processes support the delivery of nursing care and services related to confidentiality and privacy of personal health information
Strategies:
- Conducting reviews of health information practices with staff to ensure that privacy and confidentiality standards are being met
- Developing and implementing supportive policies and processes that address privacy, confidentiality and security in the collection, use and disclosure of personal health information
Policies/Processes:
- Giving the client access to his/her health information
- Managing client and/or family requests for changes to the health record
- Defining the nurse’s role in dealing with a client’s right to access his/her health record
Communication Systems
- Support information sharing and decision-making about client care and services
- Systems should promote sharing of health information among interprofessional team members while protecting the privacy, confidentiality and access rights of clients
Strategies:
- Ensuring that the electronic systems that support the transmission of client information (ex. facsimiles, e-mail, intranet) are secure and protect client confidentiality
- Ensuring that written public notice with details on how to access and correct personal health information is available, and gives the name of the contact person who can respond to inquiries and receive complaints
- Establishing a process to help staff deal with issues/conflicts arising from inconsistent practices relating to privacy and confidentiality of personal health information
- Consulting with front-line nurses, to tap into their expertise and experience, when determining the functional requirements to maintain confidentiality in computerized documentation systems
Leadership
- Leadership is the process of supporting others to improve client care and services by promoting professional practice
Strategies:
- Developing and implementing leadership opportunities, such as involving nursing staff in the development of privacy and confidentiality policies/procedures development and revisions related to the health record
- Establishing systems that ensure health information is collected, used, disclosed and accessed according to PHIPA and QOCIPA
- Designating someone in the organization to act as the main contact for nurses with questions about confidentiality and security of personal health information
Professional Developmental Systems
- Promotes a learning environment
- Activities include orientation, education, performance management and professional practice activities related to privacy and confidentiality
Strategies:
- Ensuring orientation to the facility includes addressing matters of privacy, confidentiality, security of personal health information and relevant policies and procedures
- Providing educational opportunities to support effective compliance with PHIPA and QOCIPA legislation
Cristal, N., Kohja, Z., Gawaziuk, J.P., Spiwak, R., & Logsetty. S. (2021). Narrative discourse of burn injury and recovery on peer support websites: A qualitative analysis. Burns, 47(2), 397-401.
Burn Survivor's Lived Experiences
- Burn survivors are now turning to social media and shared web-based peer support resources during recovery and continuing long after discharge
- Ongoing peer support is often part of the reclamation process after-burn injury
- Peer support and event sharing helps foster hope, motivation and reassurance
Emergent Care for Skin Burn Injuries
- In the acute phase, extreme pain and the need for immediate medical attention is a common experience
- Psychological trauma, multiple operations operation and permanent scarring and possible physical disfigurement occurs with full thickness burns
Peer Support for Skin Burn Injuries
- Helps foster hope, motivation and reassurance
- As with other patient groups, burn survivors are turning to websites to source information related to illness adaptation and recovery
- Cloud-based groups allow the writer to share information to an extent they are comfortable with, while creating their own narrative of what happened
Common Themes for Skin Burn Injury Patients
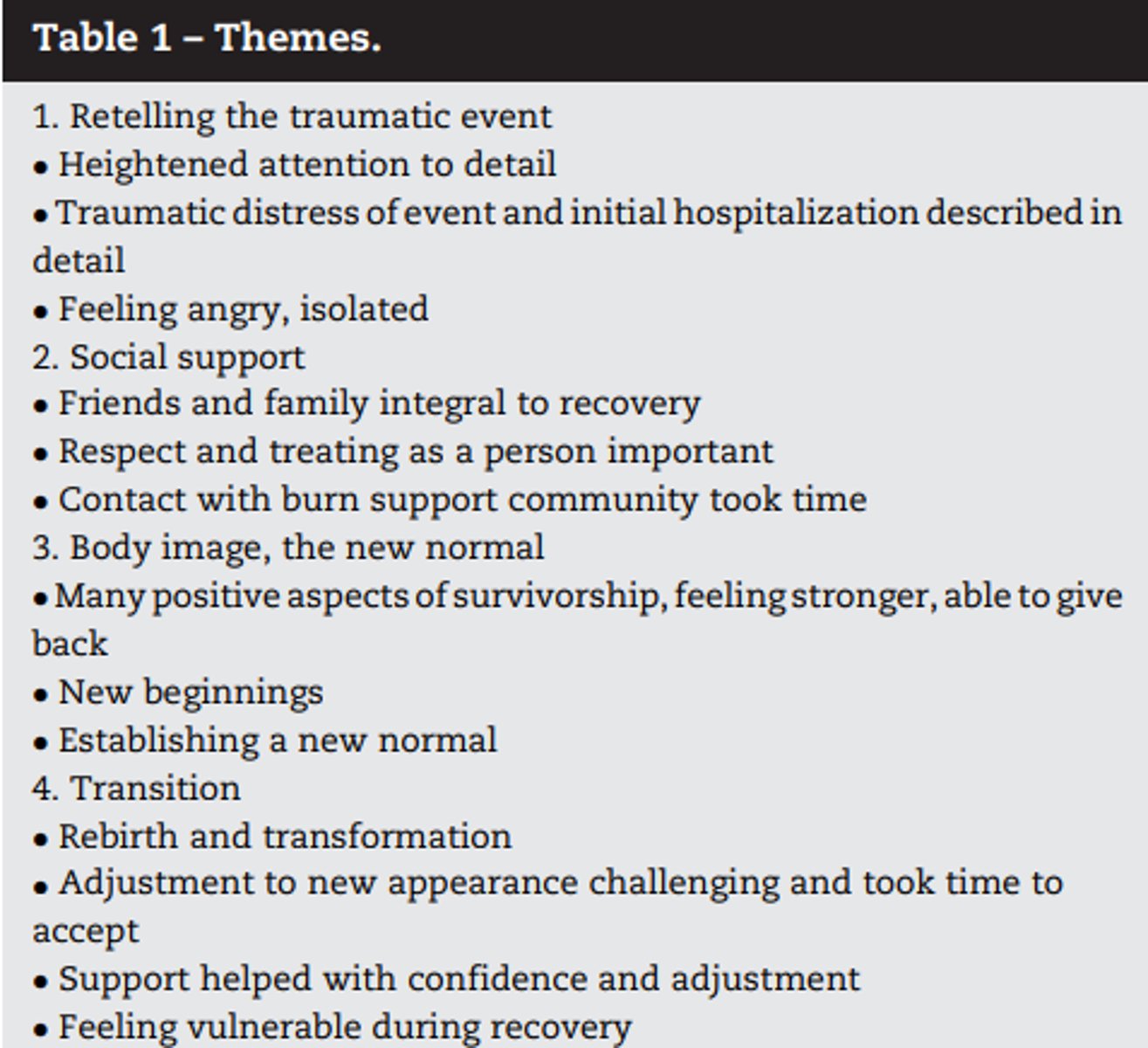
Retelling the Traumatic Event
- To accentuate the traumatic nature of the event, subjects provided immense detail and deconstruction
- The language was often passionate with an emphasis on the magnitude of the experience such as being 'engulfed in a fireball', or 'walking through a wall of fire'
- There was also extensive detail about the initial hospitalization with magnified detail about life supports, 'fighting for each breath' and hospital care making the difference between life and death
- The early care was described with an emphasis on the critical nature of the situation with so many 'tubes'
- During the accident and acute phase, events were described as moving in slow motion
- The passage of time was slowed down, with the early days feeling 'like watching a clock'
- Subjects also commented on feeling angry, emotionally wounded, and feeling overwhelmed with guilt and unable to speak about whathappened andfocus onthought
- There was a description of feeling emotionally overwhelmed with thoughts of extreme loss, anger, depression, isolation and in very low moments, wanting to die
Social Support
- This included both positive and negative explanations and the role of others in the burn story
- Most narrators described in detail the value of supportive family members, friends, caregivers and the wider community in the recovery process
- The family often provided a gateway to others in explaining what had happened and maintaining pre-burn relationships
- Frequent contact was immensely appreciated
- The appreciation and encouragement from visitors and the impact of unanticipated kindness from strangers
- Enjoyed using social media to still be connected to the outside world
- The absence of positive comments was related to more challenging recoveries
- There were also a few comments about feeling bullied and bothered for looking different (causing withdrawal and isolation)
- The value of visitation and contact from other burn survivors was described something that was appreciated gradually over time, and with the value not obvious during the initial hospitalization
- Attending burn community events and websites was also described as valuable and humbling
- Peer support social media venues provide an outlet for burn survivors to express their emotions and network with individuals enduring a similar struggle
*Need structured peer support by trained individuals
Body Image & the New Normal
- Early perceptions of appearance, expressions related to self-image, adjusting to changed and self-confidence related to changes
- Altered skin texture and appearance was what one narrator described as 'the new normal'
- The integration after burn benefit benefited from a reintroduction to children and others explaining that they were the same person
- also descriptions of looking weak and so thin after the hospitalization, being self-conscious and vulnerable
- There were also descriptions of feelings depersonalized, as being stereotyped as a burn survivor only or a patient, and not the person they are
- Facing the public and new intimate relationships were described as particularly challenging events
- The initial view of oneself was very traumatic
- Biographers noted that with encouragement they were able to go out more, not cover up scars and feel more confident about the changes in appearance
- The support and encouragement of family members was vital in accepting appearance changes and a new body image
Rebirth & Transformation
- Changes as a result of the injury, redefining oneself and finding a new path or life course
- The burn accident marked the beginning of a different life course
- There was a description of 'rising from the ashes' and becoming a new person with inner strength and resilience
- Biographers described themselves as becoming less self-centered, more compassionate, more confident and finding happiness in helping others
- The story arc was most often one of resiliency and a positive transformation
- Many acknowledged that they were stronger after the trauma
- The rebirth included lessons learned and for others going through the same experience (such as maintaining a sense of humor, to not grieve for what was lost and to be kind to oneself)
Gushue, K. & Bidigare, C. (2023). Nursing Management: Burns. In J. Tyerman, S. Cobbett, M.M. Harding, J. Kwong, D. Roberts, D. Hagler, & C. Reinisch. (Eds.). Medical-surgical nursing in Canada: Assessment and management of clinical problems (5th. Canadian ed.), pp. 518-541. Elsevier Canada.
