NPTE: Non/Other Systems
1/150
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
151 Terms
ethic question
answer C (call 911)
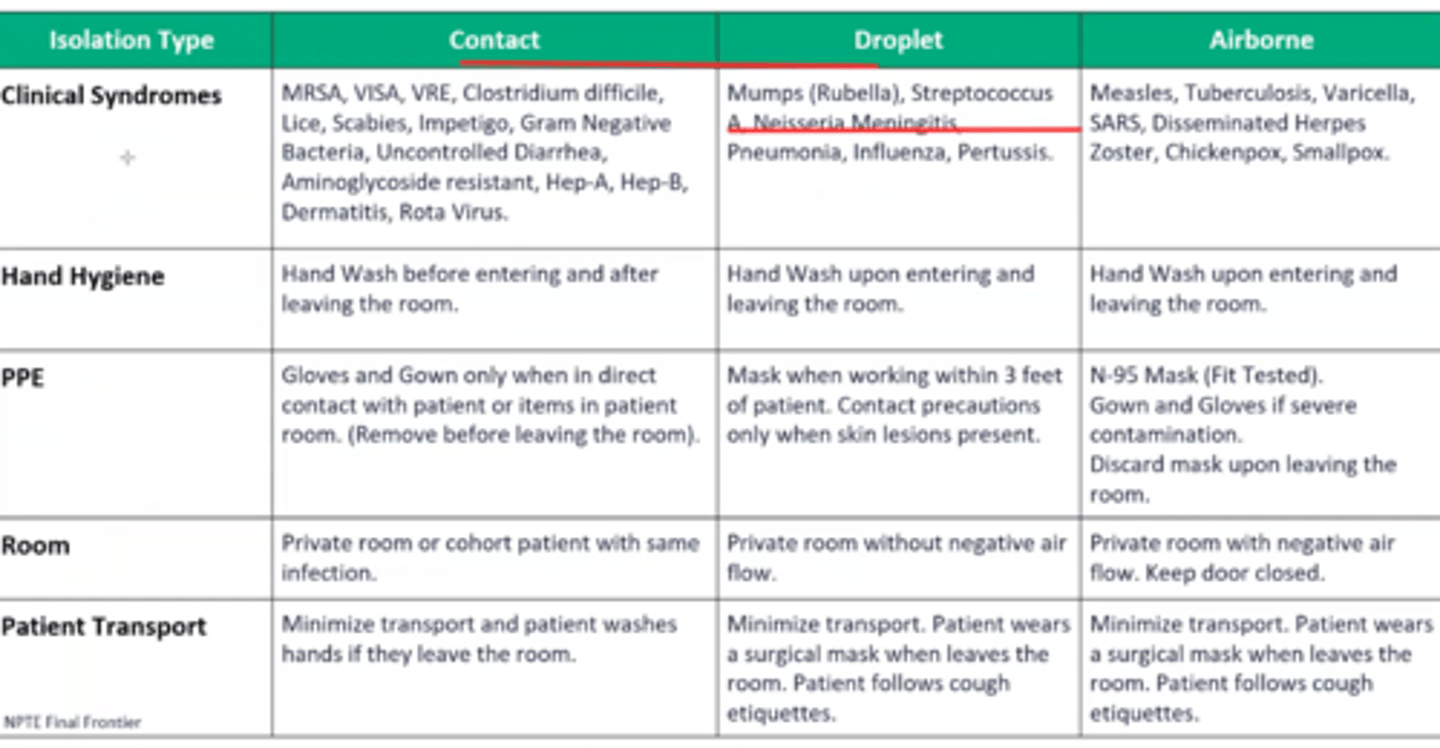
Contact vs droplet vs airborne
o Airborne
§ Measles
§ TB
§ Varicella
o Droplet
§ Sepsis/scarlet fever/strep
§ Parvovrisu B19/pneumonia/pertussis
§ Influenza
§ Diphtheria (pharyngeal)
§ Epiglottis
§ Rubella
§ Mumps/meninigitis/myocoplasma/meningeal/pneumonia
§ Adenovirus
o Contact
§ Multi drug resistant organism
§ Respiratory infection
§ Skin infections
§ Wound infections
§ Enteric (C DIFF)
§ Eye infection (conjunctivitis)
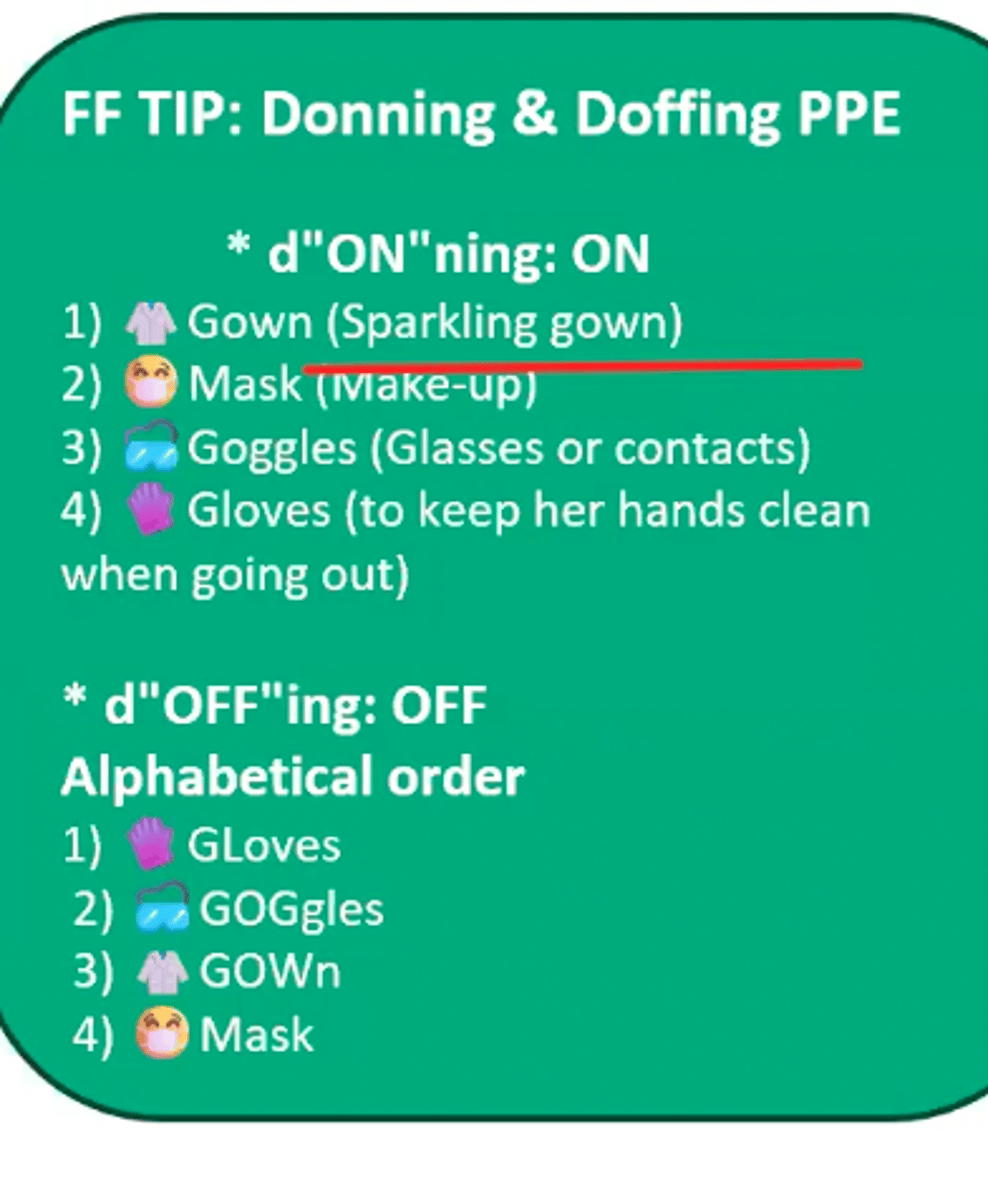
Donning and doffing
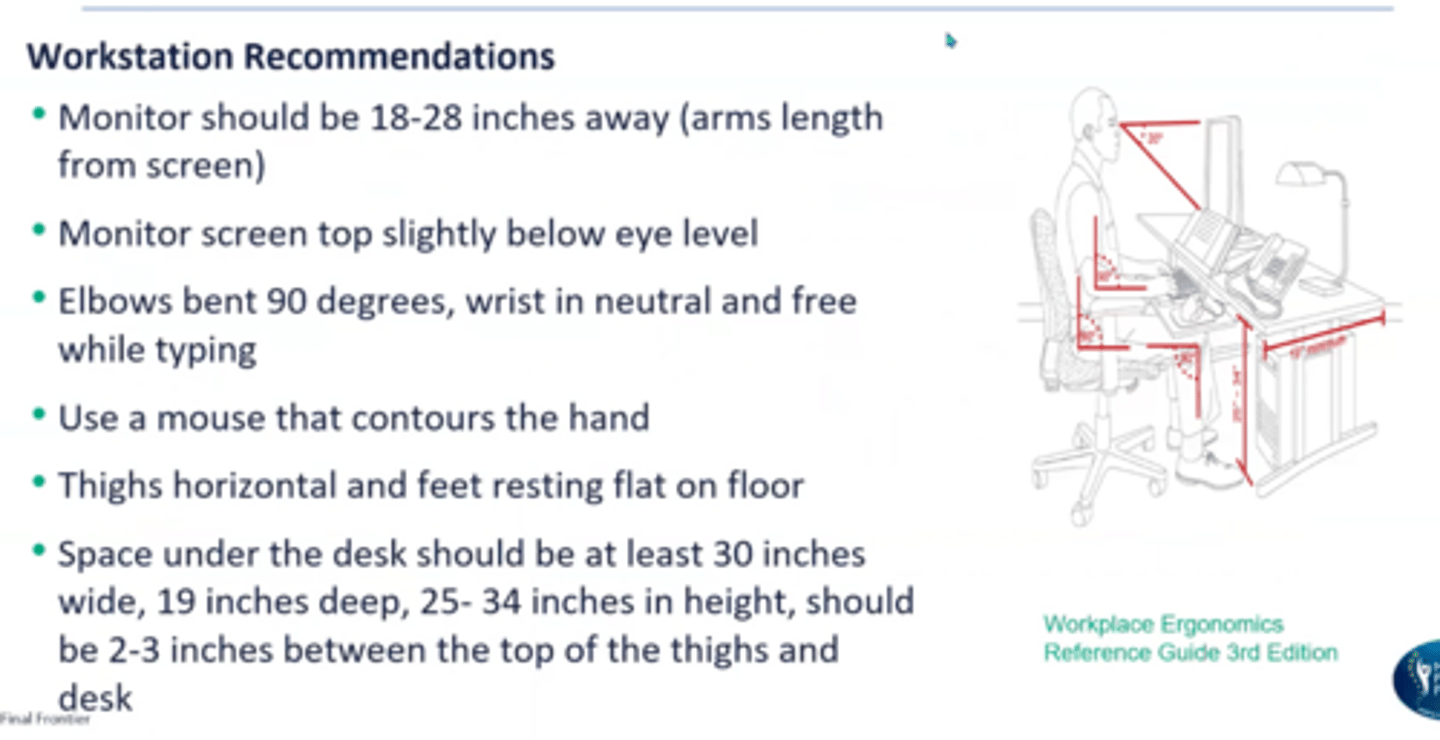
Workstation ergonomics
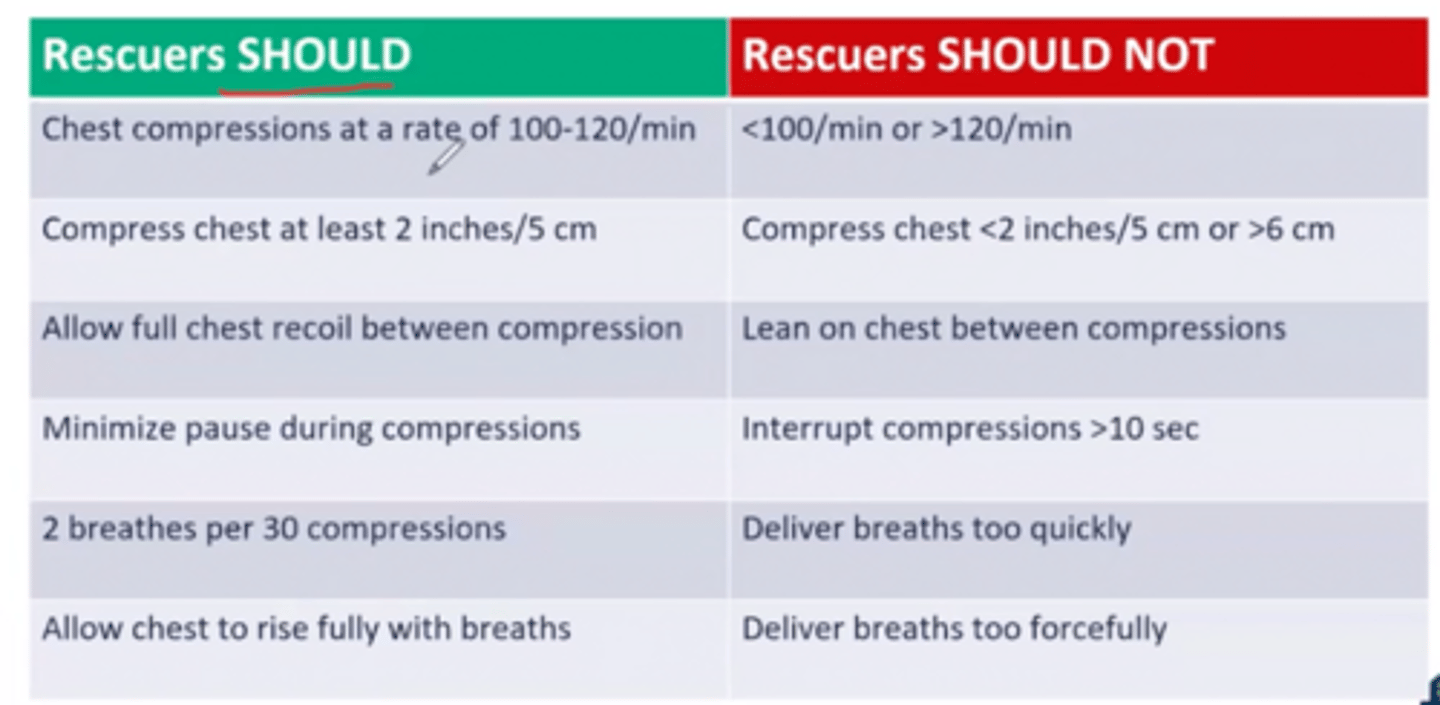
CPR do's and don'ts
-chest compressions at a rate of 100-120/min
-compress chest at least 2 in/5 cm (baby is 1.5 in)
-allow full chest recoil between compression
-minimize pause during compressions
-2 breaths per 30 compressions
-allow chest to rise fully with breaths
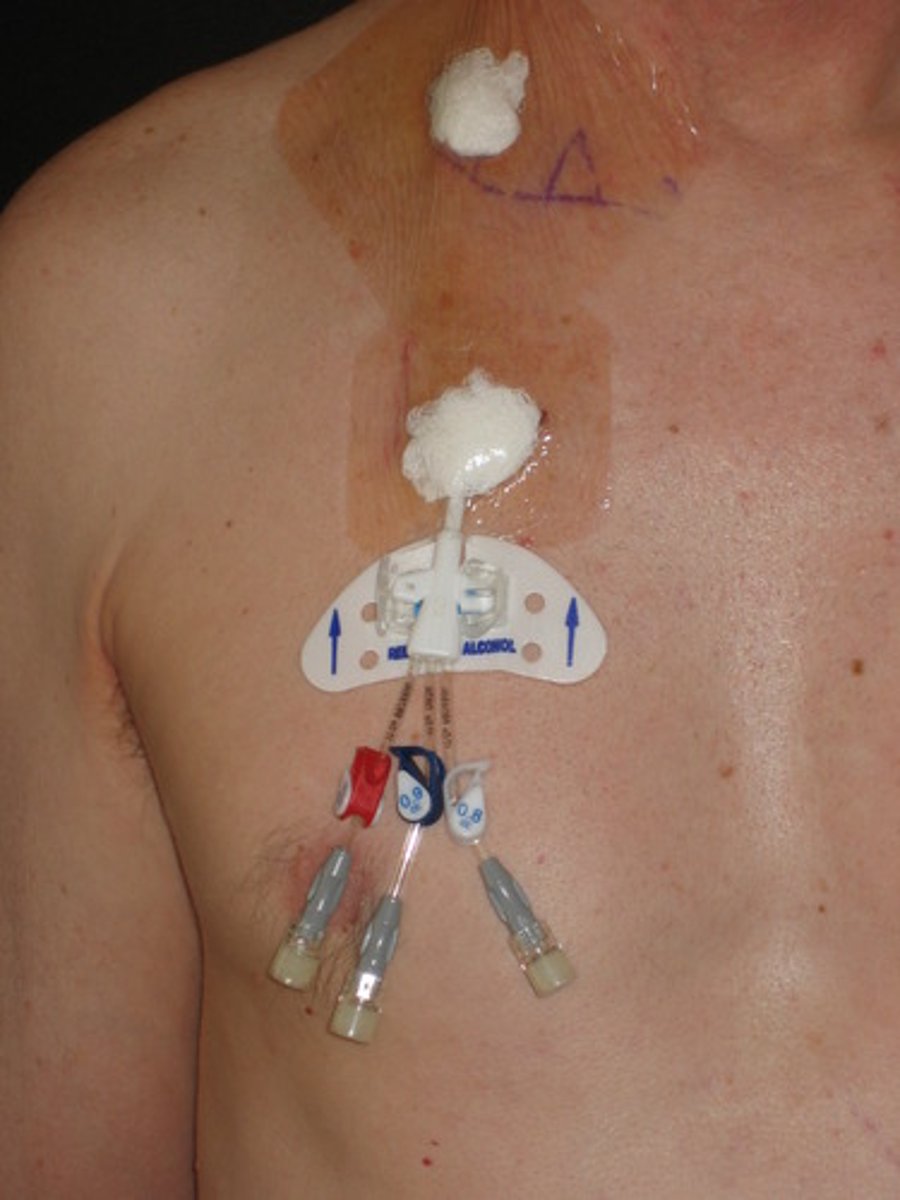
Hickman catheter
-central line tunneled under the skin
-provides antibiotics, nutritional solutions and blood samples
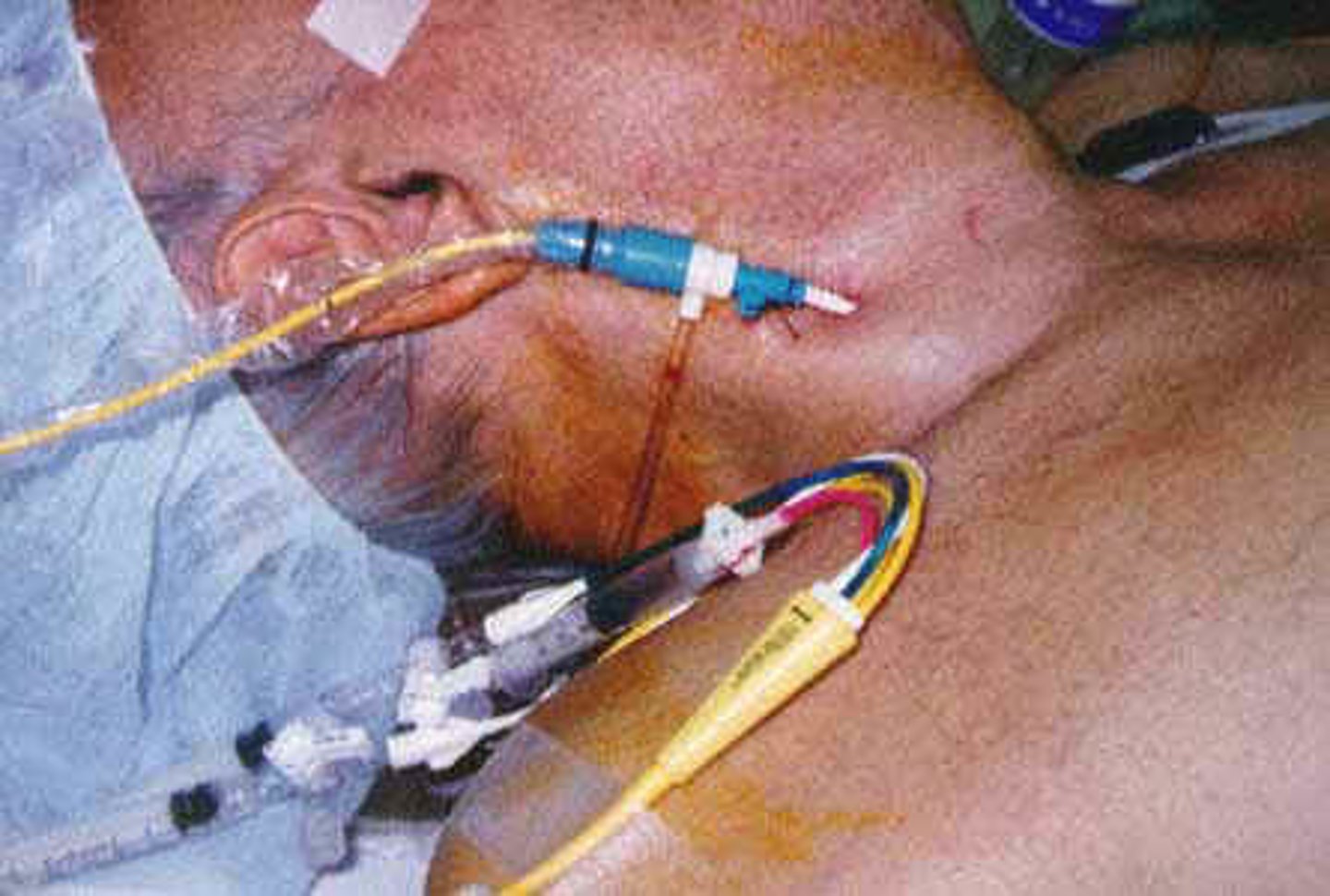
Swan ganz catheter
-balloon flotation device inserted through the internal jugular vein or femoral vein into the pulmonary artery
-monitors blood flow and the function of the heart
Colostomy bag
-exits the colon to the abdomen (stoma) when a part of the colon or large intestine has been removed
-seen with colon cancer
-focus on early mobility and beware of gait belt!! (if you use one place it above)
Central venous pressure catheter
measures blood pressure directly from right atrium and superior vena cava

Arterial line
monitor arterial blood gases
-if dislodged, apply firm pressure and alert nursing immediately

Chest drainage tube
- Inserted through an incision in the chest and may be
