Week 8 CIED Follow-Up - EGM Analysis
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
Tachy EGMs
Stored in device or printed using programmer
Abnormal rhythms: sustained and nonsustained
Determine if the device got it right
Inappropriate therapy inhibition/delivery
May require programming changes
Sensitivity must be 100%
Specificity should be as close to 100% as possible
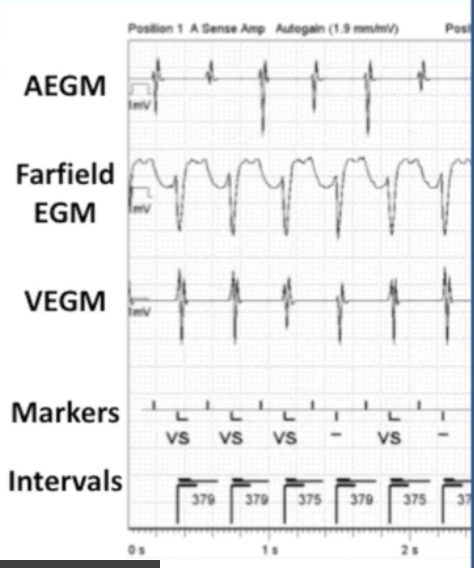
Tachy EGM Analysis: Step 1
Orient yourself to the strip
Channels:
Surface
Nearfield
Farfield
Markers/annotations
Company/device
Tachy EGM Analysis: Step 2
Analyze and classify presenting and underlying (non-paced) rhythm as much as possible
No pacing: normal rhythm analysis
Sinus node
AV node
Arrhythmias
Pacing: paced rhythm analysis
Capture
Sensing
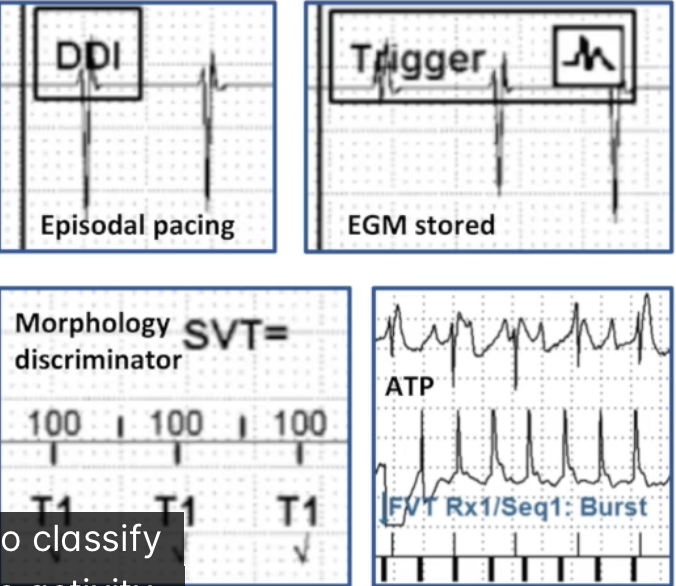
Tachy EGM Analysis: Step 3
Classify device activity
Algorithms (mode switch)
VT/VF detected
Clinical or induced
Discriminators
Episodal pacing
Therapy delivery
Charge delivered/aborted
EGM stored
Tachy EGM Analysis: Step 4
Conduct detailed left to right analysis of markers and IEGMs