Burn
- An injury to the tissues of the body caused by heat, chemicals, electric current, or radiation
- The resulting effects are influenced by the temperature of the burning agent, the duration of contact time, and the type of tissue that is injured
- Although burn incidence has decreased over the past 20 years, burn injuries still occur too frequently, mainly to persons living at lower socioeconomic levels and with histories of substance misuse or mental illness
- Most burn incidents are preventable
- Coordinated national programs in developed countries have focused on use of child-resistant lighters, nonflammable children's clothing, tap water anti-scald devices, stricter building codes, hard-wired smoke detectors and alarms, and fire sprinklers
Common Locations & Sources of Burn Injury
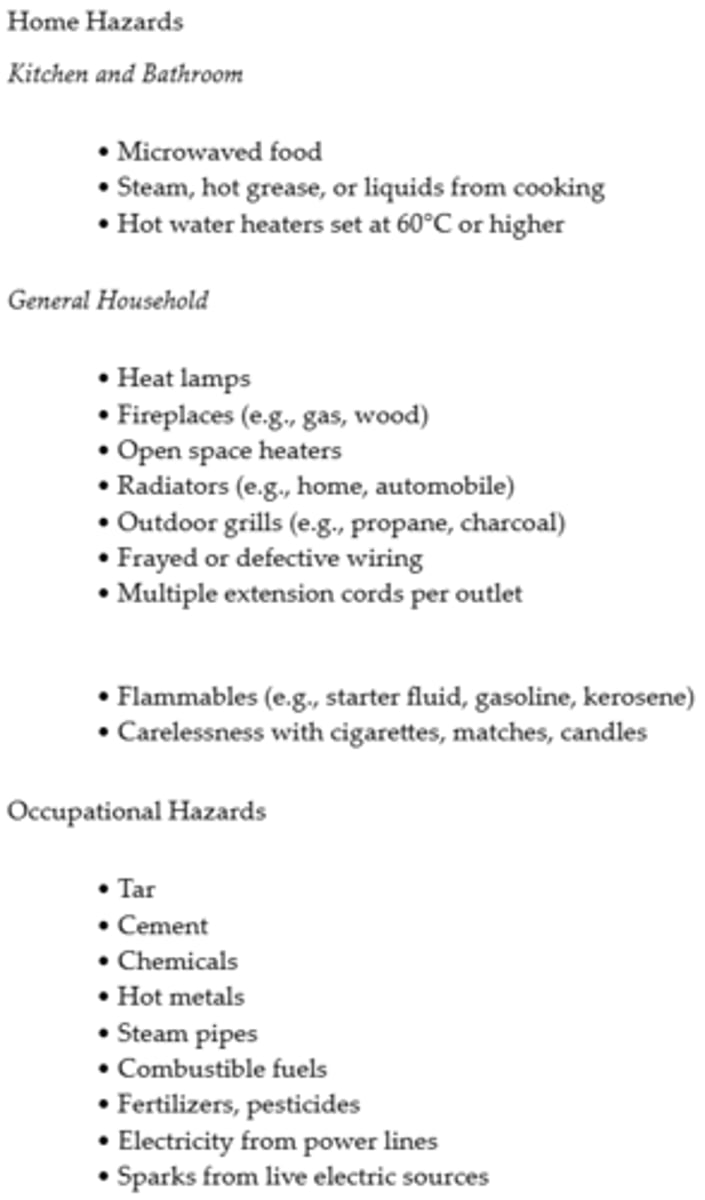
Thermal Burns
- Caused by flame, flash fire, scald, or contact with hot objects
- They are the most common type of burn injury
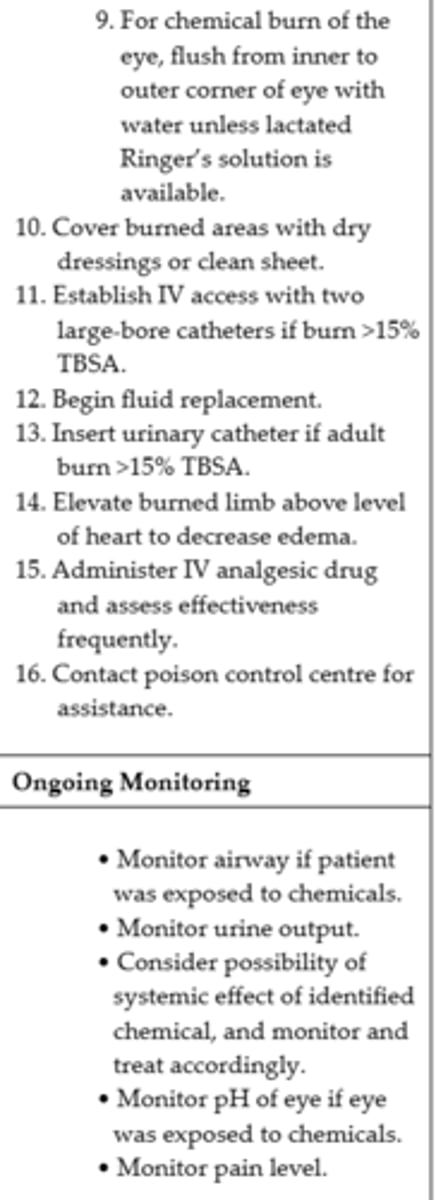
Chemical Burn
- The result of contact with acids and alkalis
- Acids can be found in the home and at work—in car batteries, bleach, chemical laboratories, vinegar, and glass polish
- The chemical compounds include hydrochloric, sulphuric, acidic, and hydrofluoric acid
- Alkali substances are found in cement, drain cleaners, cleaning agents, and fertilizer and include calcium hydroxide (lime), ammonia, or ammonia hydroxide
Smoke Inhalation Injuries
- From breathing noxious chemicals or hot air can cause damage to the tissues of the respiratory tract
= The vocal cords and glottis close as a protective mechanism, so damage to the respiratory mucosa occurs less often
- Smoke inhalation injuries are a major predictor of mortality in burn patients
- Prompt assessment for signs and symptoms of airway compromise is imperative because severe edema, bronchospasm, or a mucous plug can occur within minutes to days after the initial exposure
- 3 types: Carbon monoxide poisoning, inhalation injury above the glottis, inhalation injury below the glottis
Types of Burn Injuries #1
Types of Burn Injuries #2
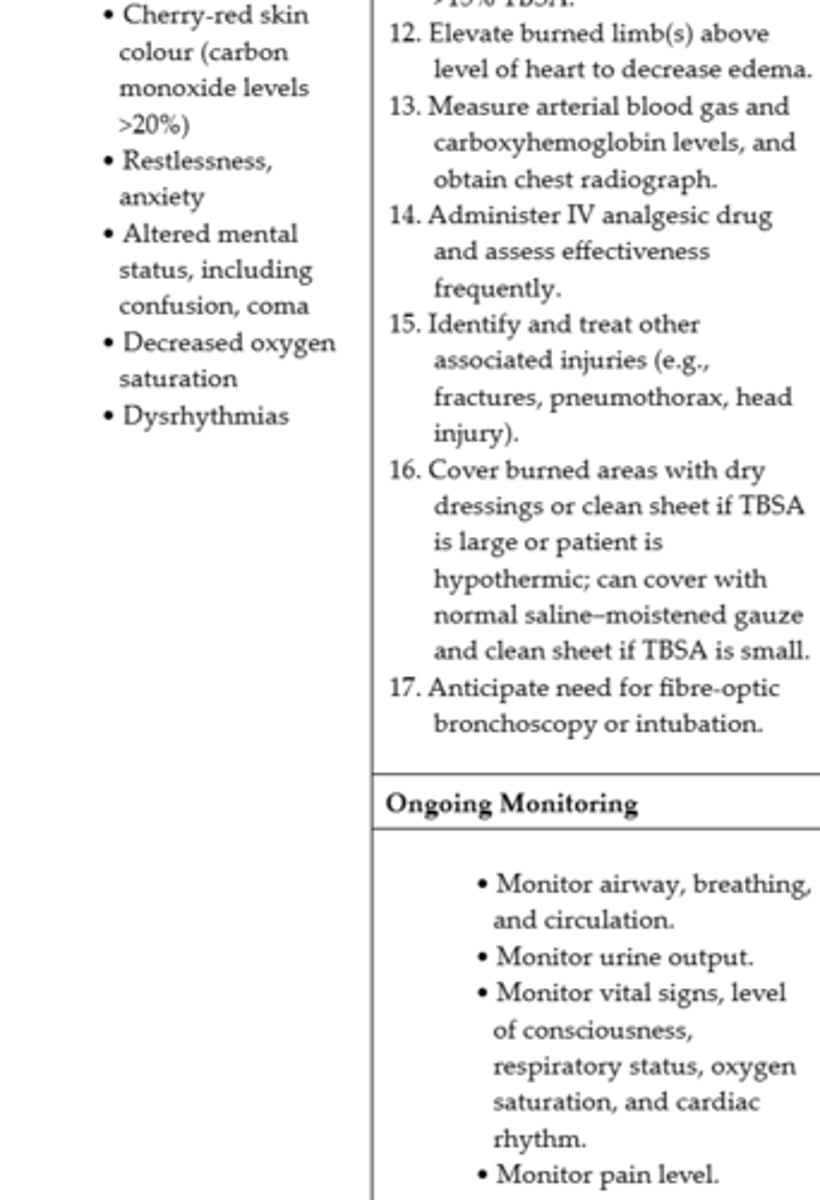
Carbon Monoxide Poisoning
- Carbon monoxide poisoning and asphyxiation account for the majority of deaths at a fire scene