connected to a mechanical or gravity-based suction
system
- Used to remove air, blood, purulent matter from the
patient's chest or pleural cavity
if dislodged, have the patient exhale, place gauze or a gloved hand over the area and call nursing staff, keep collection bottle below tube
IV lines cautions
arms should not be held above head for extended periods, alert staff if fluid is low due to air bubbles
femoral line cautions
avoid repetitive hip flexion and hip flexion >45 degrees
Catheters cautions
hang below level of bladder, do not empty bag if output is being monitored, empty or alert staff if overfilled
A clinician is preparing to ambulate with a patient with pleural effusion and a chest tube. Which of the following procedures is most important to consider?
collection bottle should be kept below the level of the inserted tube
3 multiple choice options
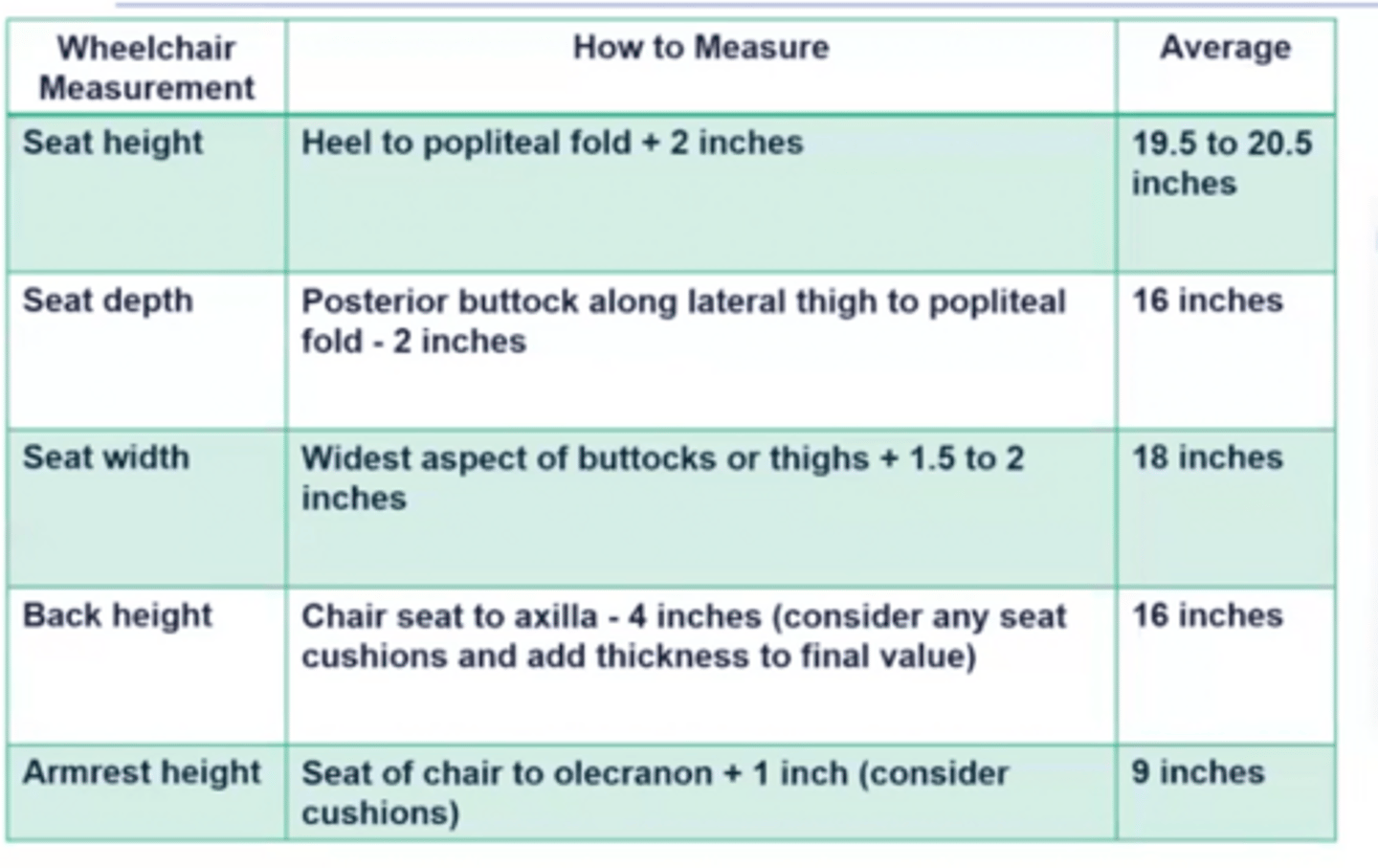
Wheelchair measurements
Wheelchair axle positioning
-normal is in line with the shoulder or slightly posterior
-bariatric patients then move the rear wheel axle forward
-bilateral transfemoral amputation then move the rear wheel axle behind the patient's shoulders
How to teach a wheelchair wheelie
lean forward, gait belt to rear axle
-patient places hands back on the hand rims, then push them forward abruptly and forcefully
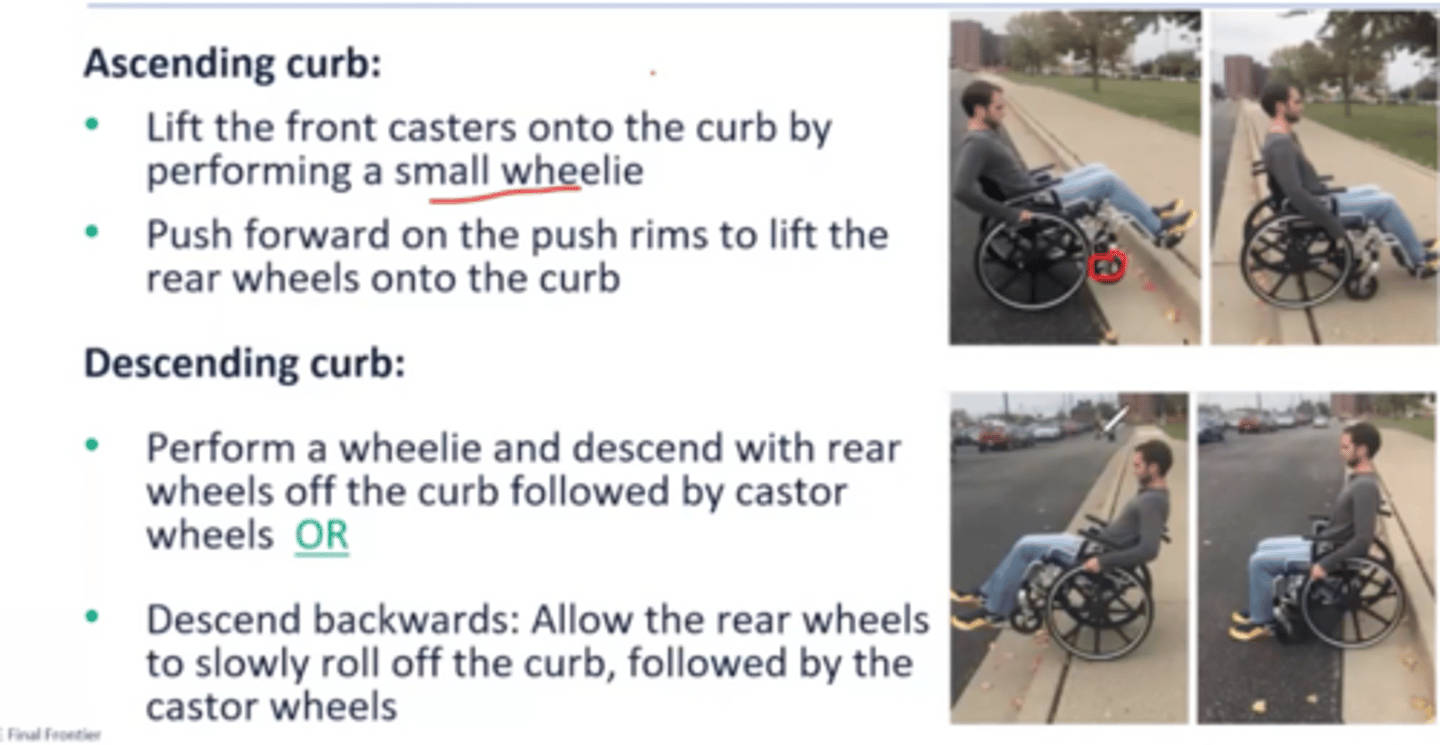
Ascending and descending curb
Posterior vs anterior hip replacement precautions
posterior: no flex >90, no adduction, no IR
anterior: no flex>90, no adduction, no ER, no extension past neutral, in combination cannot FABER (AAAA AVOID PIVOTING AWAY (ER)
Which of the following is most likely to be included while educating a patient on prevention of hip dislocation? they had an anterior THA
avoid standing activities that involve rotating the body away from the operated extremity
Do you transfer to strong or weak side?