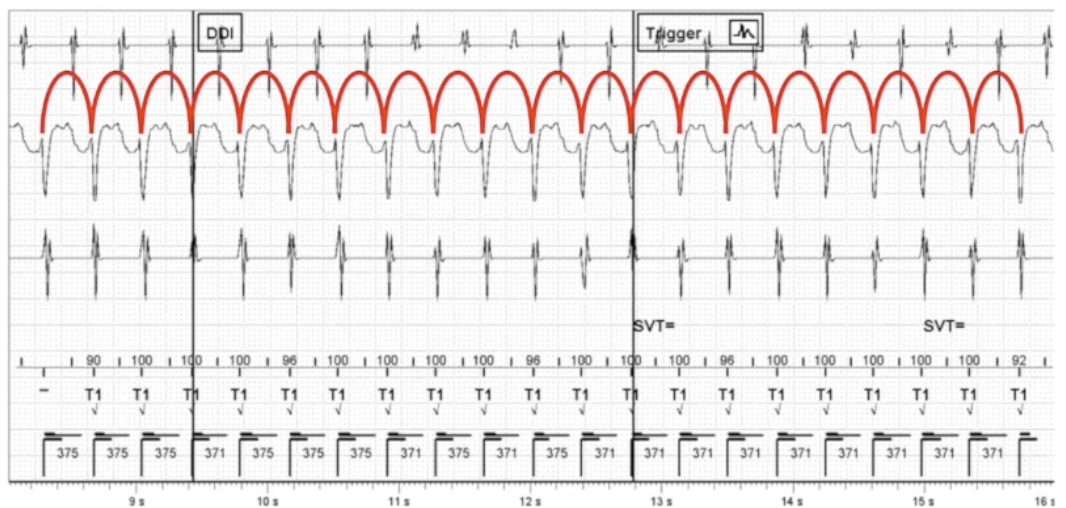
First Component of Tachy Analysis
Evaluate detection
Confirm rhythm detected
Evaluate sensing
Assess discriminator function
Second Component of Tachy Analysis
Evaluate therapy
Determine success for type of therapy delivered
Shock: conversion, energy, charge time, impedance
Third Component of Tachy Analysis
Determine need for reprogramming
Other Tachy Information
Patient history:
Indications
Arrhythmias
Medications
Symptoms
Episode details
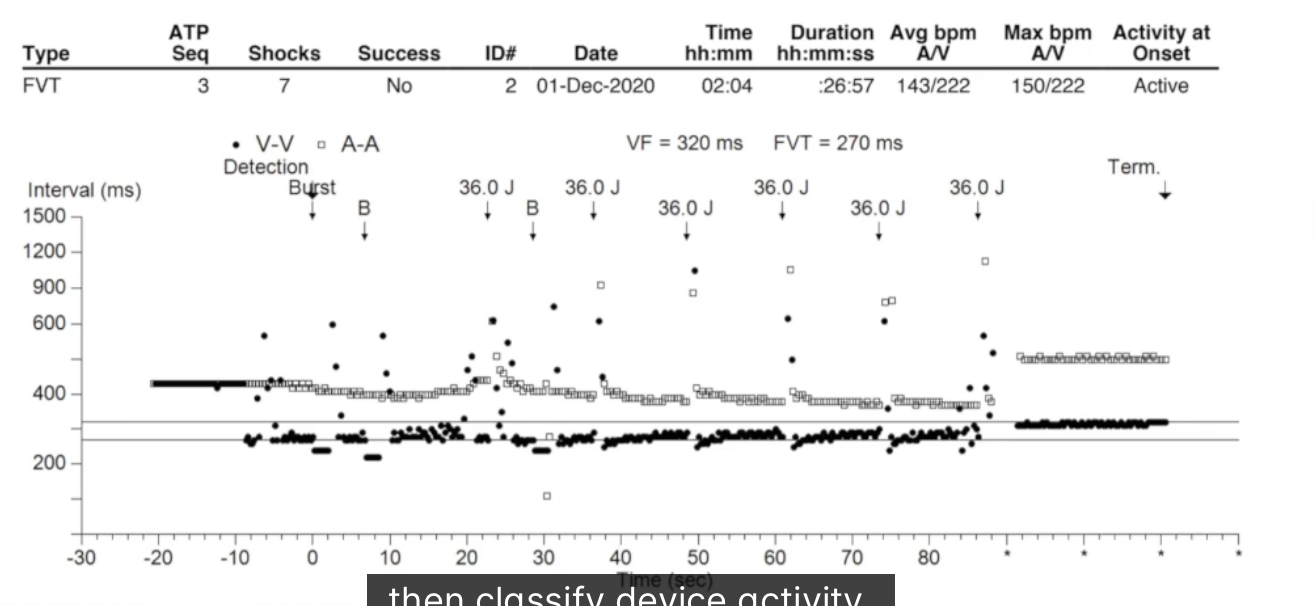
Scatter Plots Tachy Analysis
Can tell a basic story
CRT EGMs
CRT-P: pacing therapy only
CRT-D: includes tachy therapy
Goal of CRT: 100% BIV pacing to reverse remodel the heart
Analyze EGMs to optimize therapy for non-responders
Gather Information CRT
Patient history
Tachy indication: CRT-D
Reduced BIV pacing:
AF with RVR
Frequent PVCs
Loss of capture:
Electrolyte imbalances
Medications
Diseases/procedures
Device/leads
Parameters/algorithms/diagnostics
CRT Strip
CRT orient yourself to the strip
BIV Capture