- Carbon monoxide is produced by the incomplete combustion of burning materials
- It is subsequently inhaled and displaces oxygen (O2) on the hemoglobin molecule, causing carboxyhemoglobinemia, hypoxia, and, when the carbon monoxide levels exceed 20%, death
- With severe carbon monoxide poisoning, skin colour is often described as "cherry red" in appearance
- Carbon monoxide poisoning may occur in the absence of burn injury to the skin (ex. smoke inhalation during a fire)
- Carbon monoxide poisoning is treated by administering 100% oxygen until carboxyhemoglobin levels return to normal
- The use of hyperbaric oxygen therapy to treat carbon monoxide poisoning is contraindicated in the presence of a body burn as it delays important burn care
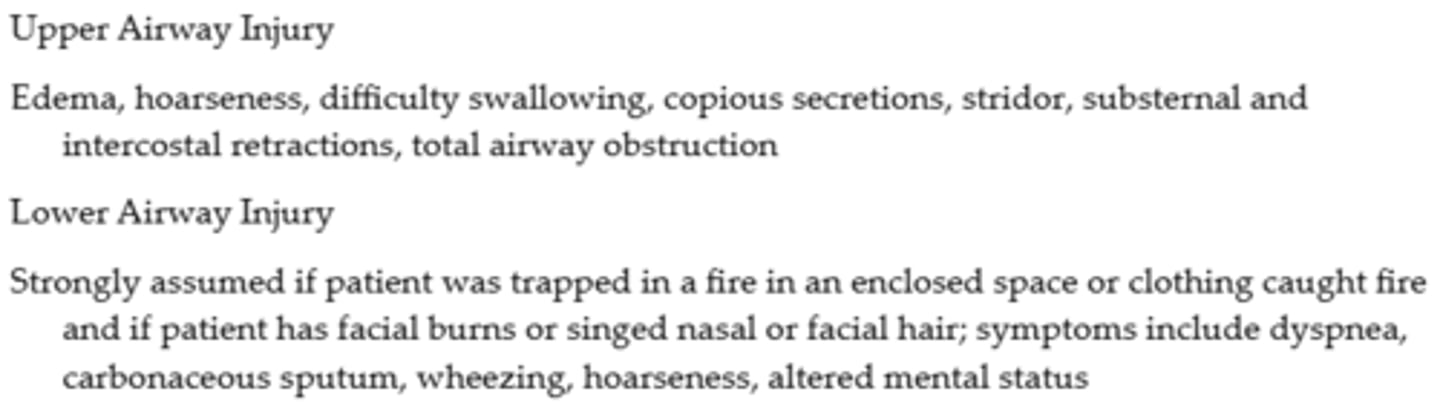
Inhalation Injury Above the Glottis
- In general, an inhalation injury above the glottis (upper airway injury) is thermally produced and may be caused by the inhalation of hot air, steam, or smoke
- Mucosal burns of the oropharynx and larynx are manifested by redness, blistering, and edema
- Mechanical obstruction can occur quickly, which represents a true medical emergency
- Clues to the occurrence of this injury include the presence of facial burns, singed nasal hair, hoarseness, painful swallowing, darkened oral and nasal membranes, carbonaceous sputum, history of being burned in an enclosed space, and clothing burns around the chest and neck
Inhalation Injury Below the Glottis
- An inhalation injury below the glottis (lower airway injury) is usually chemically produced
- Tissue damage is related to the duration of exposure to smoke or toxic fumes
- Clinical manifestations such as pulmonary edema may not appear until 12 to 24 hours after the burn, and then they may manifest as acute respiratory distress syndrome
Manifestations of Respiratory Injury Associated with Burns
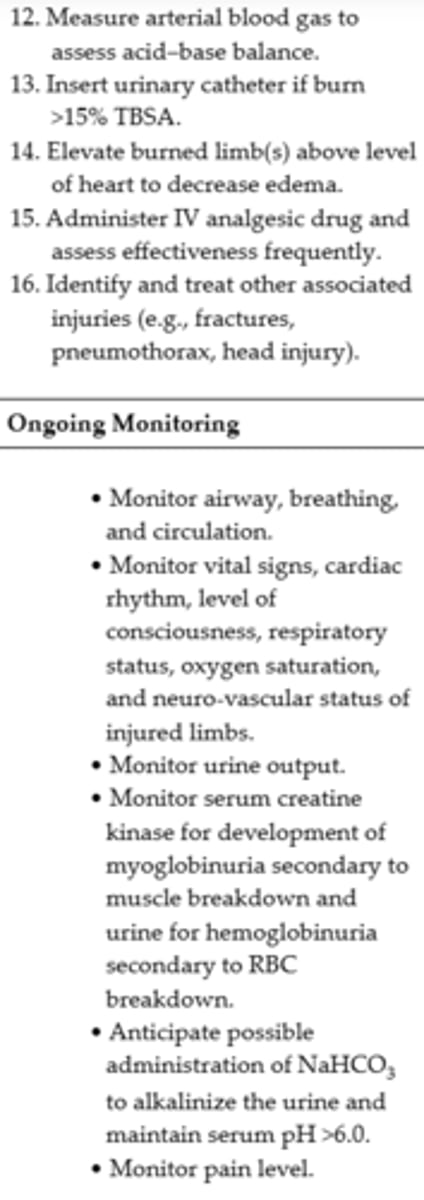
Electrical Burns
- Result from intense heat generated from an electric current and are considered the most severe type of thermal trauma, generally associated with greater damage of functional structures, such as muscle and bone
- The severity of the electrical injury depends on the amount of voltage, tissue resistance, current pathways, surface area in contact with the current, and length of time that the current flow was sustained