strong
Gait pattern for anterior THA
front wheeled walker and step to gait pattern (cannot do step thru because NO HIP EXT can be done)
Standard crutches vs forearm crutches vs cane fitting
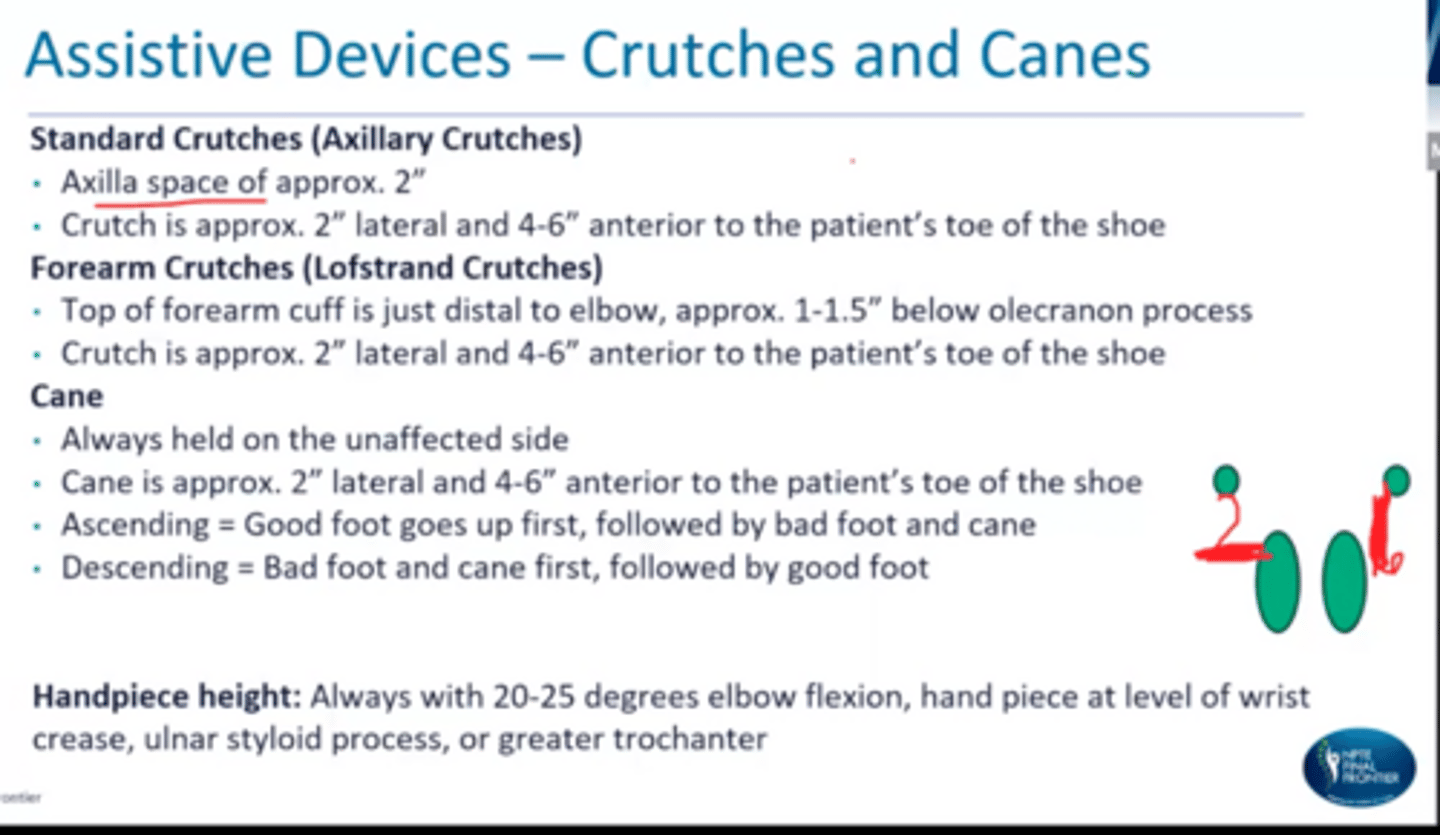
Nerve for crutch palsy
radial nerve or brachial plexus
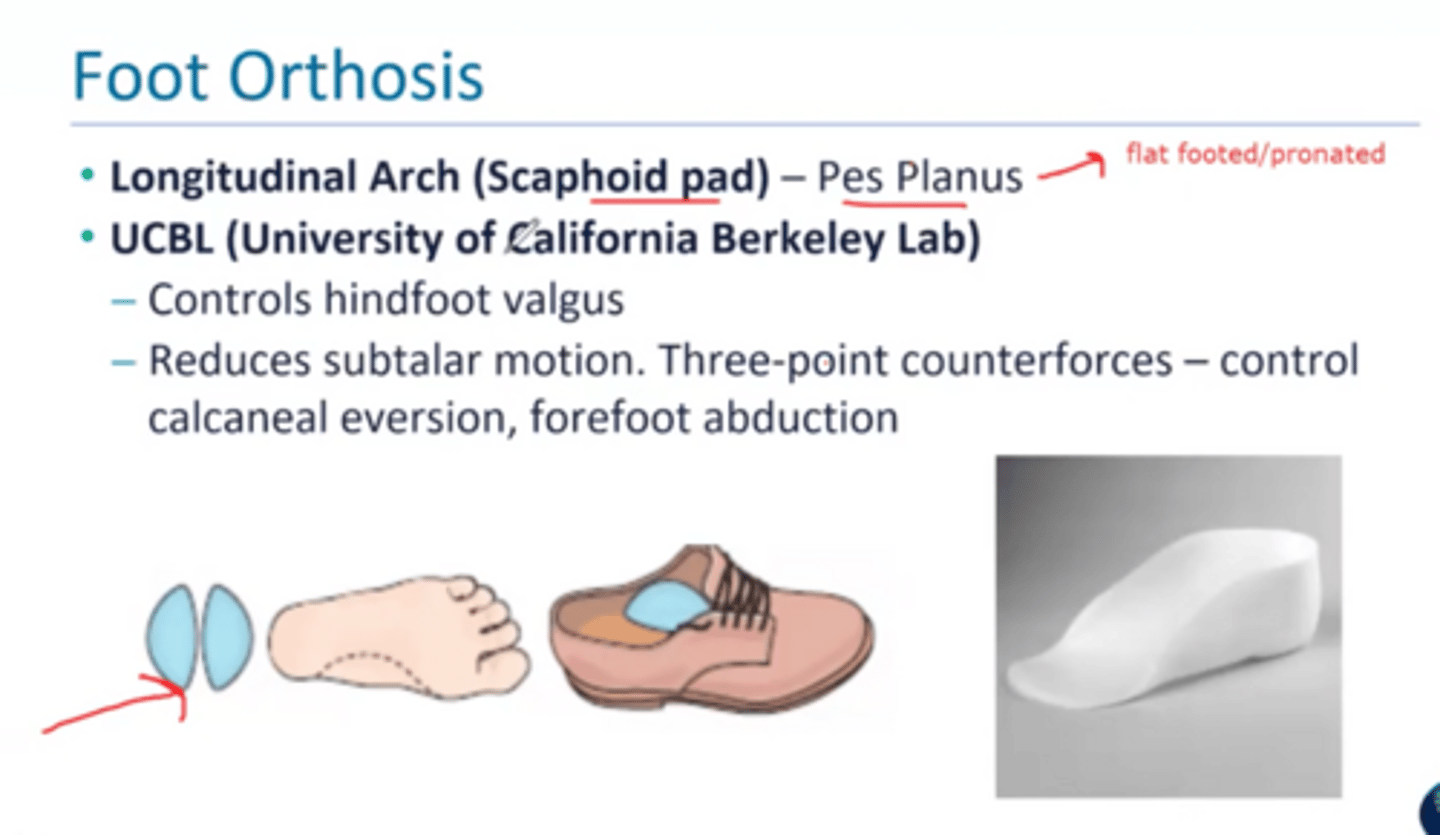
Longitudinal arch and UCBL orthosis
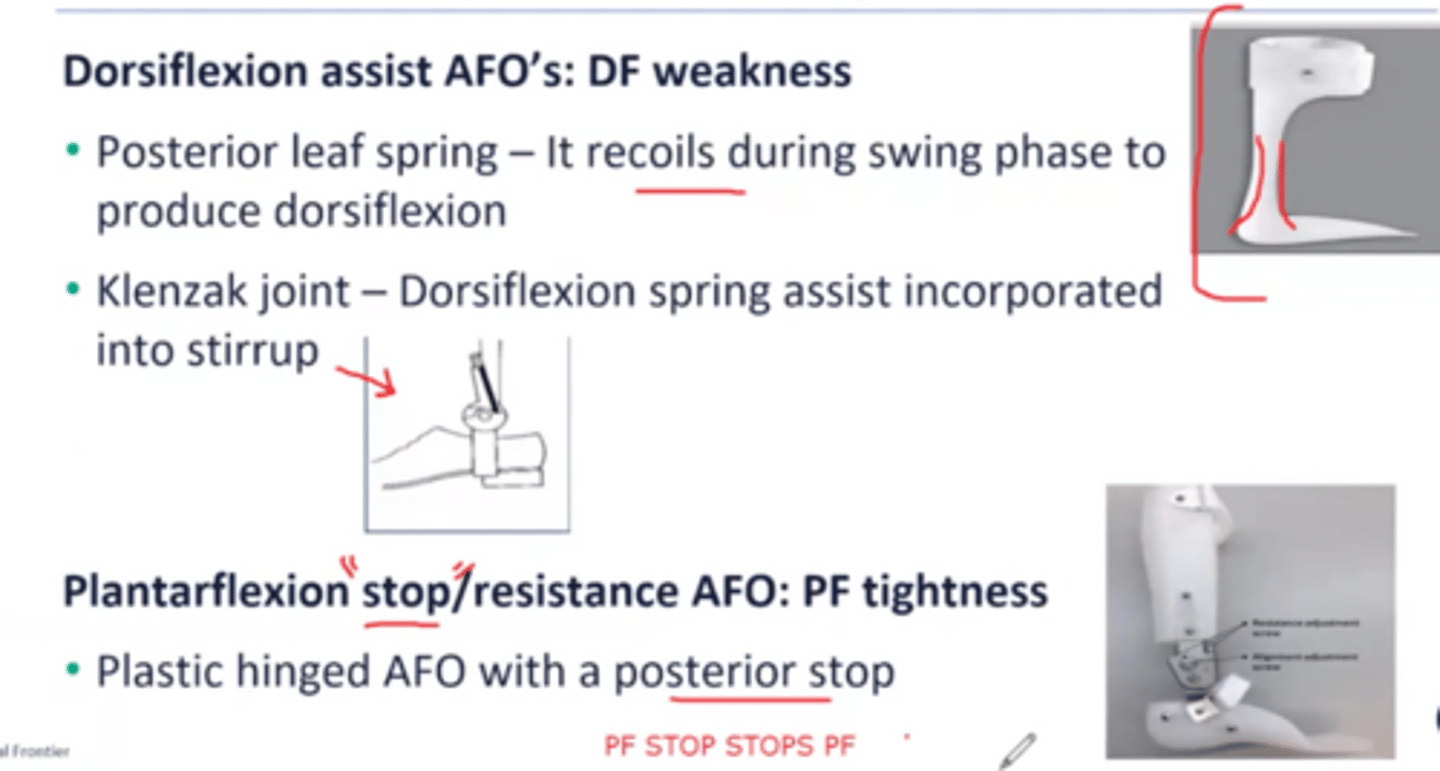
Posterior leaf spring vs klenzak joint vs plantarflexion stop
What will excessive height of medial vs lateral upright KAFO cause?
medial: lateral trunk lean
lateral: medial trunk lean
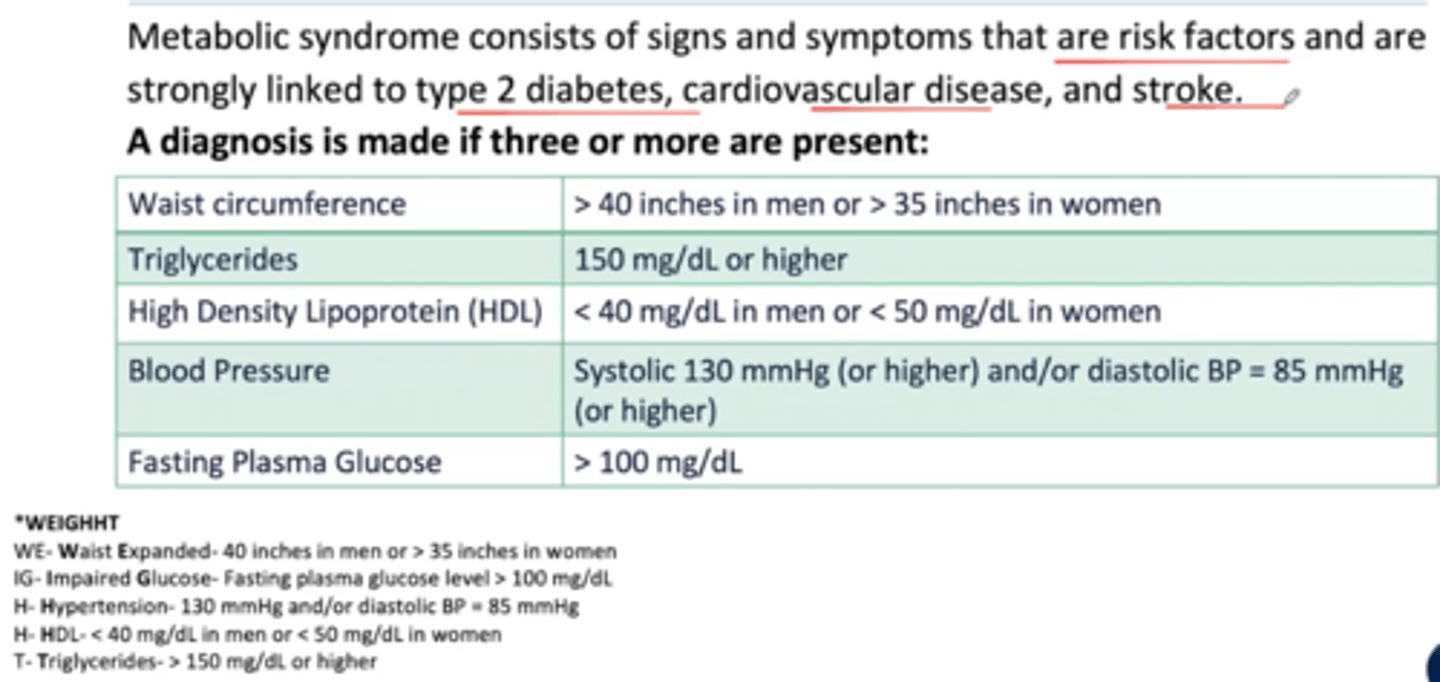
A review of the patient's chart shows BP 169/90 mmHg, triglyceride level of 160 mg/dL and a fasting blood glucose of 115 mg/dL. patients body mass index is 40 kgg/m and their waistline is 54 in. What are these findings suggestive of?