Differentiate true BIV capture, RV only capture, LV only capture, RV anodal capture
Compare morphologies:
Presenting rhythm
Underlying rhythm
RV only threshold
LV only threshold
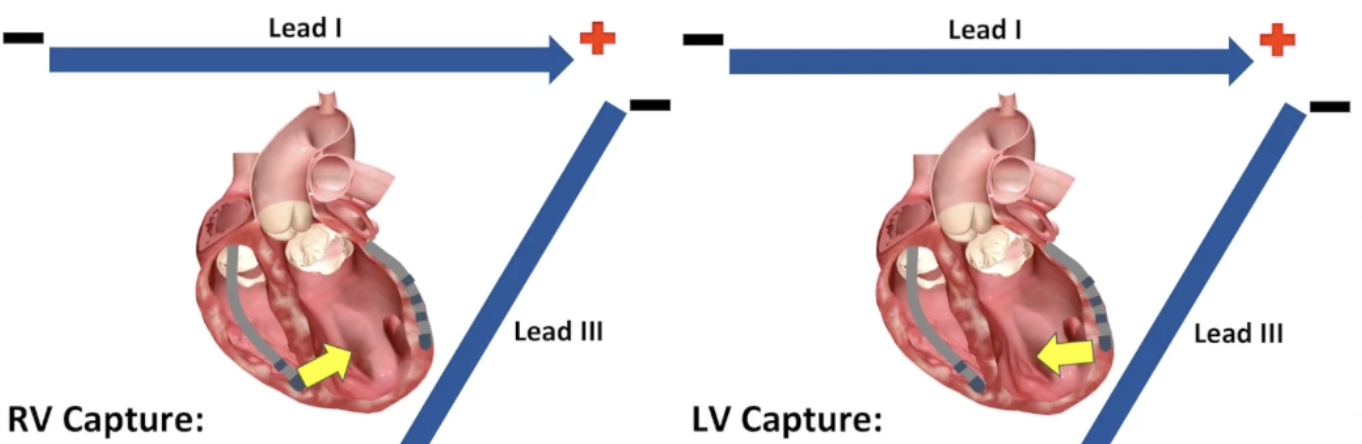
CRT Capture on the Surface ECG
RV Capture:
Lead I: more positive
Lead III: more negative
LV Capture:
Lead I: more negative
Lead III: more positive
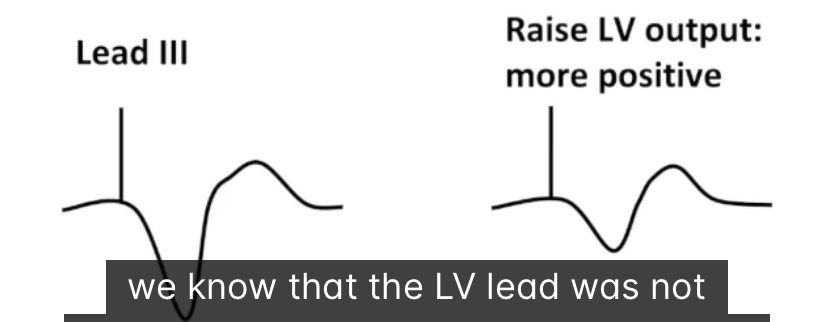
Example CRT Capture on the Surface ECG
Example: BIV pacing, suspect loss of LV capture
Raise LV output
Lead I more negative, lead I!! more positive
LV was not capturing before
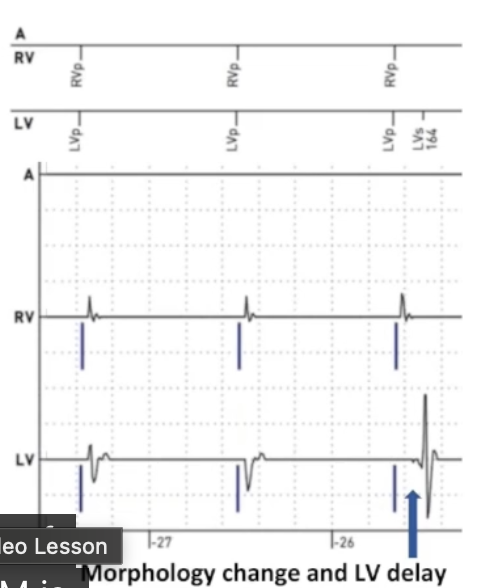
CRT LV EGM
Loss of LV capture difficult to see on surface ECG
Nearfield helps to differentiate intrinsic/paced
Lost capture: delay between pacing and LV signal
No capture at all: LBBB
Only RV capture: cell to cell activation from RV lead
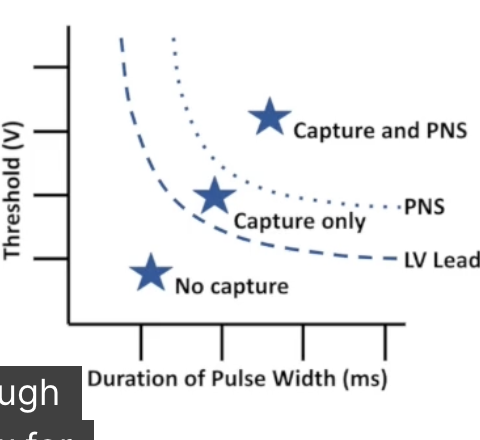
CRT Threshold Testing
RV: same as other devices
LV: additional considerations
Many pacing configurations
RV anodal capture
Phrenic nerve stimulation
CRT Phrenic Nerve Stimulation