- Tissue density affects the amount of resistance to electric current
- Current that passes through vital organs (e.g., brain, heart, kidneys) produces more life-threatening sequelae than that which passes through other tissue
- As with inhalation injury, a rapid assessment of the patient with an electrical injury should be performed
- Contact with electric current can cause muscle contractions strong enough to fracture the long bones and vertebrae
- For this reason, all patients with electrical burns should be considered at risk for a cervical spine injury
- Cardiac arrhythmias are the most common complication from electric shock and can be sudden or delayed (delayed arrythmias can occur without warning during the first 24 hours after injury)
- Direct nerve damage can result and manifest as a peripheral nerve injury, spinal cord damage, cerebellar ataxia, hypoxic encephalopathy, or intracerebral hemorrhage
- Myoglobin from injured muscle and hemoglobin from damaged red blood cells (RBCs) are released into the circulation whenever massive muscle and blood vessel damage occurs
Iceberg Effect
- The severity of an electrical injury can be difficult to determine since most of the damage is below the skin
Classification of Burn Injury
- Severity is determined by (a) depth of burn, (b) extent of burn calculated in percentage of total body surface area (TBSA), (c) location of burn, and (d) patient risk factors (e.g., age, past medical history)
- Goals of care include wound healing, prevention of infection, pain management, prevention of complications, and return to preinjury function
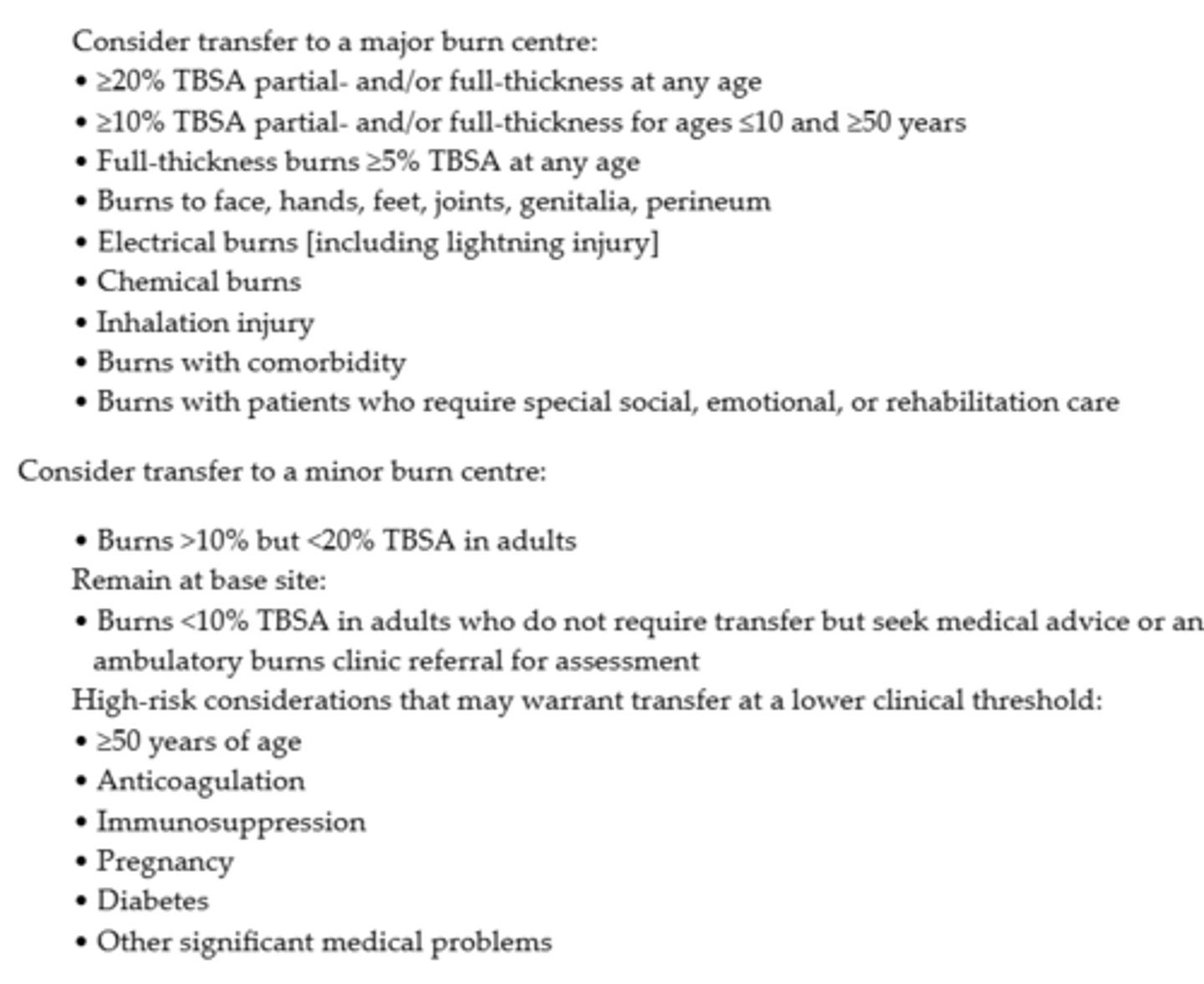
Criteria for Transfer of the Patient with Burn Injuries
Depth of Burn
- Burns continue to be defined by degrees: first-, second-, third-, and fourth-degree
- The ABA recommends a more precise definition, classifying them according to depth of skin destruction: partial-thickness burn and full-thickness burn
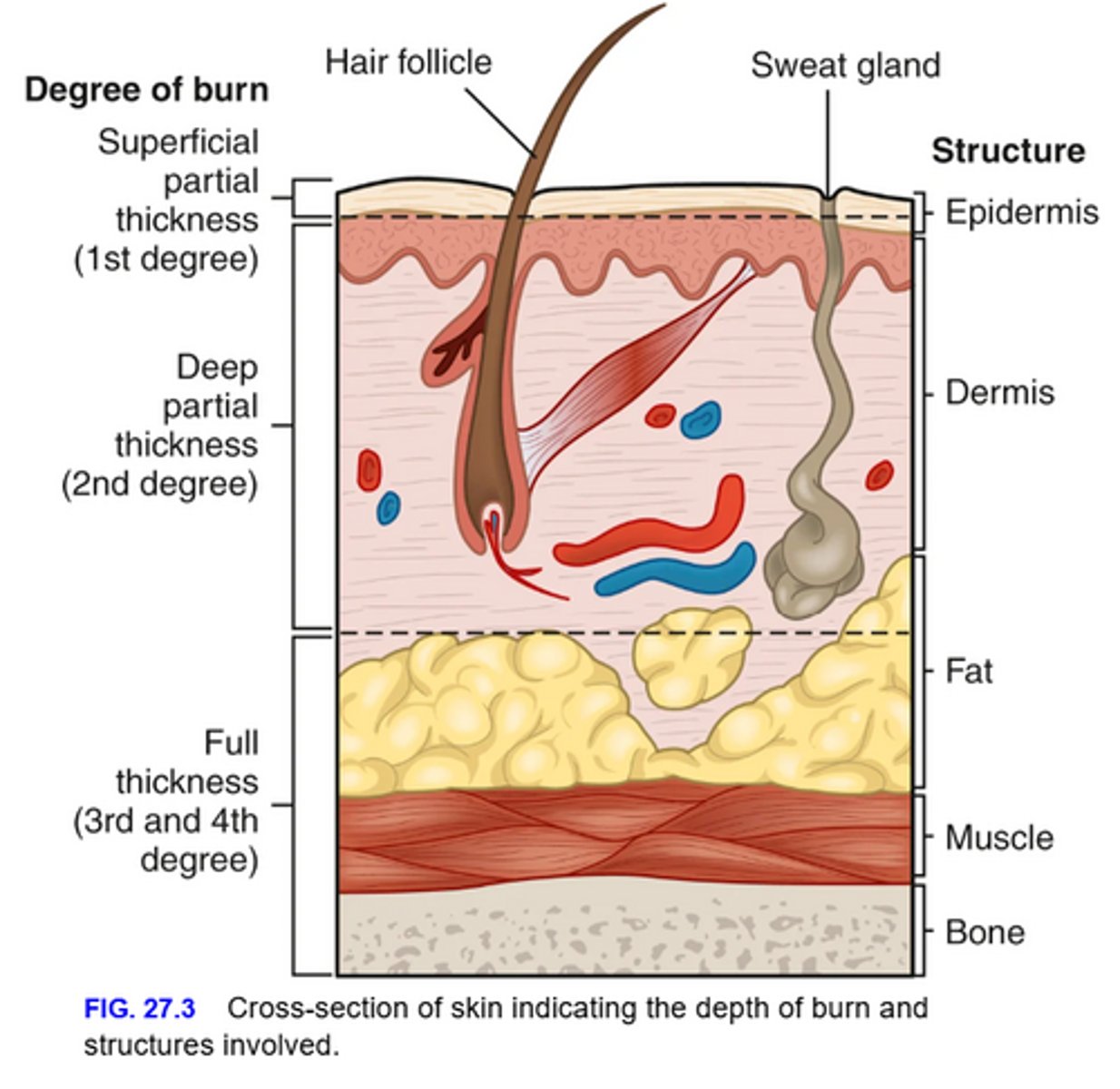
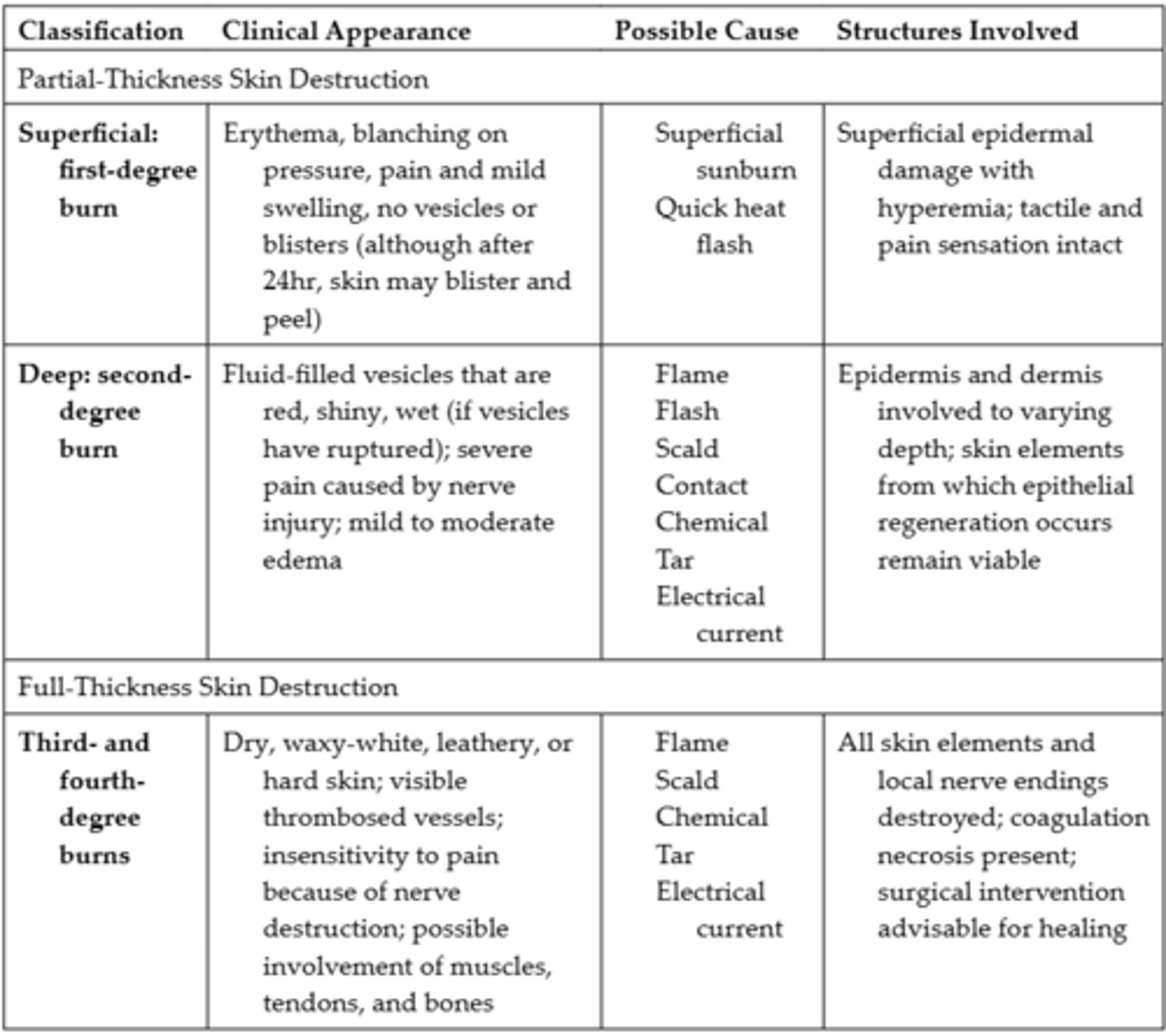
Partial Thickness Burns
- Have varying degrees of epidermal and dermal skin injury, with some skin elements remaining viable for regeneration
Full Thickness Burns
- Involve the destruction of all skin elements and subcutaneous tissues, with the possible involvement of muscles, tendons, and bones