metabolic syndrome
3 multiple choice options
Metabolic syndrome
consists of signs and symptoms that are risk factors and are strongly linked to type 2 diabetes, cardiovascular disease and stroke
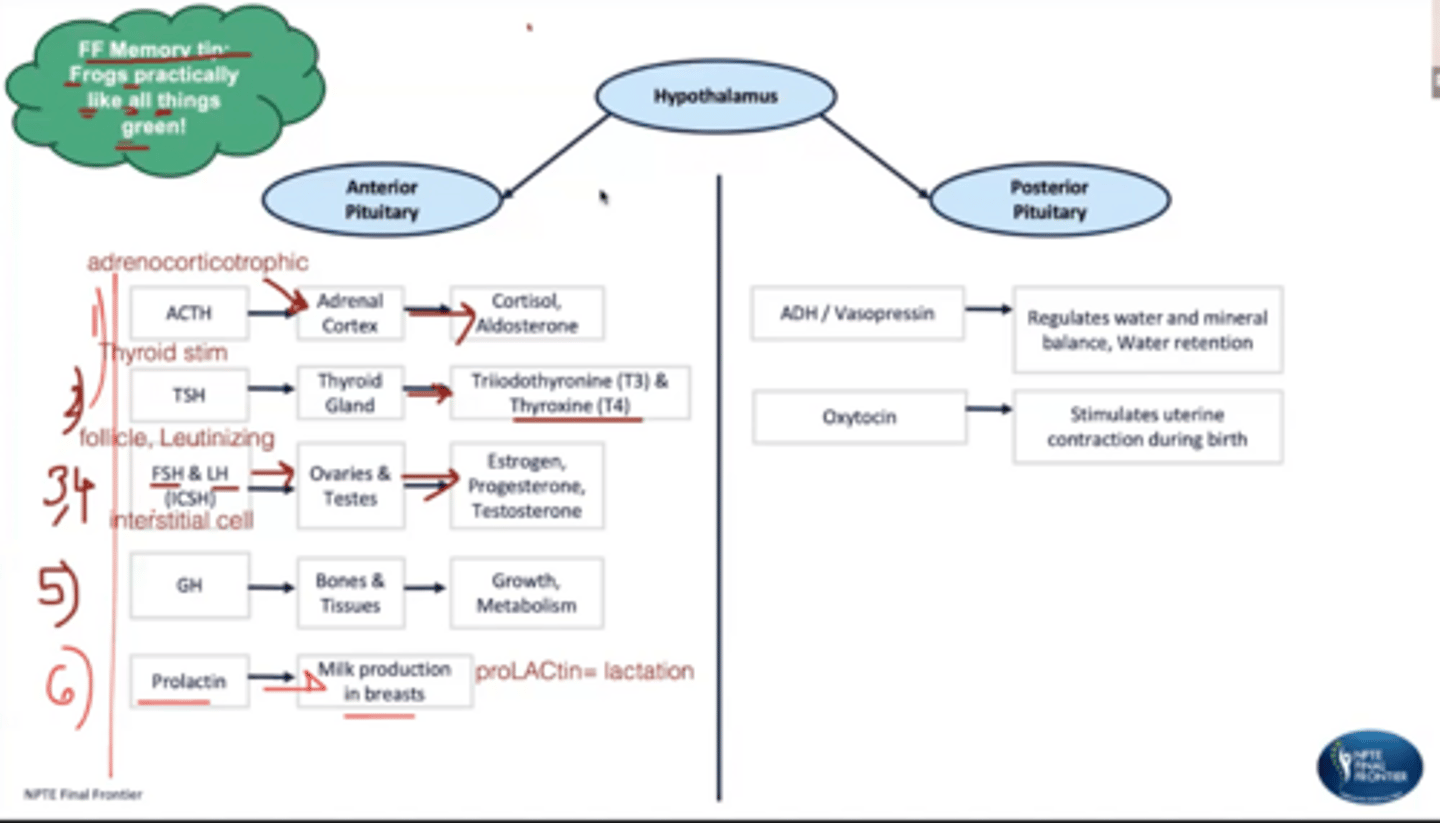
Anterior vs posterior pituitary
frogs practically like all things green for anterior pituitary
FSH
TSH
LH
ACTH
GH
Glands of the endocrine: hypothalamus, pituitary, thyroid, parathyroid, adrenal
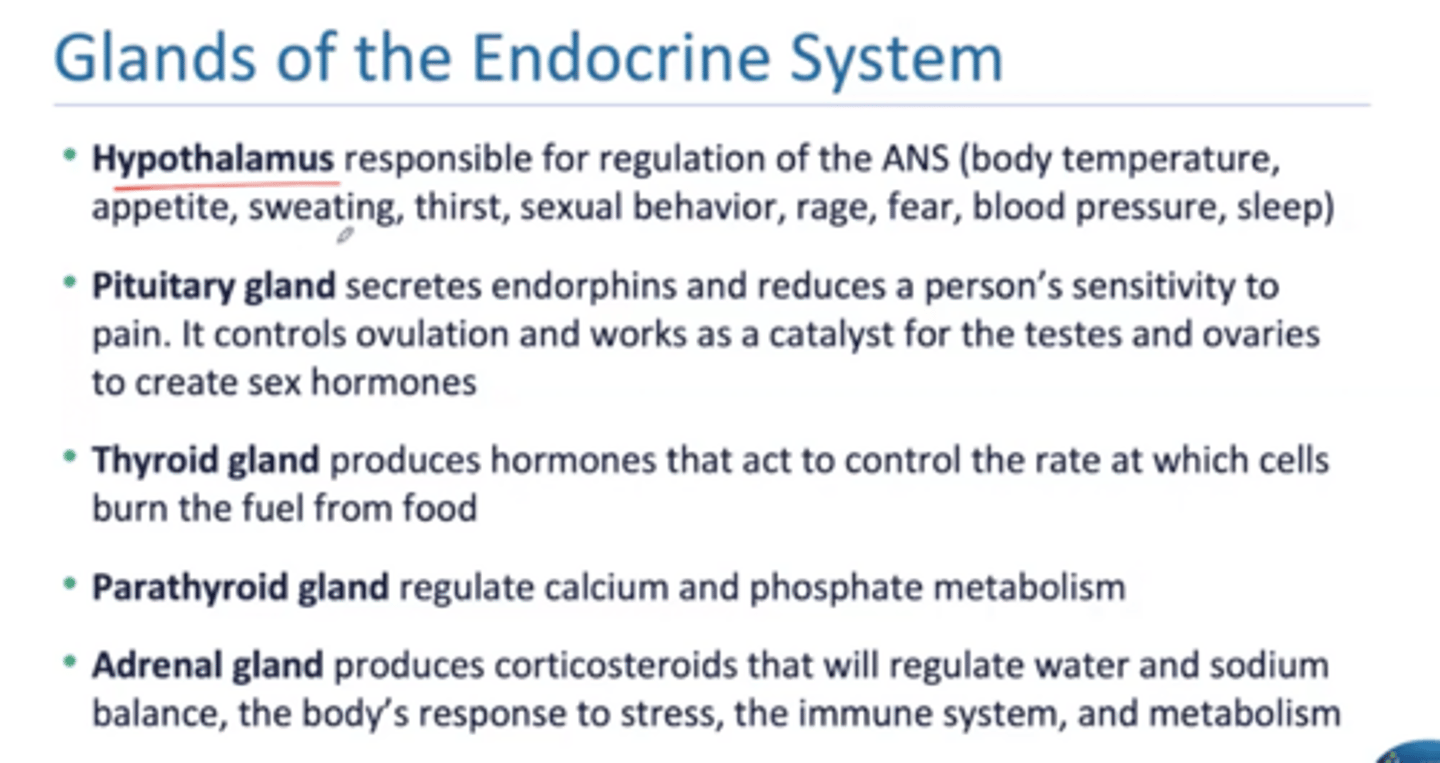
What does cortisol do?
blood pressure, gluconeogensis, regulate stress, decrease inflammation
What does aldosterone do?
retains Na and water, kicks out K+
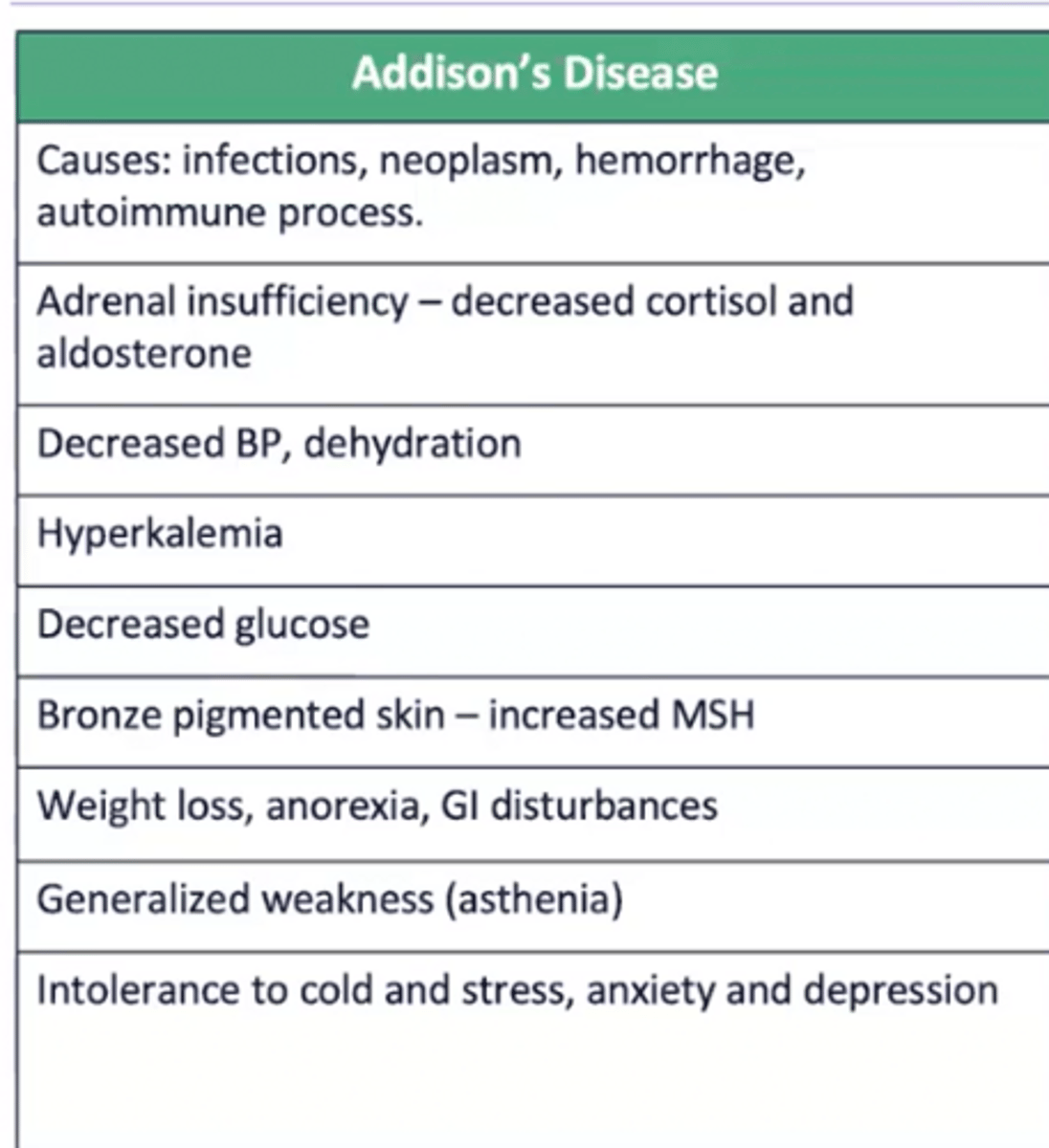
Addison's disease
Mrs. Addison is a brown old petite lady walking with a stick
Secondary adrenal insufficiency
● Lack of pituitary ACTH because of insufficient stimulation of adrenal cortex
● Causes: removal of pituitary gland, rapid withdrawal of drugs, hypothalamic or pituitary tumors
Cushing's disease
Mr. Cushings is a white chubby boy (ruddy appearance) who loves chugging beer or santa clause
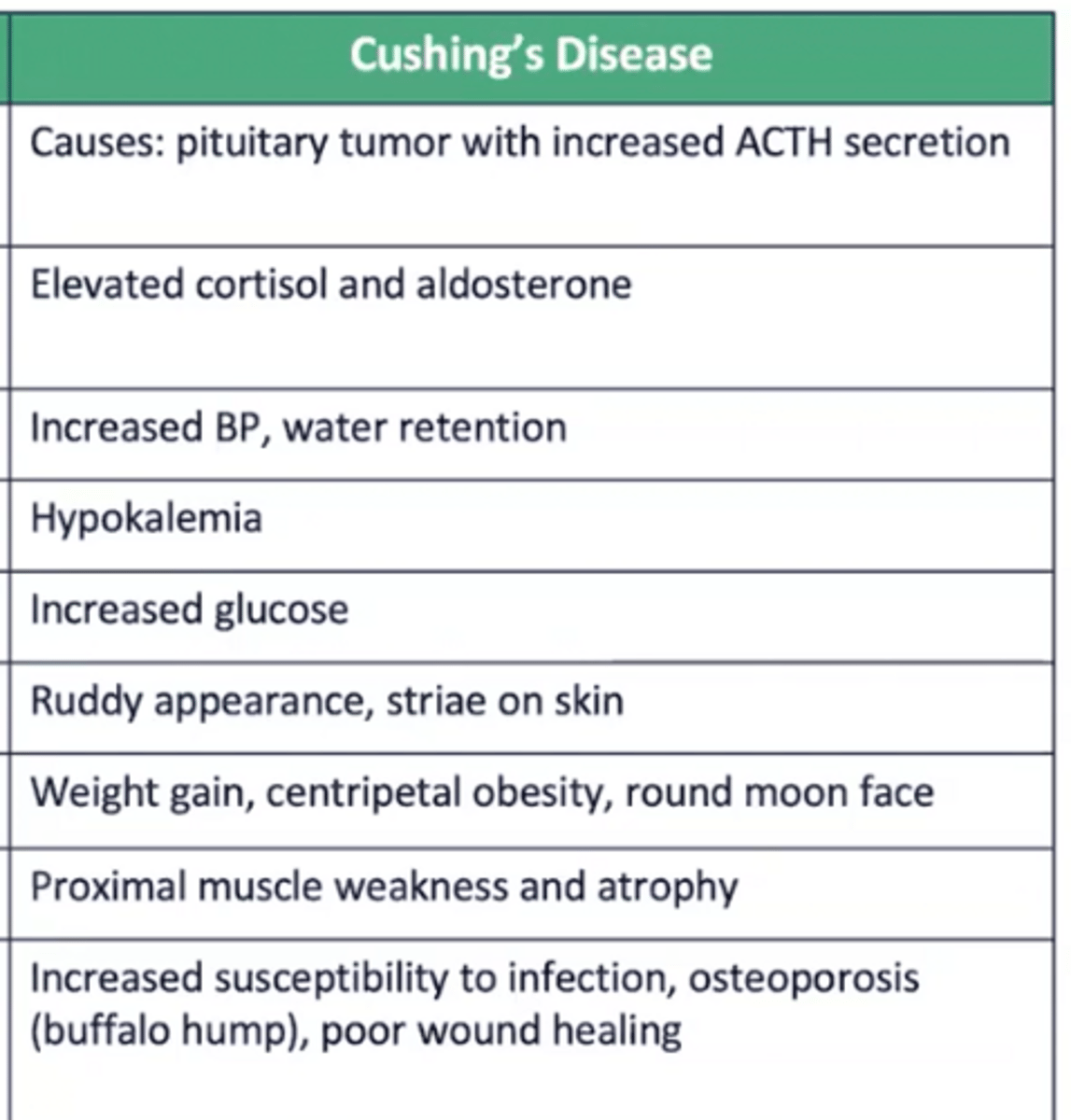