Output must be lower than PNS threshold
May require safety margin < 2:1
Can test different vectors instead
PNS is positional
Different thresholds when sitting/standing/supine
Often discovered after implant
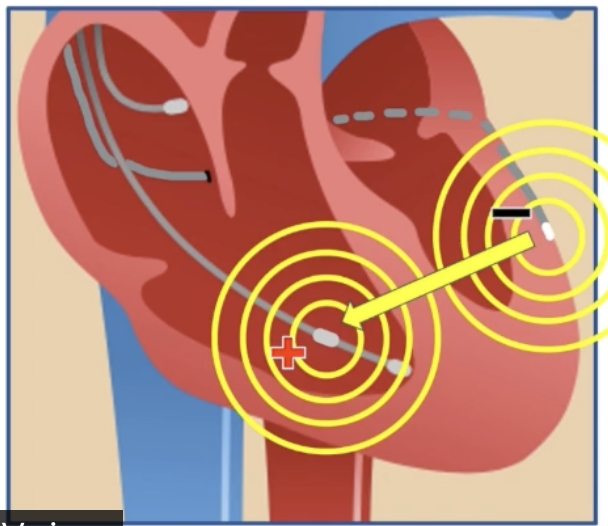
CRT Anodal Stimulation
Depolarization caused by electrons returning to positively charged anode
Higher threshold than cathodal capture
RV leads:
Anode has larger surface area: anodal capture less likely
Close spacing of anode and cathode: anodal capture less significant

CRT Extended Bipolar Configuration
LV pacing vector only on LV lead: anodal stimulation not a problem
Extended bipolar:
Anode on RV lead (ring or coil)
LV thresholds higher than RV thresholds
RV anodal threshold similar to LV cathodal threshold
Particularly likely with ring (CRT-P or dedicated bipolar CRT-D)
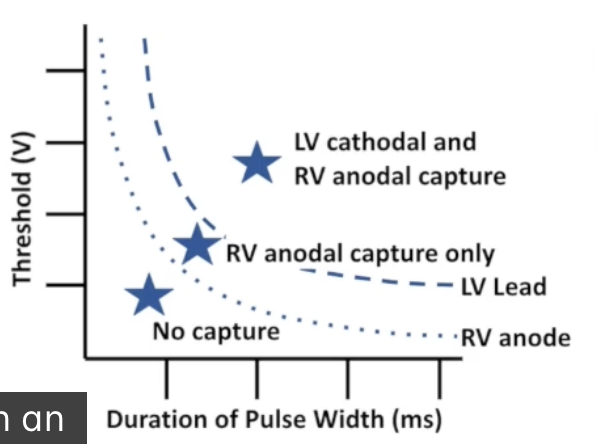
CRT Problems with Anodal Stimulation
RV anodal threshold lower than LV cathodal threshold:
Confuse RV anodal capture for LV capture
Set LV output too low
Begin at output with RV anodal capture only, decrement until RV anodal capture is lost