- If there is significant damage to the dermis (ex. a full-thickness burn), not enough skin cells remain to regenerate new skin
Extent of Burn
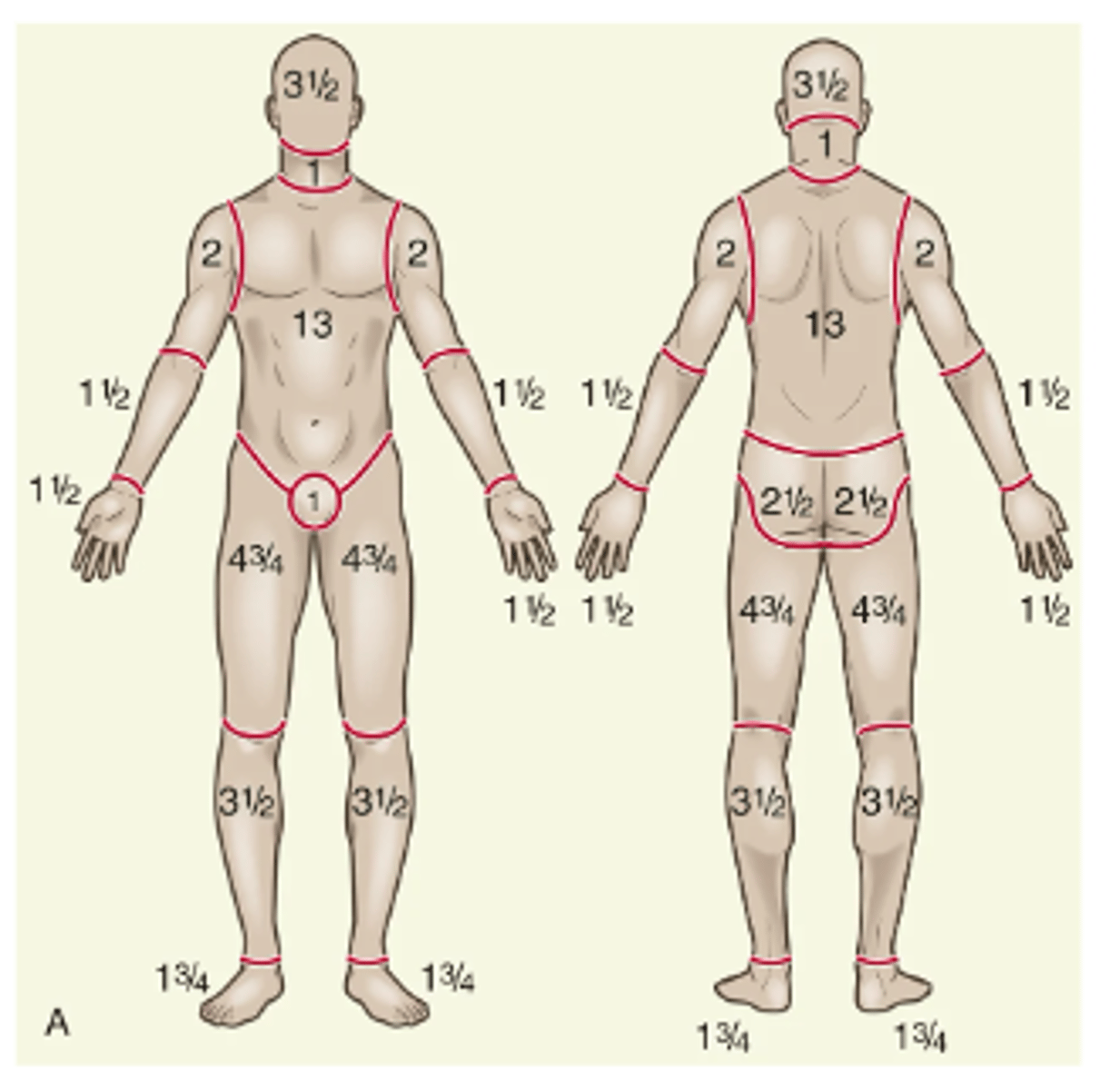
- Two commonly used guides for determining the TBSA affected or the extent of a burn wound are the adult Lund-Browder chart and the adult rule of nines chart
Lund-Browder Chart
- Considered more accurate because the patient's age, in proportion to relative body-area size, is taken into account
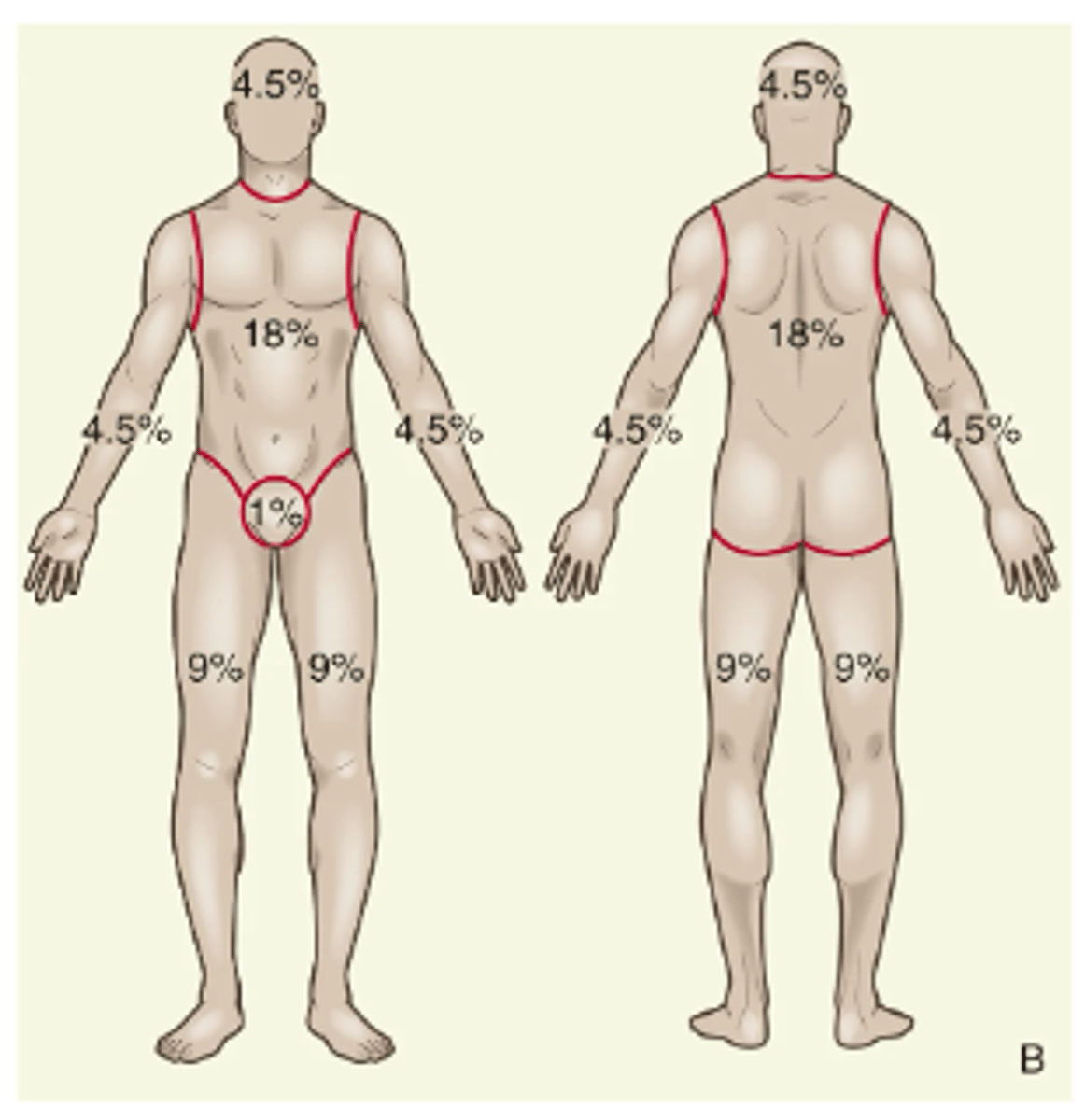
Rule of 9's
- Easy to remember, is considered adequate for initial assessment of an adult patient with burn injury
- For irregular or odd-shaped burns, the size of the patient's hand (including the fingers) is approximately 1% TBSA
Sage Burn Diagram
- A free, Internet-based tool available for estimating TBSA burned
Location of Burn
- Burns to the face and neck and circumferential burns to the trunk or back can result in mechanical obstruction, secondary to edema, and leathery, devitalized tissue formation (eschar), both of which may inhibit respiratory function
- These injuries may also include possible inhalation injury and respiratory mucosal damage
- Burns to the hands, feet, joints, and eyes are of concern because they make self-care very difficult and may jeopardize future function
- Burns to the hands and feet are challenging to manage because of superficial vascular and nerve supply systems that must be protected and because of the need to maintain hand function during healing
- Burns to the ears and nose are susceptible to infection because the skin is very thin and the underlying skeleton frequently exposed
- Burns to the buttocks or perineum are at high risk for infection from urine or feces contamination
- Circumferential burns to the extremities can cause circulatory compromise distal to the burn and, subsequently, neurological impairment of the affected extremity
Classification of Burn Injury Depth
Patient Risk Factors
- The older person heals more slowly and usually experiences more difficulty with rehabilitation than a younger adult
- Any patient with pre-existing cardiovascular, respiratory, or renal disease has a poorer prognosis for recovery because of the tremendous demands placed on the body by a burn injury