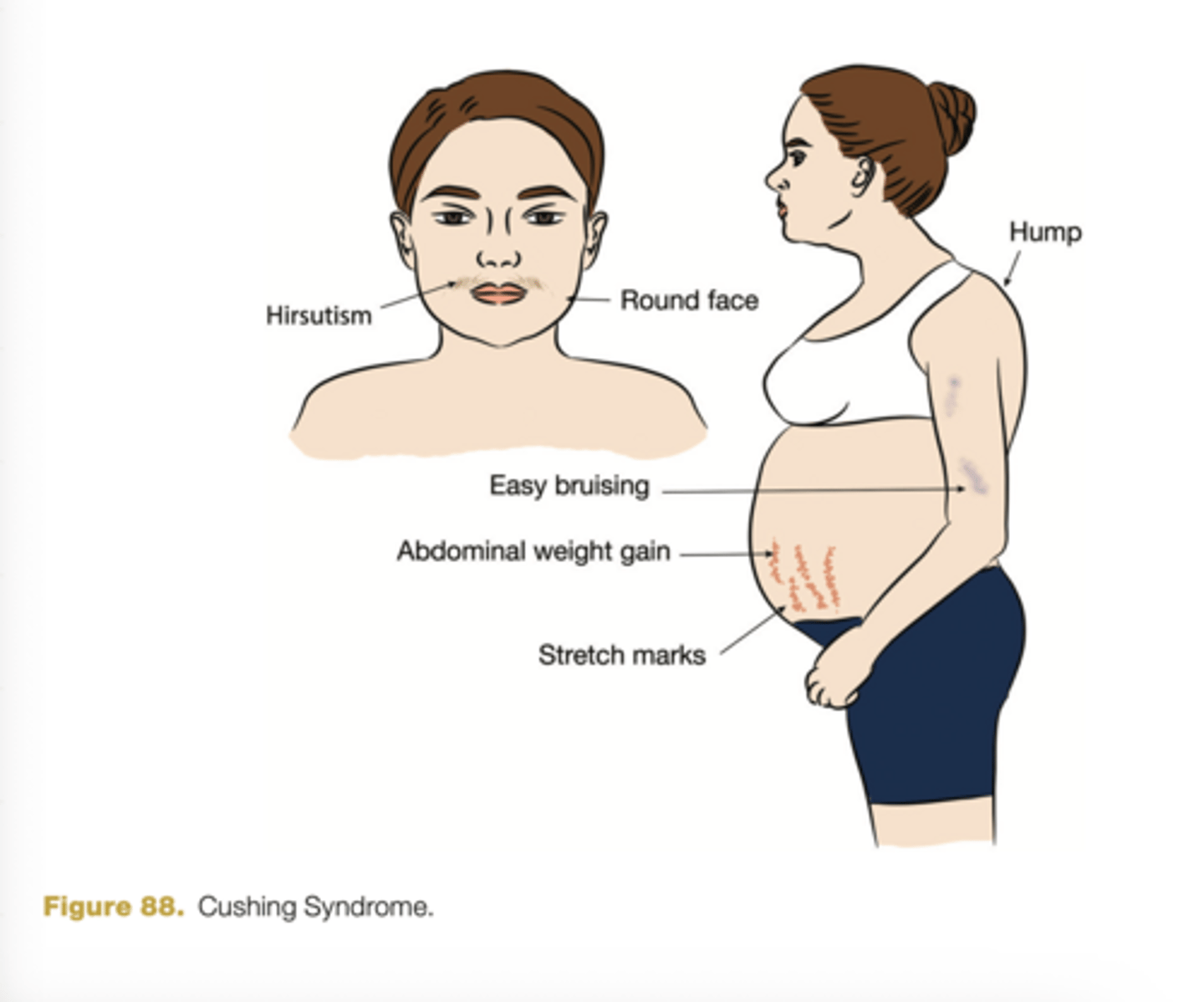
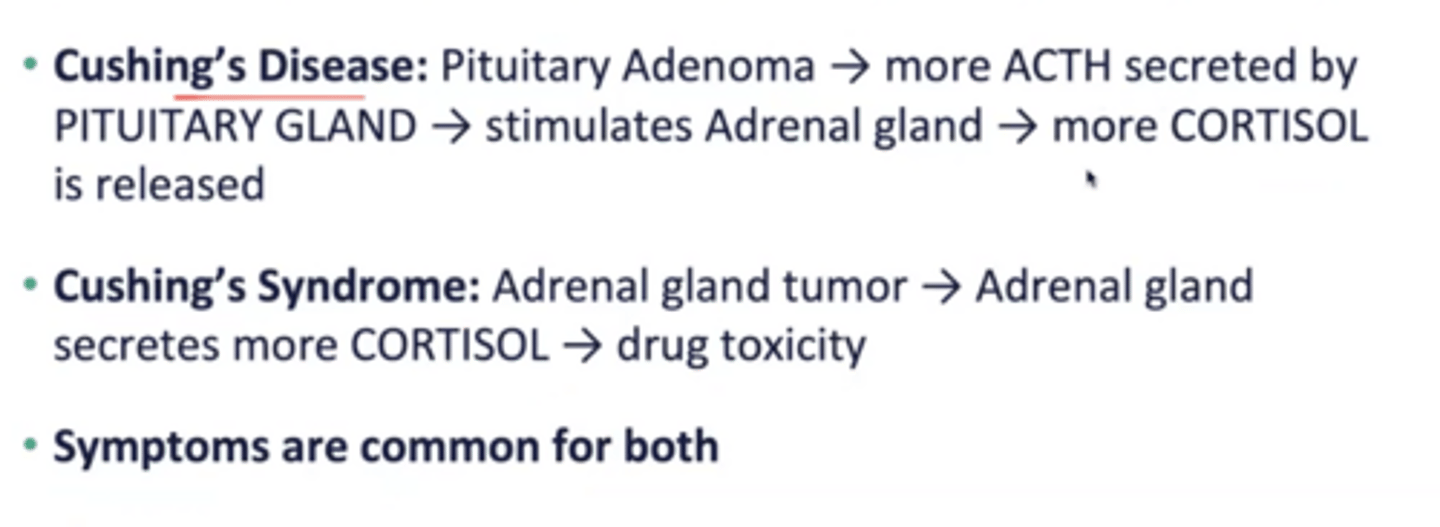
Cushing disease vs syndrome
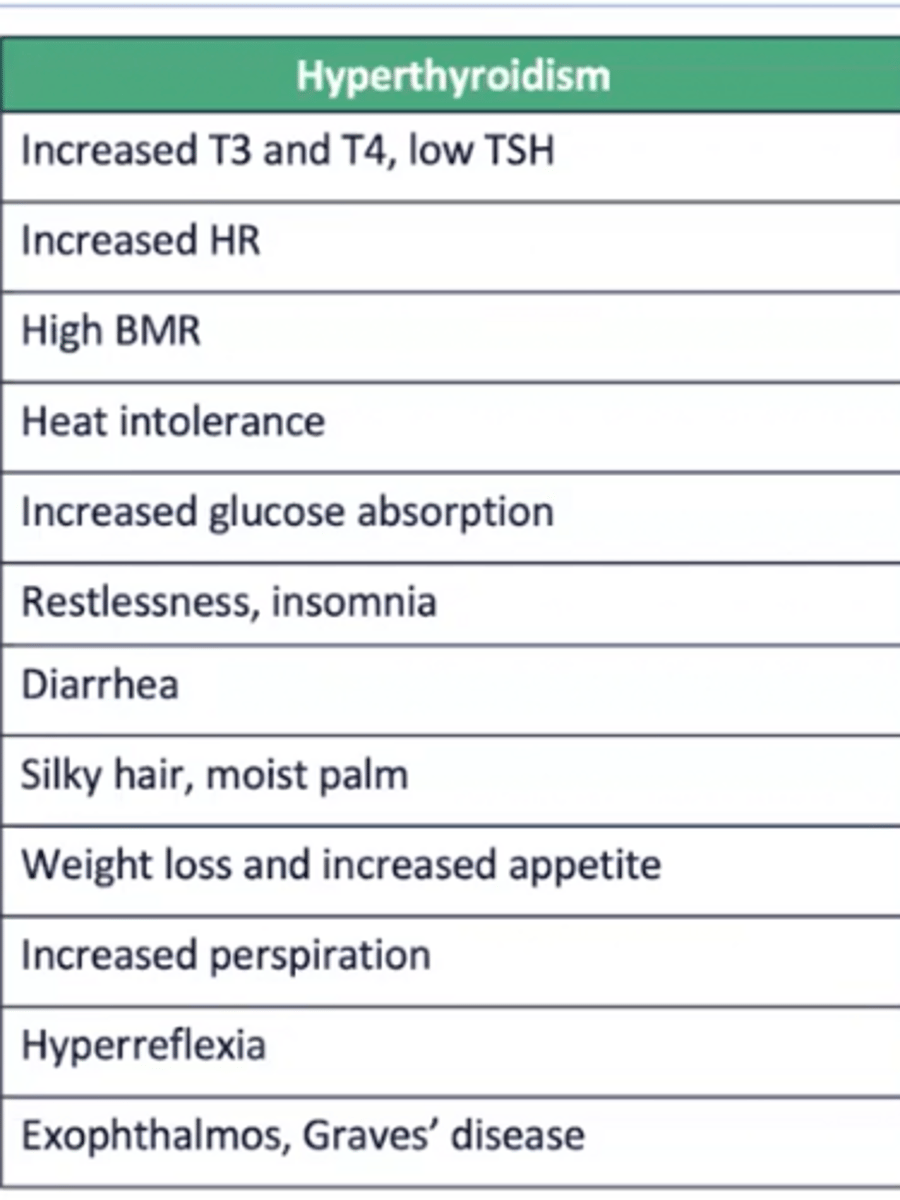
Hyperthyroidism
graves and exophthalmos
(blood pressure decreases; osteoporosis risk)
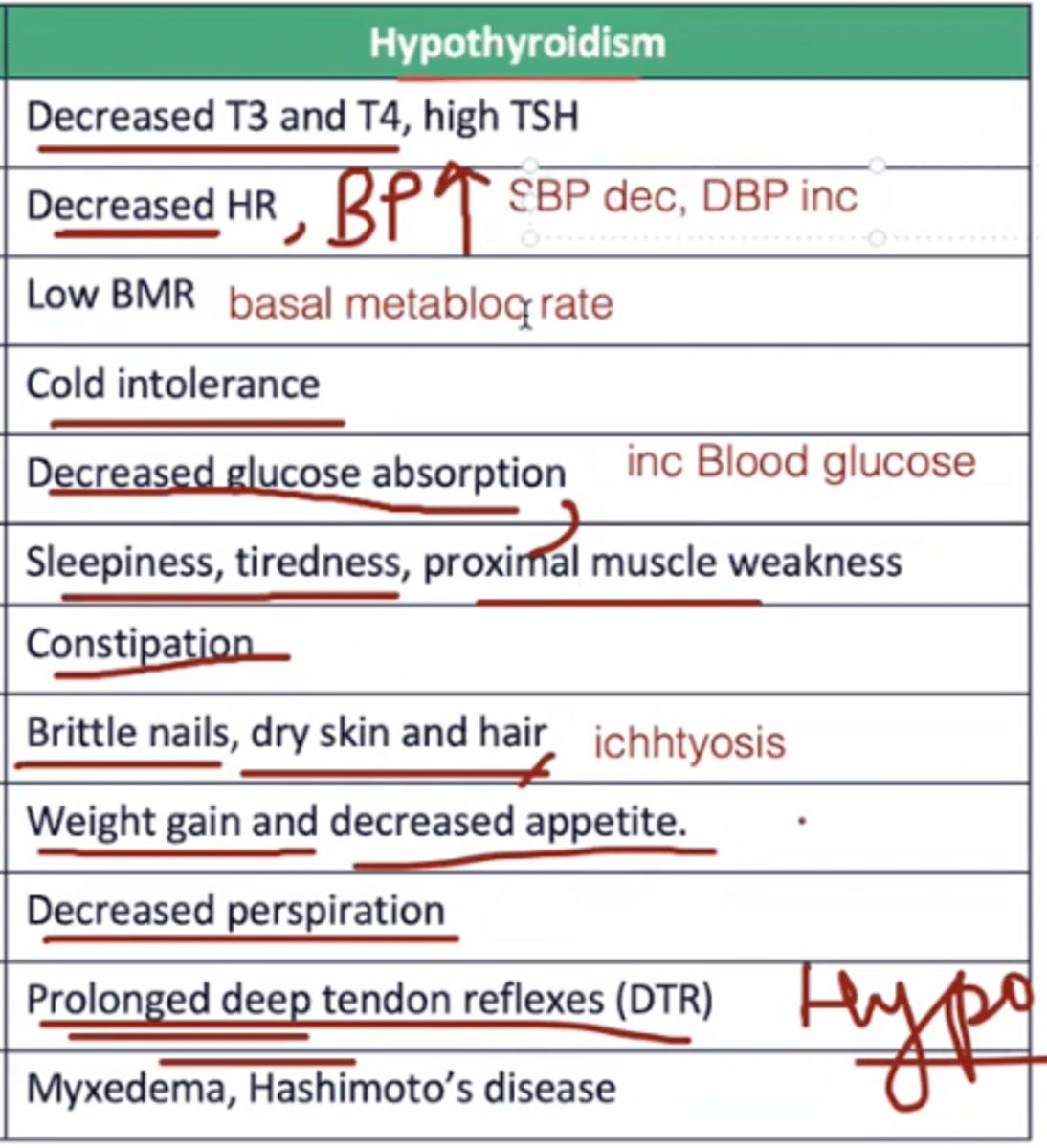
Hypothyroidism
myxedema (puffiness and swelling in hands, feet, and face BAD), hashimotos
lazy person laying on the couch all day in sidelying
When are goiters usually seen?
hyperthyroidism (deficiency of iodine)
Hyperparathyroidism vs hypoparaythyroidism
directly related to calcium and inversely related to phosphate
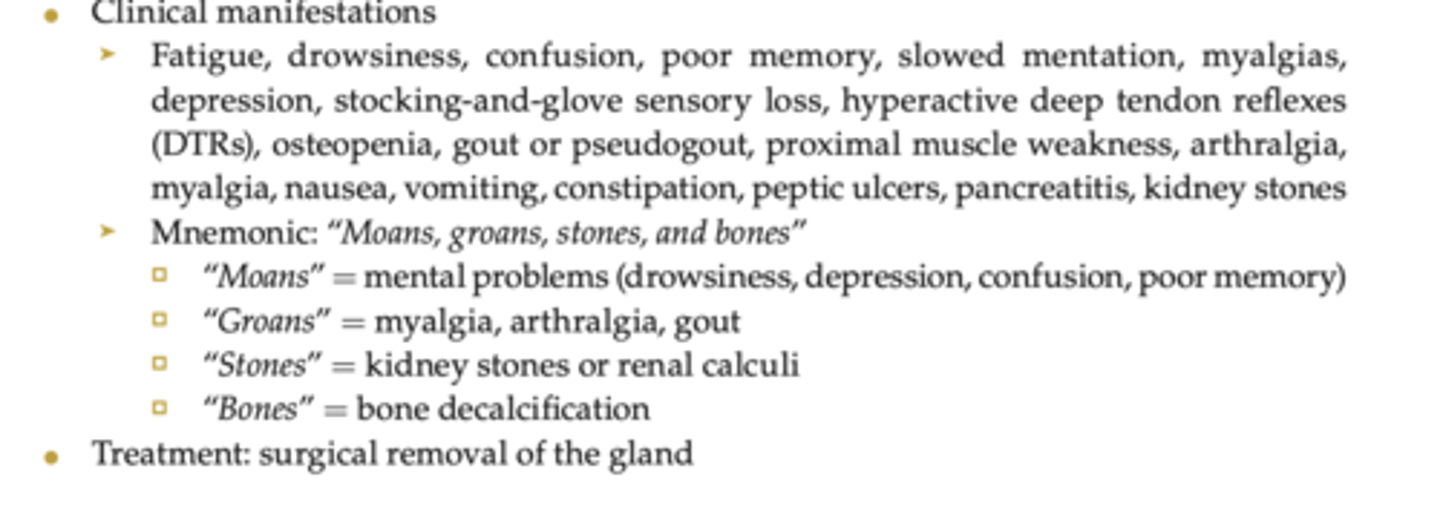
-hyperparathyroidism: bones, stones, groans, moans, sensory
-hypoparathyroidism: analogy - cats are numb (trosseau sign is carpopedal spasm; chovsteak is tingling numbness in the facial nerve)
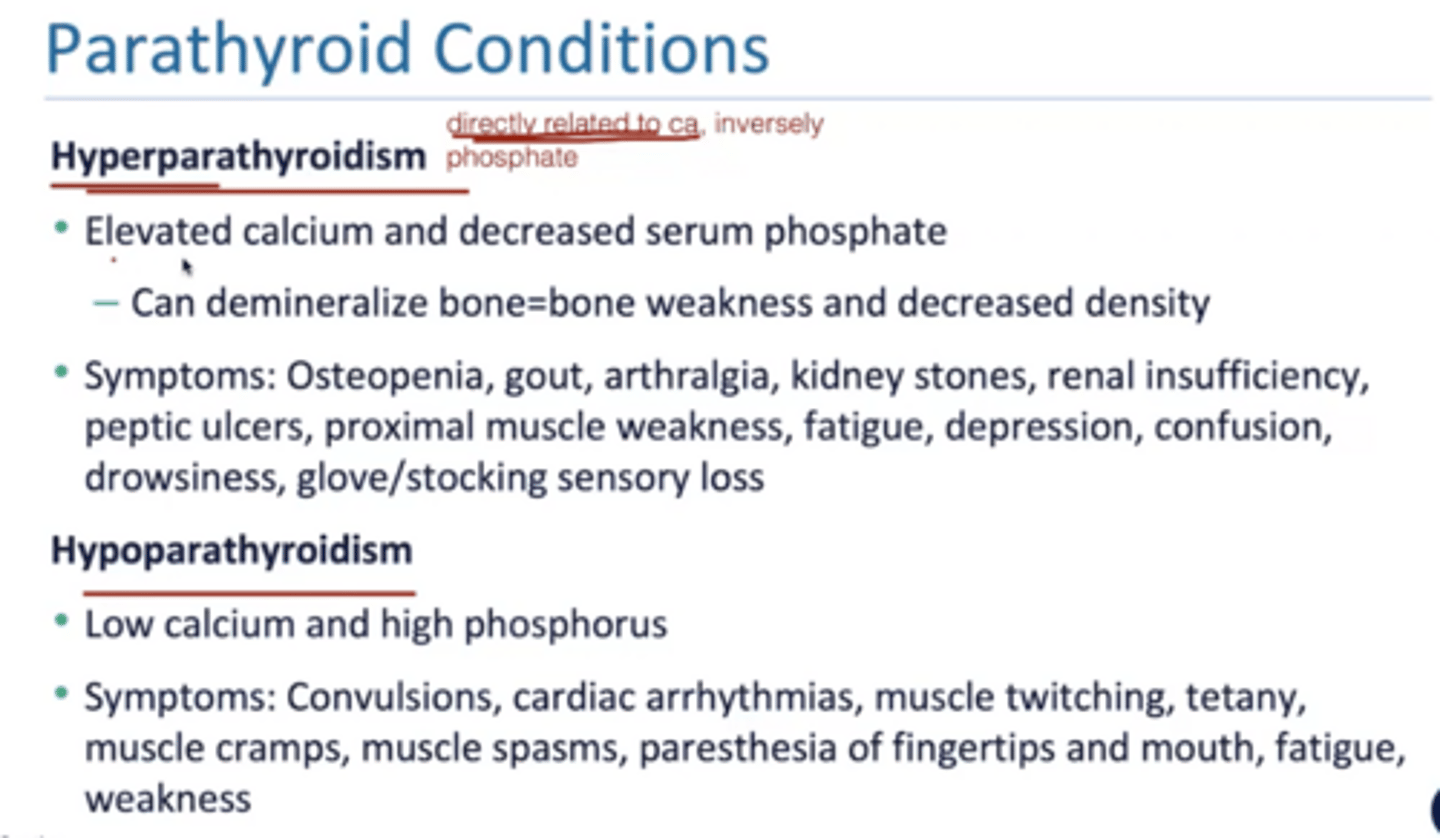
Hyperparathyroidism bones, stones, groans, moans, sensory
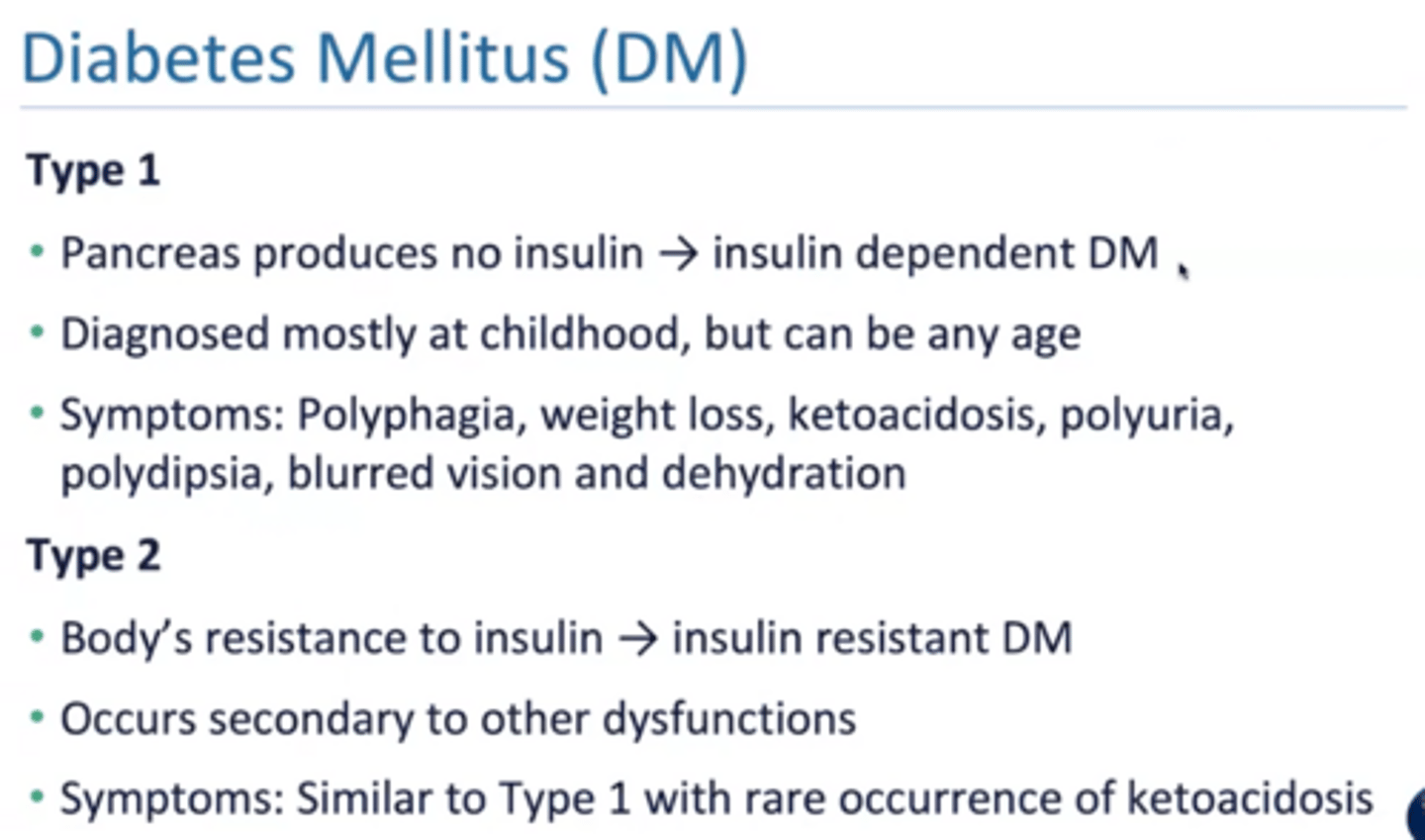
Type 1 vs type 2 diabetes
type 1: insulin dependent
type 2: insulin resistant
(ketoacidosis is fruity odor breath and is emergency!!)