No LV capture: no therapy
CRT Avoiding Anodal Stimulation Errors
Be wary when testing in extended bipolar configuration
Start at high enough outputs to ensure LV capture
Continue until there is true loss of capture
Include RV and LV nearfield EGMs
Use surface ECG if available
CRT Electronic Repositioning
Older devices: limited options
Quadripolar: many possible vectors
Choose lowest LV threshold with no PNS
Be wary of anodal stimulation with extended bipolar
Vary pulse width if thresholds are high
High impedance decreases energy use
CRT AV Delay Optimization
Intrinsic conduction: competition with BIV pacing
Inhibition
Functional non capture
Fusion
Pseudofusion
Program short enough to ensure 100% BIV capture
Program long enough to maintain AV synchrony
Fusion is acceptable, sometimes preferable
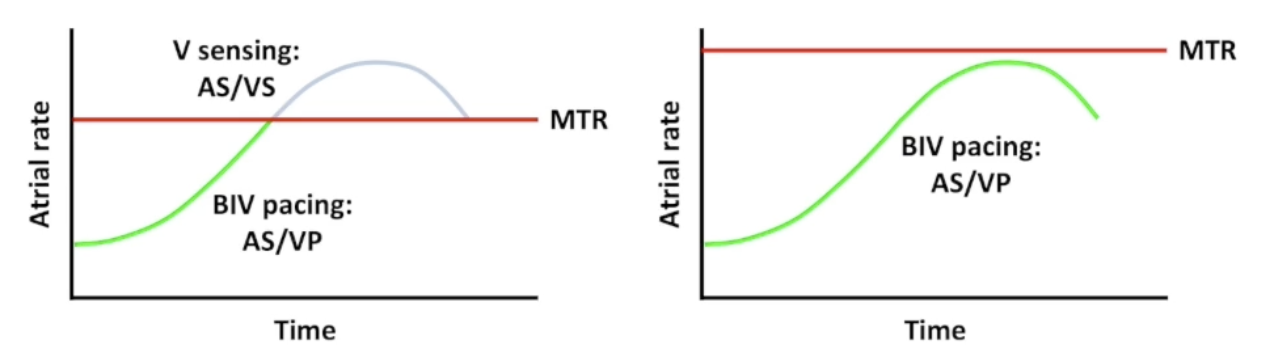
Upper Rate Behavior
Atrial rate faster than MTR:
CHB: pacemaker Wenckebach and fixed ratio block
No CHB: intrinsic rate comes through, lower % BIV pacing
Common to increase MTR in CRT devices