- The patient with diabetes mellitus or peripheral vascular disease is at high risk for poor healing
- The patient with a burn injury who has concurrently sustained other injuries, fractures, head injuries, or other trauma, has a poorer prognosis for recovery
Phases of Burn Management
- Burn management has been organized chronologically into three phases that correspond to the key priority of each particular phase: emergent (resuscitative), acute (wound healing), and rehabilitative (restorative)
- Planning for rehabilitation begins on the day of the burn injury or admission to the burn unit
- Formal rehabilitation begins as soon as functional assessment can be performed
Prehospital Care
- At the injury scene, priority is given to removing the person from the source of the burn and stopping the burning process
- Small thermal burns (<10% of TBSA) should be covered with a clean, cool, tap water-dampened towel for the patient's comfort and protection until definitive medical care is instituted
- Cooling of the injured area (if small) within 1 minute helps minimize the depth of the injury
- If the burn area is large (>10% TBSA) or an electrical or inhalation burn is suspected and the patient is unresponsive, attention needs to be focused first on ABC (airway, breathing, circulation)
- To prevent hypothermia, large burns should be cooled for no more than 10 minutes
- A burn should never be covered with ice because this can cause hypothermia and vasoconstriction of blood vessels, further reducing blood flow to the injury
- As much burned clothing as possible should be gently removed, to prevent further tissue damage
- Adherent clothing should be left in place until the patient is transferred to a hospital
- The patient should be wrapped in a dry, clean sheet or blanket to prevent further contamination of the wound and to provide warmth
- Chemical burns are best treated by quickly removing the solid particles and powder from the skin
- Patients with inhalation injuries should be observed closely for signs of respiratory distress or compromise
- It is important for individuals involved in the prehospital phase of burn care to adequately communicate the circumstances of the injury to hospital-based health care providers

Emergent Phase