Secondary diabetes
associated with other conditions
➤ Pancreatic disease or removal of pancreatic tissue
➤ Endocrine disease: acromegaly, Cushing syndrome
➤ Drugs: some diuretics, glucocorticoids, levodopa
➤ Chemical agents
Gestational diabetes
high blood sugar during third trimester of pregnancy
Prediabetes
impaired glucose tolerance (IGT) with abnormal response to oral glucose
Kussmaul breathing
sign of diabetic ketoacidosis (DKA)
S/S of diabetes
● Hyperglycemia: elevated blood sugar (fasting glucose level of > 126 mg/dL)
● Glycosuria: elevated glucose level in urine
● Polyuria: excessive urination
● Polydipsia: excessive thirst
● Polyphagia: excessive hunger
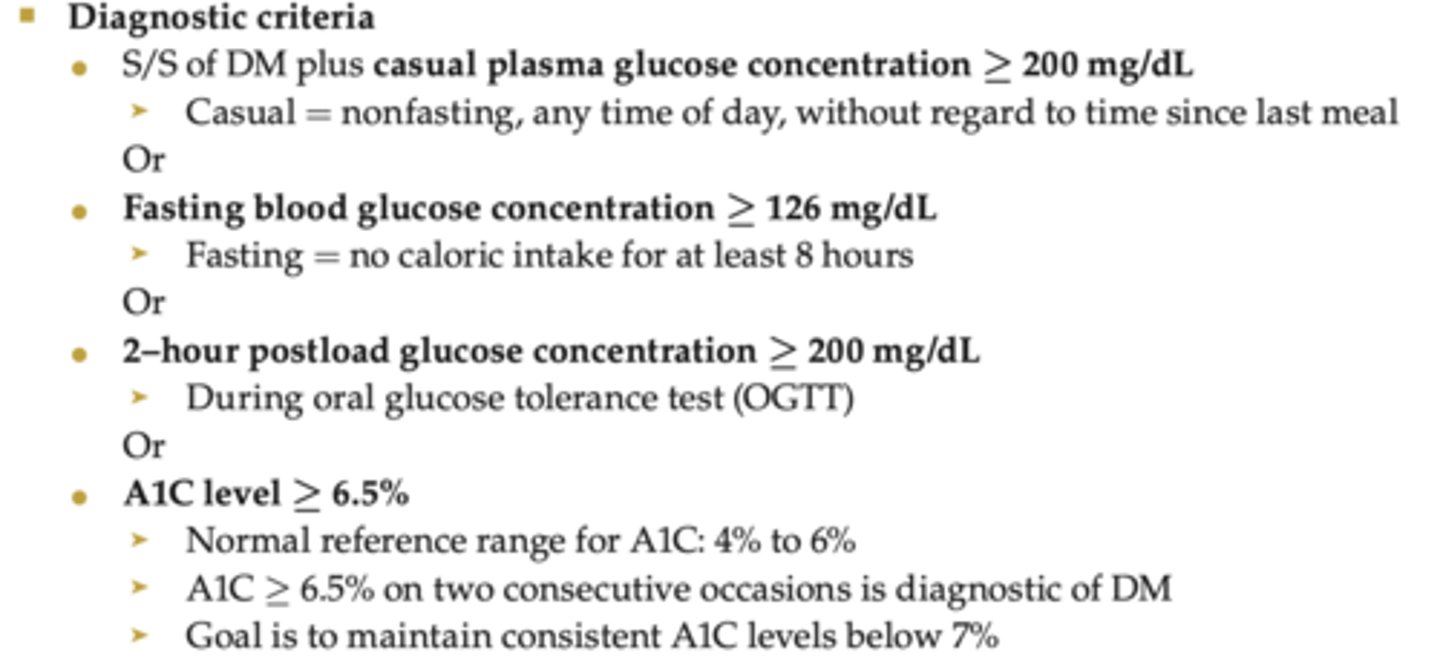
● Glycated hemoglobin (A1C) level: ≥ 6.5%
● Ketonuria
● Unexplained weight loss
● Fatigue and weakness
● Irritability
● Blurred vision
● Recurring skin, gum, bladder, vaginal, or other infections
● Numbness or tingling in hands and feet
● Cuts and bruises heal with difficulty
Complications of diabetes
- microvascular disease (retinopathy, diabetic neuropathy, peripheral neuropathy)
- macrovascular disease (heart, brain and lower extremity arteries are effected), atherosclerosis, coronary artery disease, peripheral vascular disease
- integumentary impairments (degenerative changes in connective tissues, skin infections)
- musculoskeletal impairments (adhesive capsulitis, hand stiffness)
- neuromuscular impairments (diabetic polyneuropathy)
- diabetic autonomic neuropathy
- kidney failure
-vision impairments
- fatty liver disease
Diabetes diagnostic criteria
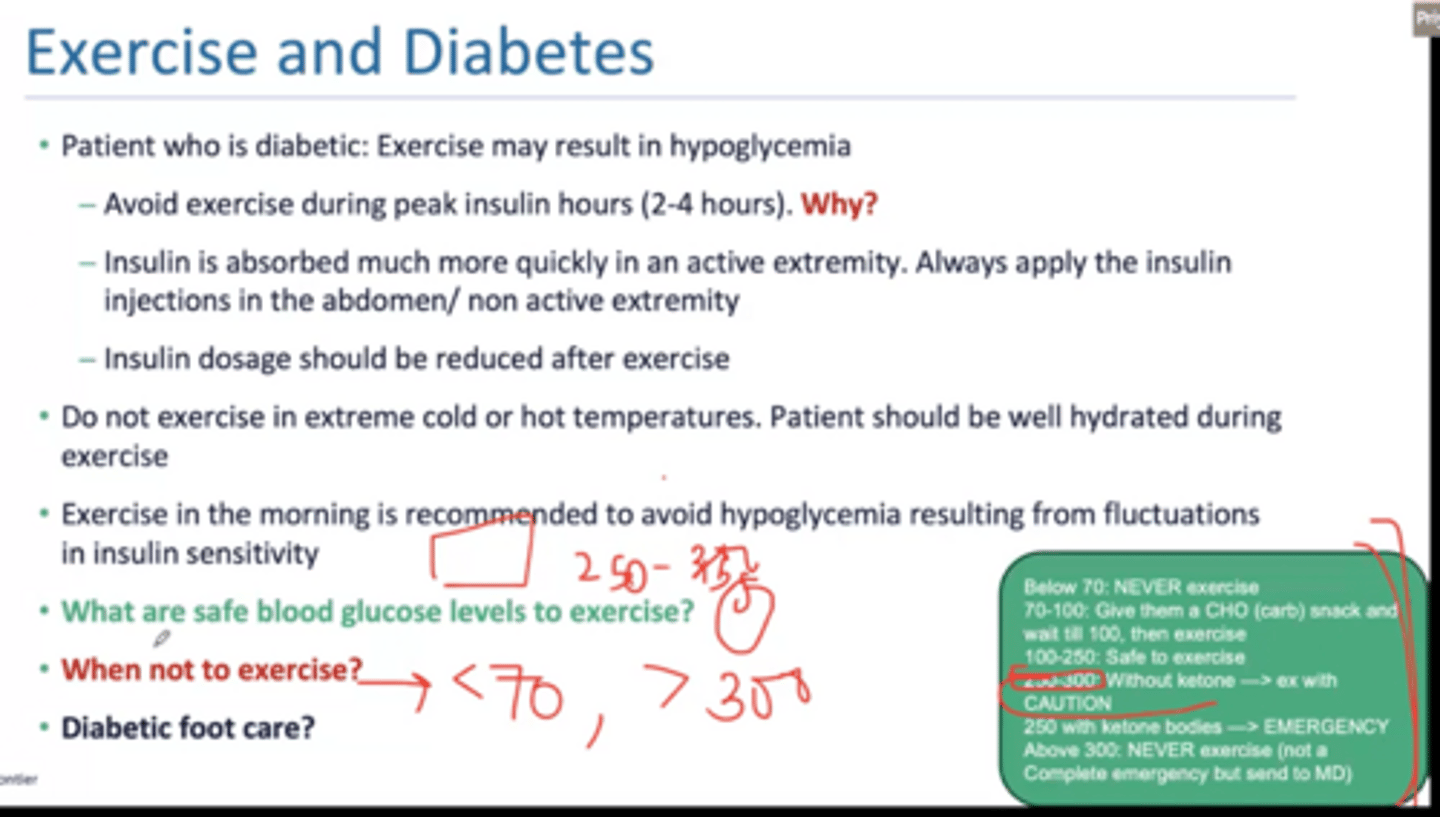
Post exercise hypoglycemia may last as long as ___ hours
12
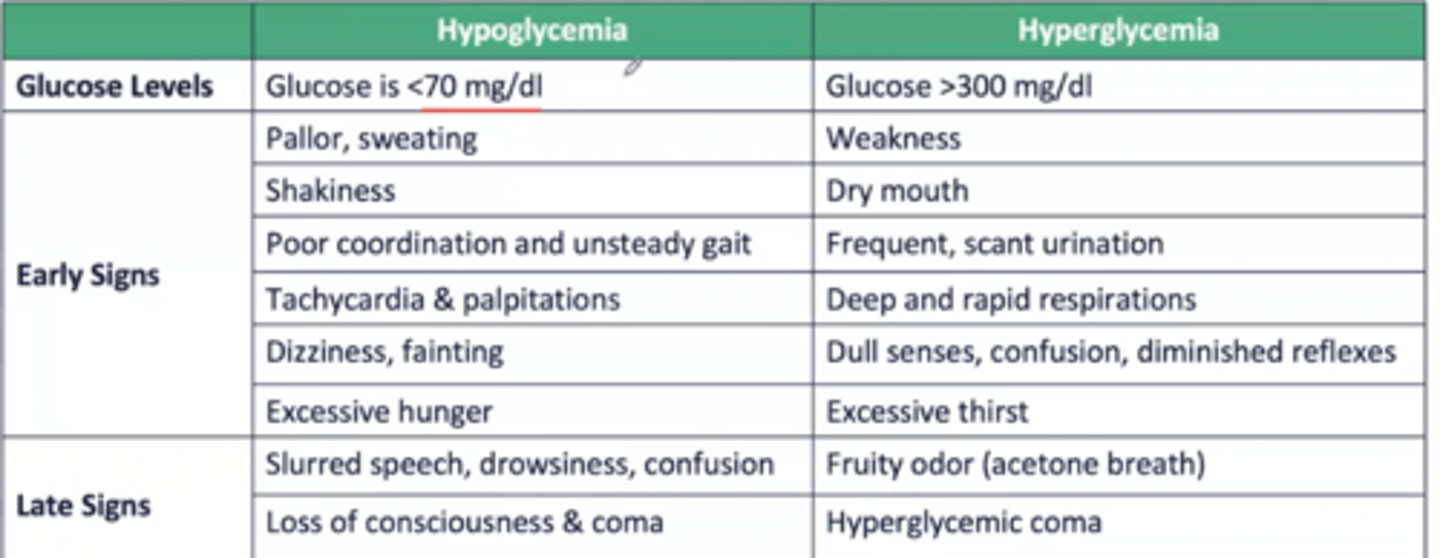
Signs and symptoms of hypoglycemia and hyperglycemia
Sympathetic cardiovascular changes in patients with long standing type 1 diabetes
heart rate becomes fixed
Fasting blood glucose vs random blood glucose level vs HbA1C diagnosis of DM
fasting: >126 mg/dL
random blood glucose level: > 200 mg/dL
HbA1C: >10 is immediate insulin therapy and 4-6% is normal; 3 month average of amount of glucose that is attached to your hb
Hypoglycemia vs hyperglycemia
hypoglycemia:
Tachy
Irritable
Restless
Excessive hunger
Dizziness
cold and clammy give them a candy
hyperglycemia: hot and cry sugar high
How does exercise impact diabetes/when can you exercise?