- The period of time required to resolve the immediate, life-threatening conditions resulting from the burn injury
- This phase usually lasts up to 72 hours from the time of the burn
- Primary concerns are the onset of hypovolemic shock and formation of edema
- The phase ends when fluid mobilization and diuresis begin
Fluid & Electrolyte Shifts - Emergent Phase
- The greatest initial threat to a patient with a major burn is hypovolemic shock (due to increased capillary permeability)
- As the capillary walls become more permeable, water, sodium, and, later, plasma proteins (especially albumin) move into interstitial spaces and other surrounding tissue
- This results in the shifting of more fluid out of the vascular space into the interstitial spaces (second spacing fluid accumulation; or to third spaces)
- Other sources of fluid loss during this period are insensible losses by evaporation from large, denuded body surfaces and the respiratory system
- The normal insensible loss of 30 to 50 mL per hour is increased in severely burned patients
- Decreased blood pressure (BP), increased heart rate, and other manifestations of hypovolemic shock are clinically detectable signs of intravascular volume depletion
- If it is not corrected, irreversible shock and death may result
- The circulatory status is also impaired because of hemolysis of RBC
- Thrombosis in the capillaries of burned tissue causes an additional loss of circulating RBCs
- Elevation of the hematocrit is commonly caused by hemoconcentration, which results from fluid loss
- Sodium rapidly shifts to the interstitial spaces and remains there until edema formation ceases
- A potassium shift develops initially because injured cells and hemolyzed RBCs release potassium into the circulation
- Toward the end of the emergent phase, capillary membrane permeability is restored if fluid replacement is adequate
Emergency Management Chemical Burns #1
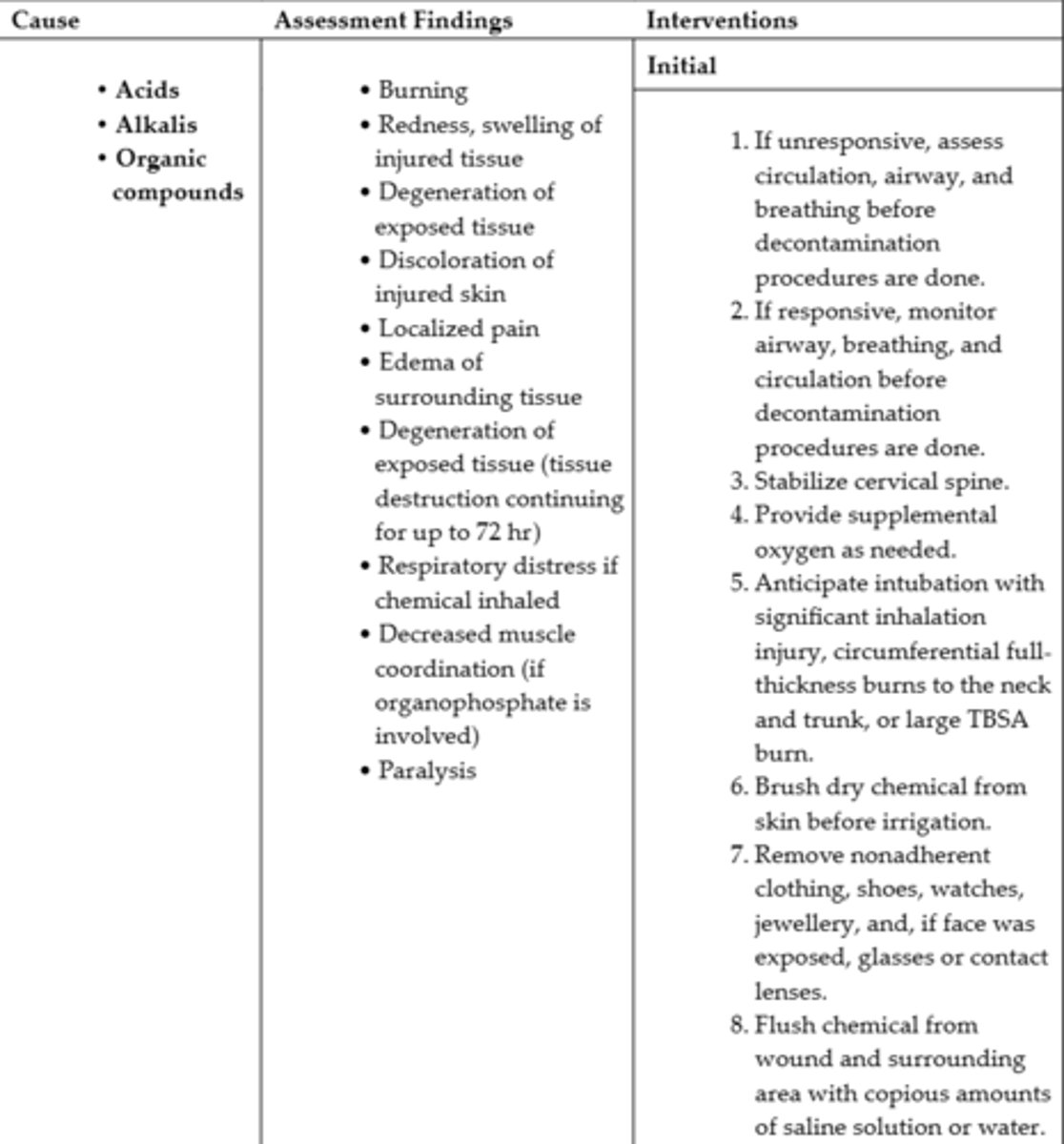
Emergency Management Chemical Burns #2
Emergency Management Inhalation Injury #1
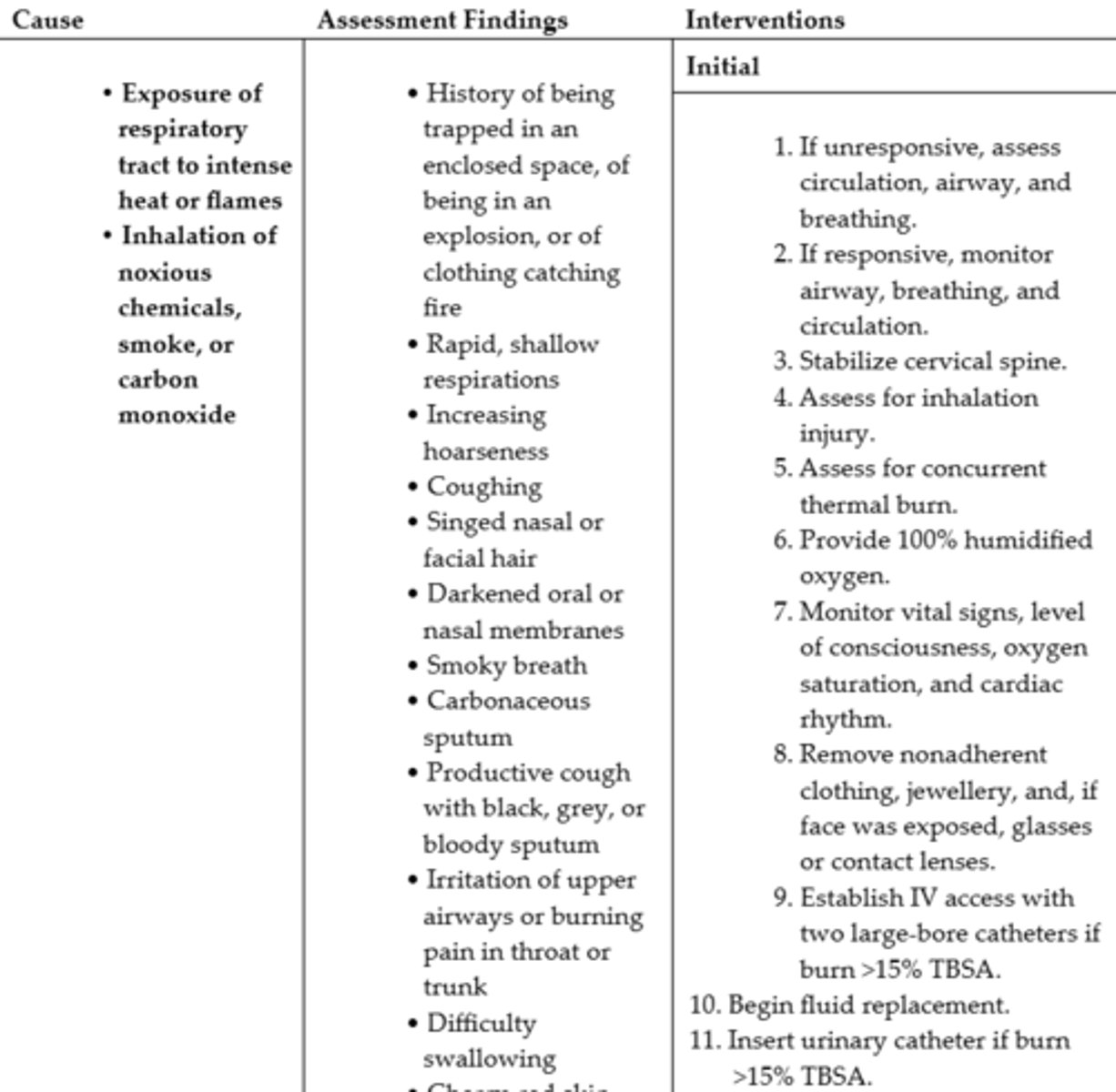
Emergency Management Inhalation Injury #2
Inflammation & Healing - Emergent Phase
- Burn injury causes coagulation necrosis, in which tissues and vessels are damaged or destroyed
- Neutrophils and monocytes accumulate at the site of injury