NO exercise: <70 or >300
safe is 100-250
Diabetic foot care
-foot should undergo screening
-wash (do not soak) feet daily in warm water
-toe nails cut
-clean white socks without wrinkles
-alternate shoes
-snug fit with laces or velcro
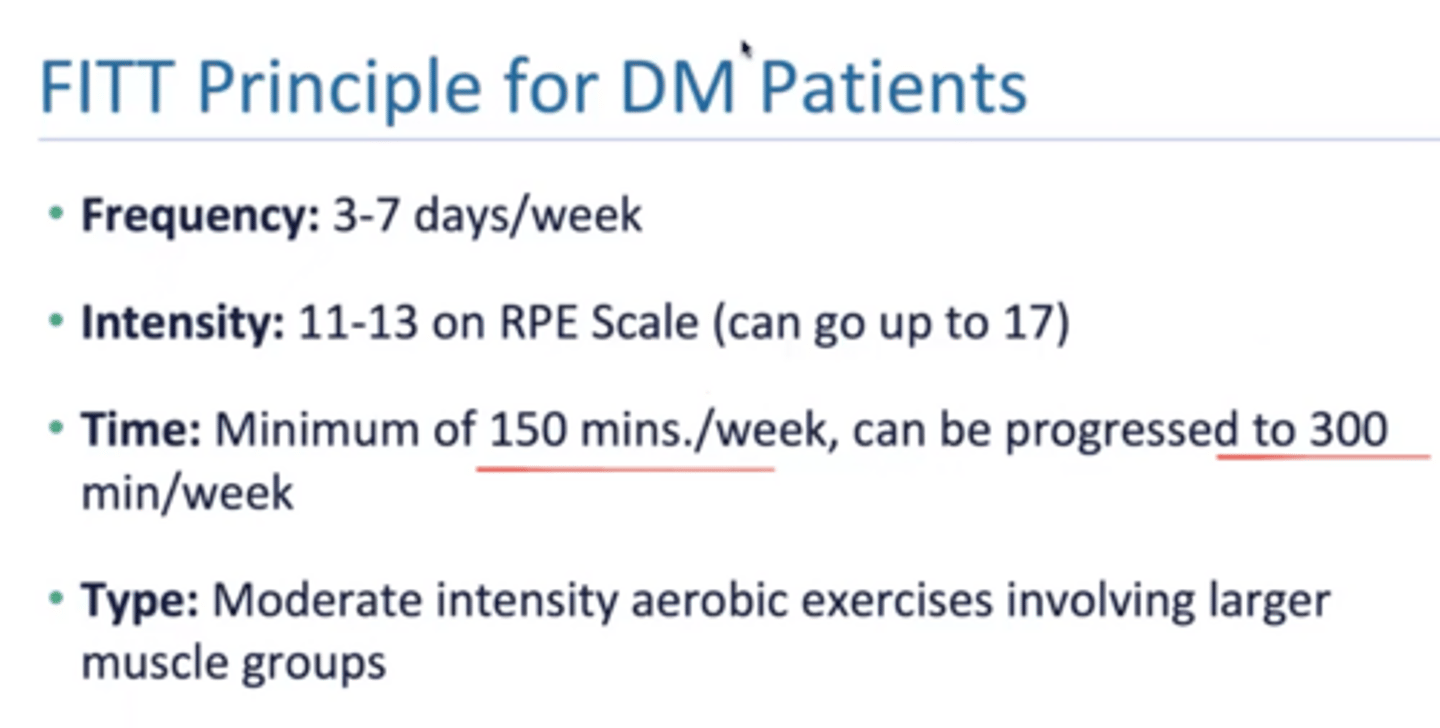
DM FITT principles
Lateral wall of the pelvic cavity is formed by _______________ and ___________
piriformis and obturator internus
What makes up the pelvic diaphragm (primary muscular support)
What is the perfect scheme?
a method of examination of the pelvic floor muscles that looks at
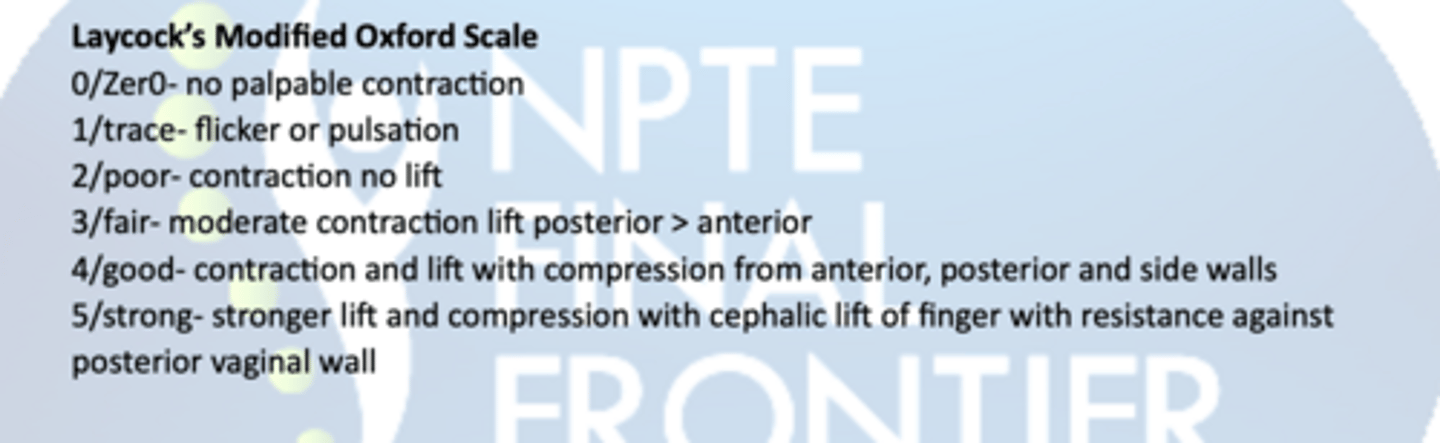
Power - Modified Oxford Scale
Endurance - How long can they hold a maximal voluntary contraction (up to 10sec)
Repetitions - How many maximal voluntary contractions they hold with a rest between them, up
to 10 reps (eg 10 repetitions of a 10-second hold)
Fast- The number of 1-second maximal voluntary contractions they can perform in a row (up to
10)
Every Contraction Timed - a reminder to time every contraction
Stress incontinence
involuntary leakage of urine during couch, sneezing or exertion;
-can be seen in postpartum, pelvic floor muscle weakness (levator ani muscles which are puboccygeus, ilioccygeus, pubo rectalis)
tx: strengthen pelvic floor muscles
Urge incontinence
involuntary contraction the detrusor muscle with a strong desire to void (urgency)
-can be seen with infections, parkinsons, UMN lesions
tx: treat infections and voiding schedule
Overflow incontinence
incontinence caused by an acontractile or underactive detrusor muscle; bladder is overdistended, can not empty completely and urine dribbles or leaks out
-can be seen with benign prostatic hyperplasia, DM
tx: behavioral modification like double voiding, medication and catherization
Functional incontinence
incontinence due to mobility, dexterity, or cognitive deficits
-can be seen with dementia, lower extremity weakness
tx: clear clutter, improve accessibility, and prompted voiding
Changes with pregnancy weight gain and MSK system postural changes
-25 to 35 lbs essential for baby's nourishment
-postural changes: forward head, kyphosis, increased lordosis, anterior pelvic tilt
-postural stress continues even postpartum due to lifting and carrying of baby
Blood pressure and heart rate changes in pregnancy and positional consideration
-blood pressure is low in first and second trimester increases in last trimester (CO increases)
-resting heart rate increases by 10-20 bpm (heart rate will not proportionally increase with exercise, max heart rate)
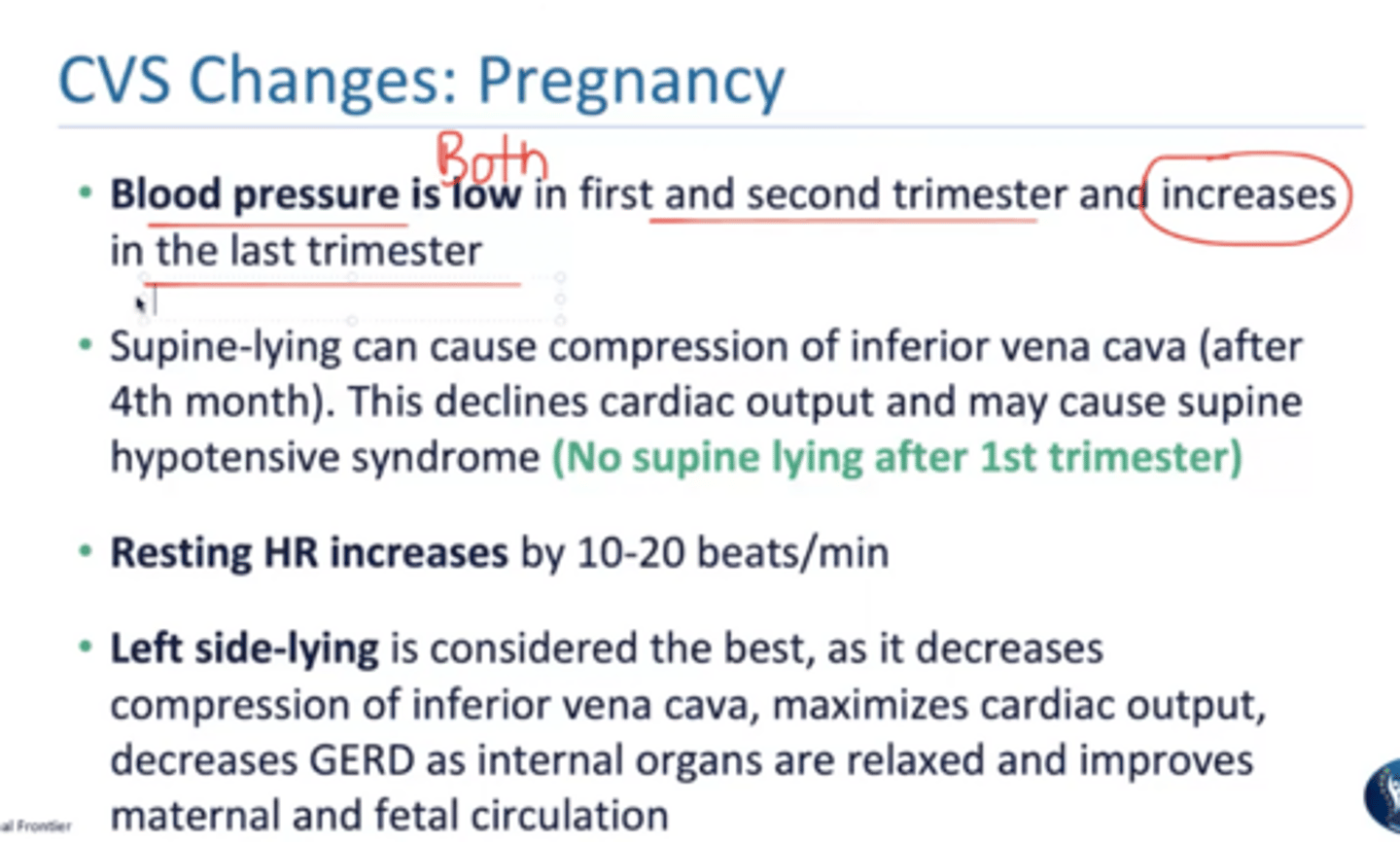
Lay on your ______ side when pregnant
left
_________ incontinence is most common during pregnancy
stress (80% of the time)
Respiratory changes during pregnancy
➤ Depth of respiration increases
➤ Tidal volume and minute ventilation increase, whereas total lung capacity is unchanged or decreases slightly
➤ Natural state of hyperventilation exists during pregnancy to meet the increased oxygen demands during pregnancy
➤ Diaphragm is elevated and thoracic cage widens → hyperventilation, with mild exercise
Metabolic changes during pregnancy
➤ Increased basal metabolic rate and heat production
➤ Lower fasting blood glucose levels
➤ Body requires an additional 300 kcal per day to maintain homeostasis
➤ Stroke volume (SV) and CO increase with exercise
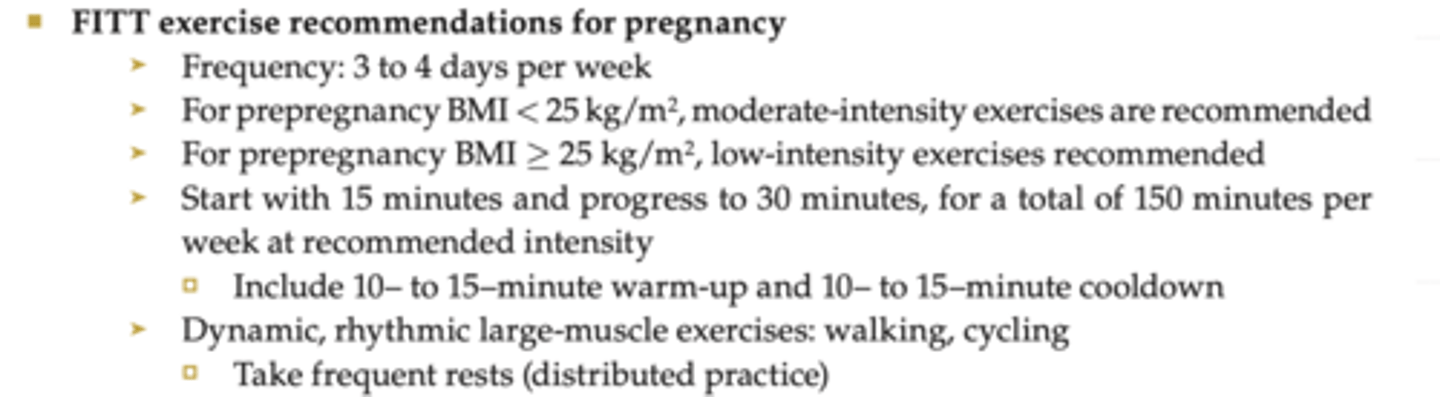
FITT for pregnancy
➤ Postural education and exercises
Stretch and strengthen appropriate muscles
➤ Pelvic stabilization exercises
➤ Pelvic floor muscle exercises
➤ Focus on strengthening trunk flexors, hip extensors, and pelvic floor muscle
➤ Ankle pumps for late-stage pregnancy; elevate legs to assist in venous return
➤ Progress from gravity-assisted to standing positions as strength and awareness increase
Postcesarean 1-3 days post vs later exercises
● 1 to 3 days post: breathing exercises, coughing or huffing to loosen phlegm, and pelvic floor exercises
● Later: gentle partial sit-ups and head lifts, low-intensity aerobic exercises, pelvic tilts in quadruped position
Premature rupture of membranes
anmoitic sac breaks and amniotic fluid is lost before the onset of labor (requires immediate medical attention)
Incompetent cervix
painless dilation of cervix in 2nd trimester (after 16 weeks gestation) or early 3rd trimester
- May use stitches to keep cervix closed (cerclage)
- Without timely intervention, may lead to continued dilation of the cervix → rupture of membranes → delivery of fetus
Placenta previa
placenta attaches too low on the uterus → as the cervix dilates, the placenta begins to separate from the uterus and may present before the fetus
- Life threatening to the fetus
- Bleeding is the primary symptom
Contraindications for pregnancy
-prolonged periods of motionless standing
-avoid valsalva
Absolute contraindications
-Preeclampsia
-severe anemia
-restrictive lung disease
-type 1 diabetes
Precautions to observe for during pregnancy
● Vaginal bleeding
● Persistent pain: chest, pelvic girdle, low back
● Leakage of amniotic fluid
● Painful contractions that persist beyond exercise session
● Shortness of breath
● Tachycardia
● Headache, dizziness
● Swelling and/or pain in calf
Premature onset of labor is before
37 weeks
Preterm rupture of membranes
amniotic sac breaks and amniotic fluid is lost
before the onset of labor; Requires immediate medical attention
Incompetent cervix
painless dilation of cervix in 2nd trimester (after 16 weeks'
gestation) or early 3rd trimester
May use stitches to keep cervix closed (cerclage)
Without timely intervention, may lead to continued dilation of the cervix → rupture of membranes → delivery of fetus
Placenta previa
placenta attaches too low on the uterus → as the cervix dilates,
the placenta begins to separate from the uterus and may present before the fetus
-life threatening to fetus
-bleeding is primary symptom
Preeclampsia
starts in 3rd trimester and disappears postpartum
- Pregnancy-induced acute HTN
- BP > 140/90 (measured 2 times within 4 h) → medical emergency
- S/S: HTN, protein in urine, severe fluid retention
- Complications: maternal convulsions, coma, and death
Ectopic pregnancy
tubal pregnancy
-Fertilized egg is implanted outside the uterine cavity (mainly in the fallopian tube)
-Medical emergency
S/S
⚬ Sudden onset of sharp pain on one side of the lower abdomen or pelvis
lasting more than a few hours
⚬ Referred pain to shoulder
⚬ Amenorrhea, irregular bleeding, and spotting
⚬ Dizziness, fainting, paleness, and shock
-Treatment: pain management, surgery
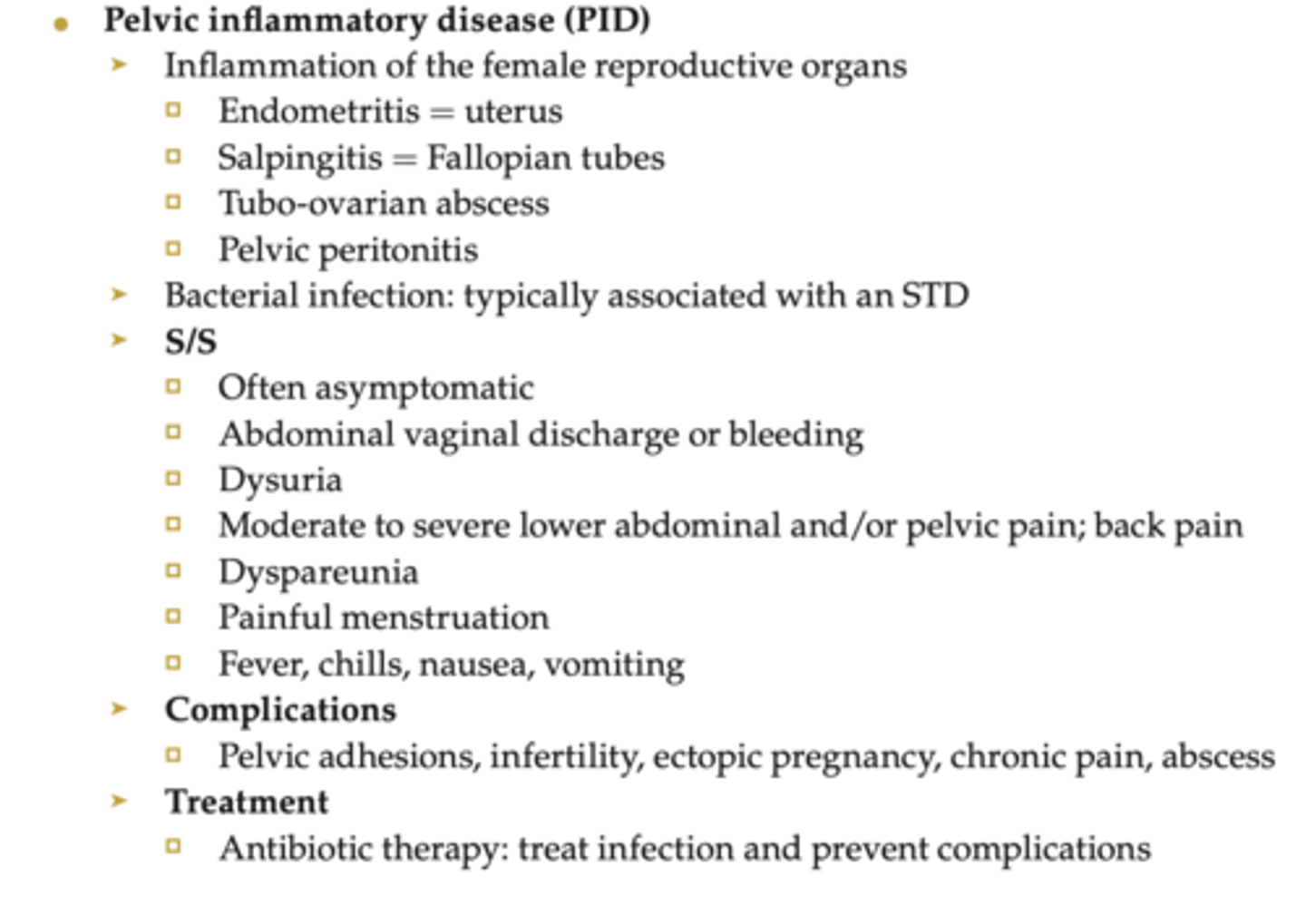
Pelvic inflammatory disease
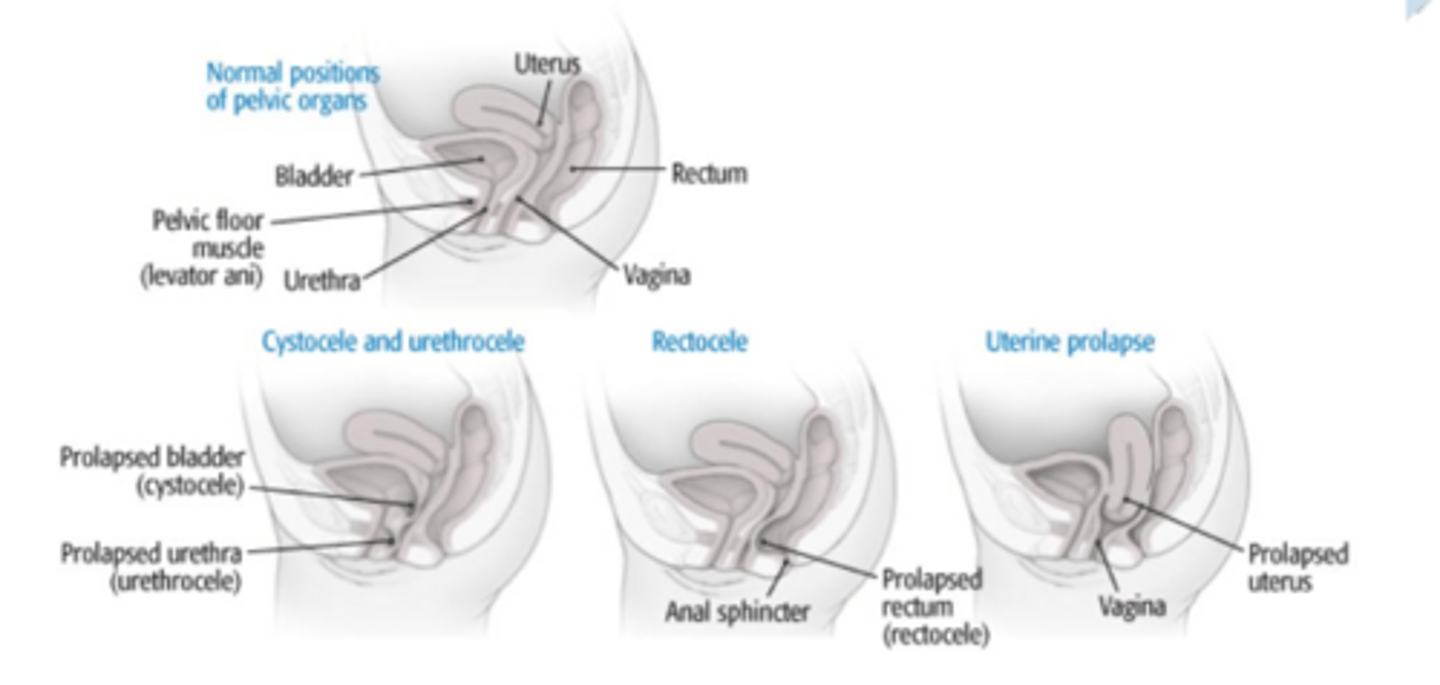
Cystocele vs rectocele vs uterine prolapse
Uterine Prolapse- bulging uterus into the vagina
Signs & symptoms:
• Pelvic pressure, perineal heaviness, backache
• Symptoms relieved by lying down
• Symptoms made worse by prolonged standing, walking, coughing, or straining
Cystocele Prolapse- herniation of bladder into the vagina
Signs & symptoms:
• Urinary frequency and urgency
• In advanced stages, difficulty emptying the bladder
• Cystitis (bladder infection)
• Bulge or pressure sensation in the perineal area
• Urinary incontinence
Rectocele Prolapse- herniation of rectum into the vagina
Signs & symptoms:
• Perineal pressure and bulge
• Straining to defecate
• Feeling of incomplete rectal emptying
• Constipation
Pelvic floor prolapse treatment
• Kegel's exercise -Start in lying (gravity elimination position) and progress to upright postures,
sitting, and standing while performing activities. This improves control of the pelvic muscles and
helps in treating incontinence. Examples are gravity assisted (Inverted hook lying), gravity
eliminated (supine, prone, side-lying), resisted (standing, lunges, squat)
• Vaginal weight training (using vaginal cones)
• Biofeedback, postural reeducation, pelvic mobilization
• Electrical stimulation
• Teach splinted coughing, and huffing as a patient will not be able to bear down
Coccydynia
pain in region of coccyx
-joint becomes hypermobile and causes coccyx pain
-causes: trauma, events associated with childbirth
Sacroiliaic joint dysfunction
➤ Due to postural changes, ligament laxity
➤ Pain in the posterior pelvis and buttock that may radiate into the posterior thigh and knee
Nerve supply to pelvic floor
pudenal nerve
Precalmpsia
-pregnancy induced acute hypertension after the 20th week of gestation
-increase in protein in urine, hyperreflexia, edema, headache, sudden weight gain
-a blood pressure more than 140/90 mmHg; second abnormal BP reading four hours after the first confirms the diagnosis
EMERGENCY!
Eclampsia
after birth and has seizures due to high BP after childbirth, headache and visual disturbances (preclampsia does not have seizures!)
Multiple gestation
more than 1 fetus
Contraindications to exercise for pregnant women
*uncontrolled maternal type I diabetes or any of these that are currently symptomatic
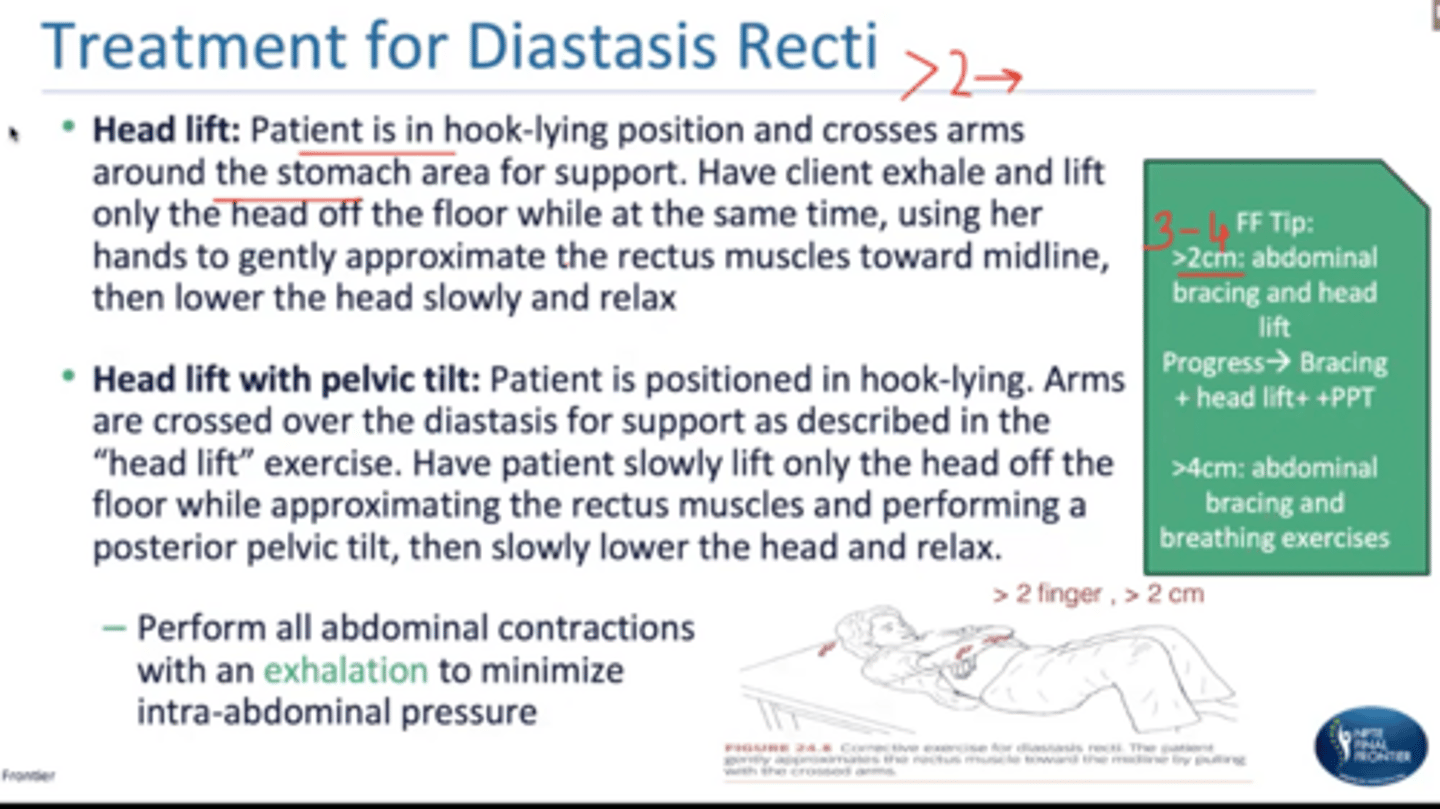
Treatment for diastasis recti and how much is considered diastasis recti
>2 cm (don't do any aggressive...avoid curl ups, leg lifts, fire hydrants)
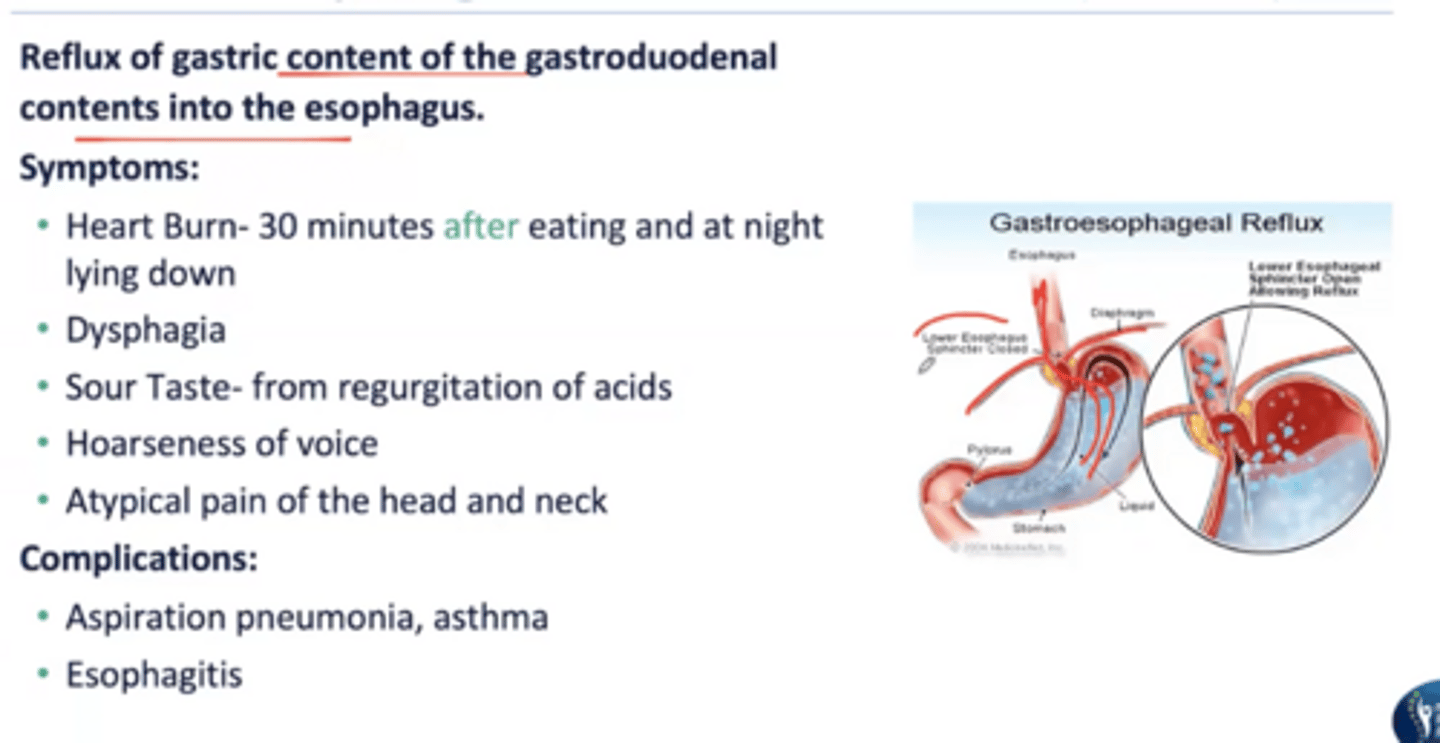
Gerd symptoms and complications
problem with the lower esophageal sphincter; reflux of gastric content of the gastroduodenal contents into the esophagus
GERD treatment
-maintain upright positions
-eat meals at least 3-4 hours before sleep
-avoid supine b/c tends to straighten the esophagus
-sleep on left side preventing nocturnal reflex
-exercise must be completed 2-3 hours after eating or before meals
-avoid spicy, chocolate, fatty food, peppermint
-drugs: antacids, H2 receptor blockers, proton pump inhibitors