- Fibroblasts and newly formed collagen fibrils appear and begin wound repair within the first 6 to 12 hours after injury
Immunological Changes - Emergent Phase
- The skin barrier to invading organisms is destroyed, bone marrow depression occurs, and circulating levels of immunoglobulins decrease
- The function of white blood cells (WBCs) becomes defective
- The inflammatory cytokine cascade triggered by tissue damage impairs the function of lymphocytes, monocytes, and neutrophils
- This impaired function increases the patient's risk for infection
Clinical Manifestations - Emergent Phase
- Patients with burns are likely to be in shock from hypovolemia
- Areas of full-thickness and deep partial-thickness burns are initially anaesthetic because nerve endings have been destroyed
- Superficial to moderate partial-thickness burns are painful
- Blisters, filled with fluid and protein, may develop in partial-thickness burns
- Patients with a larger burn area may have signs of adynamic ileus, such as absent or decreased bowel sounds, as a result of the body's response to massive trauma and potassium shifts
- Shivering may occur as a result of chilling caused by heat loss, anxiety, or pain
- Ongoing nursing assessment of the ABCs, vital signs, cardiac rhythm, oxygenation, and level of consciousness are priorities during the emergent phase of burn care
- Most patients with burn injuries are quite alert and can provide answers to questions shortly after the injury or until they are intubated
- They are often frightened and benefit from calm reassurance and simple explanations by all health care providers
Emergency Management Electrical Burns #1
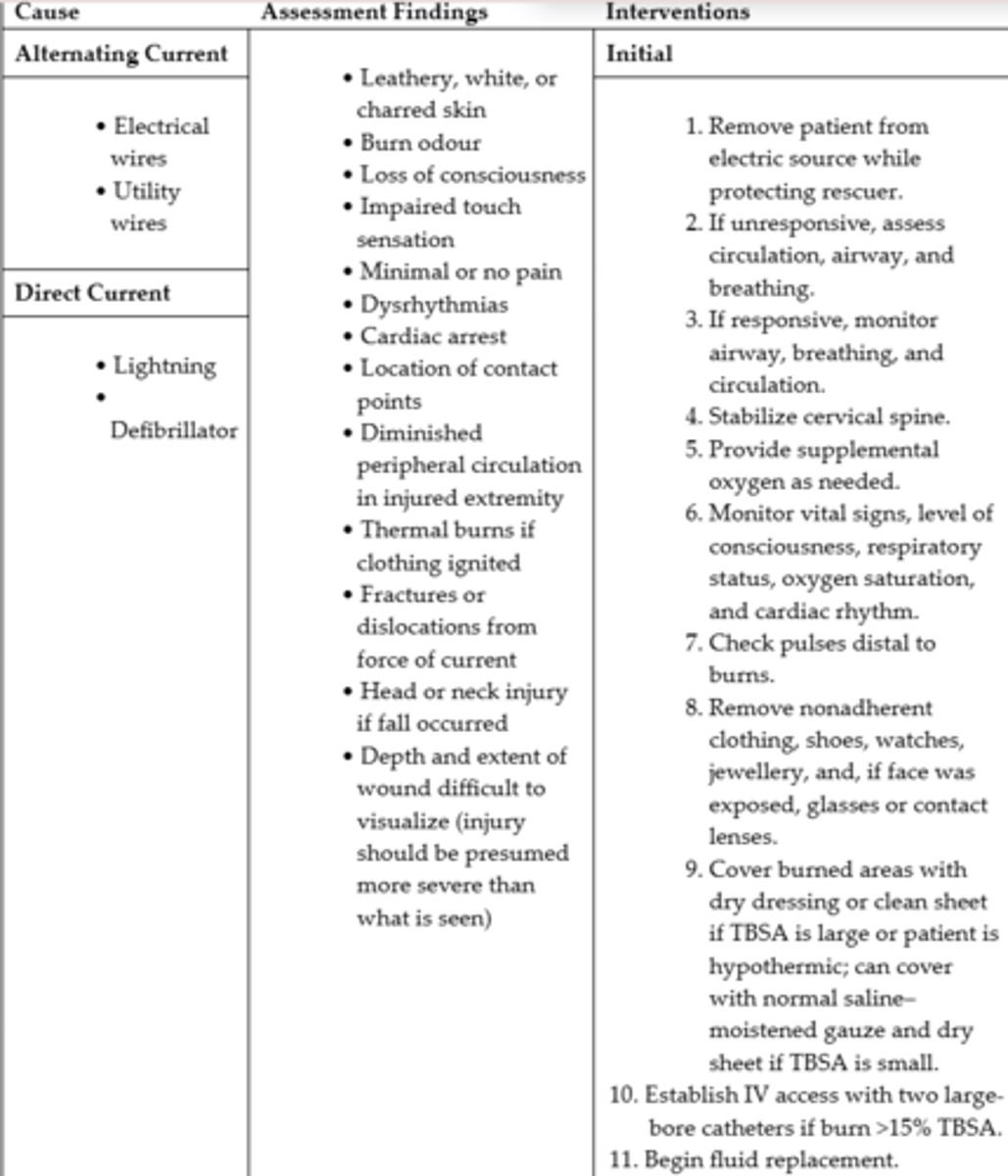
Emergency Management Electrical Burns #2
Cardiovascular System Complications - Emergent Phase
- Cardiovascular system complications include dysrhythmias and hypovolemic shock, which may progress to irreversible shock
- Circulation to the extremities can be severely impaired by deep, circumferential burns and subsequent edema formation (act like tourniquet)
- If they are untreated, ischemia, paresthesias, and necrosis can occur
- To restore circulation to compromised extremities, an escharotomy (a scalpel or electrocautery incision into necrotic tissue) is frequently performed after the patient's transfer to a burn unit