N/V/C/D Pharmacotherapy
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
What are some GI/Intraperitoneal causes of N/V?
- Obstruction
- Infection
- Pancreatitis
- IBD/IBS
- Hepatitis
- Gastroparesis
- GERD
- PUD
What are some cardiac causes of N/V?
- Myocardial infarction
- Heart failure
What are some neurologic causes of N/V?
- Motion sickness
- Migraine
- Increased intracranial pressure)
- Meningitis
What are some common drugs/toxins that can cause N/V?
- Antibiotics
- Chemotherapy
- Digoxin
- Ethanol
- Opioids
What are some metabolic/endocrine causes of N/V?
- Pregnancy
- DKA
- Hyperthyroidism
How is "simple" N/V characterized based on symptoms, signs, and tests?
- Mild distress
- Self-limiting
- Resolves spontaneously
- Symptomatic therapy
- Queasiness/discomfort
- No tests needed
How is "complex" N/V characterized based on symptoms, signs, and tests?
- Severe distress
- Not relieved after antiemetics
- Progressive deterioration due to fluid-electrolyte imbalances
- Weight loss, fever, abdominal pain
- Test serum electrolytes, upper/lower GI evaluation
What are the 5 steps to N/V treatment?
1. Define what patient means by N/V
2. Determine whether N/V is acute or chronic
3. Consider medication or toxin side effects
4. Use findings to formulate a diagnosis to guide treatment
5. Direct treatment based on NT and receptors involved in central/peripheral emetic pathways
What are the "go-to" options for uncomplicated reflux/heartburn-associated N/V?
- Antacids
- H2RAs
- Consider short OTC PPI
What is some key monitoring/counseling for uncomplicated reflux/heartburn-associated N/V?
- In CKD, caution with Mg/Al
- Diarrhea/constipation
- Counsel on dosing separation
What are the "go-to" options for vestibular/motion sickness/vertigo?
- Meclizine
- Dimenhydrinate
- Scopolamine patch if prolonged or can't take PO
What is some key monitoring/counseling for vestibular/motion sickness/vertigo?
- Sedation/anticholinergic effects
- Apply patch hours before motion
- Avoid with narrow-angle glaucoma/urinary retention
What are the "go-to" options for gastroparesis-associated N/V?
Metoclopramide (short-term)
What is some key monitoring/counseling for gastroparesis-associated N/V?
- EPS/tardive dyskinesia risk
- Avoid prolonged use
- Monitor restlessness
- Dystonia
- Counsel on timing before meals
What are the "go-to" options for PONV prophylaxis/rescue?
Risk-based multimodal prophylaxis/rescue. Different class if <6hr since prophylaxis
What is some key monitoring/counseling for PONV prophylaxis/rescue?
- QT prolongation (5-HT3, butyrophenones)
- Avoid repeating same class within 6 hours
What are the "go-to" options for pregnancy N/V?
- First line: pyridoxine +/- doxylamine
- Adjunct: antihistamines/phenothiazines
- Refractory: metoclopramide/ondansetron
What is some key monitoring/counseling for pregnancy N/V?
- Balance fetal safety + severity
- Sedation risk
- Counsel hydration
- Refer if unable to keep fluids down
What are some non-pharmacologic options for N/V?
- Dietary changes
- Relaxation
- Biofeedback
- Hypnosis
- Cognitive distraction
- Guided imagery
- Acupuncture
PONV stands for:
Post-Operative Nausea and Vomiting
What are some PONV patient-related risk factors?
- Age < 50
- Female sex (2-3x more likely)
- Nonsmoker
- History of PONV or motion sickness
- Hydration status
What are some PONV anesthesia-related risk factors?
- Use of general anesthesia
- Use of volatile anesthetics (halothane, isoflurane, desflurane, sevoflurane)
- Nitrous oxide
- Use of opioids
What are some PONV surgery-related risk factors?
- Type of procedure (laparoscopic, GYN, cholecystectomy)
- Duration of surgery
When is multimodal prophylactic medication recommended for PONV?
In patients with 1+ risk factors
What should be given for emesis within 6 hours of surgery?
Rescue therapy from a different class
What should be given for emesis >6 hours of surgery?
Any drug used for prophylaxis can be used except dexamethasone and transdermal scopalamine
When must ondansetron be given for PONV prophylaxis?
At the end of surgery
When must dexamethasone be given for PONV prophylaxis?
At induction
N/V can progress to _____________ in 0.3-3% of pregnancies
hyperemesis gravidarum
How is hyperemesis gravidarum treated in pregnancy?
- May require enteral/parenteral nutrition
- Corticosteroids (methylprednisolone)
What is the first-line treatment for pregnancy induced N/V?
- Pyridoxine (B6) 10-25 mg +/- antihistamine (doxylamine)
- Brand names include Diclegis and Bonjesta
What are 4 adjunct therapies for pregnancy induced N/V?
1. Promethazine 12.5-25 mg PO/IM/PR q4-6hr
2. Prochlorperazine 25 mg PR q12hr
3. Dimenhydrinate 25-50 mg PO q4-6hr (max 200 mg/day with doxylamine)
4. Diphenhydramine 25-50 mg PO q4-6hr
What are 3 refractory therapies for pregnancy induced N/V?
1. Promethazine 12.5-25 mg PO/IM/PR q4-6hr
2. Metoclopramide 5-10 mg IM/PO q6-8hr
3. Ondansetron 4-8 mg ODT PO q6-8hr
What is the most reliable pharmacotherapy for N/V due to balance disorders?
Antihistamine-anticholinergic agents
What is first line for motion sickness when unable to take oral or prolonged effect is needed?
Scopolamine patch
What are some common side effects of the scopolamine patch?
- Drowsiness
- Decreased mental acuity
- Visual disturbances
- Dry mouth
- Urinary retention
What are some common medication causes for acute diarrhea?
- Antibiotics
- Hydralazine
- Metformin
- Sorbitol
- Colchicine
- Laxatives
- Misoprostol
- Theophylline
- Digitalis
- Mannitol
- Quinidine
- Thyroid products
What are some common dietary supplements causes for acute diarrhea?
- St. John's wort
- Echinacea
- Ginseng
- Aloe vera
What are some common poison causes for acute diarrhea?
- Arsenic
- Cadmium
- Mercury
- Monosodium glutamate
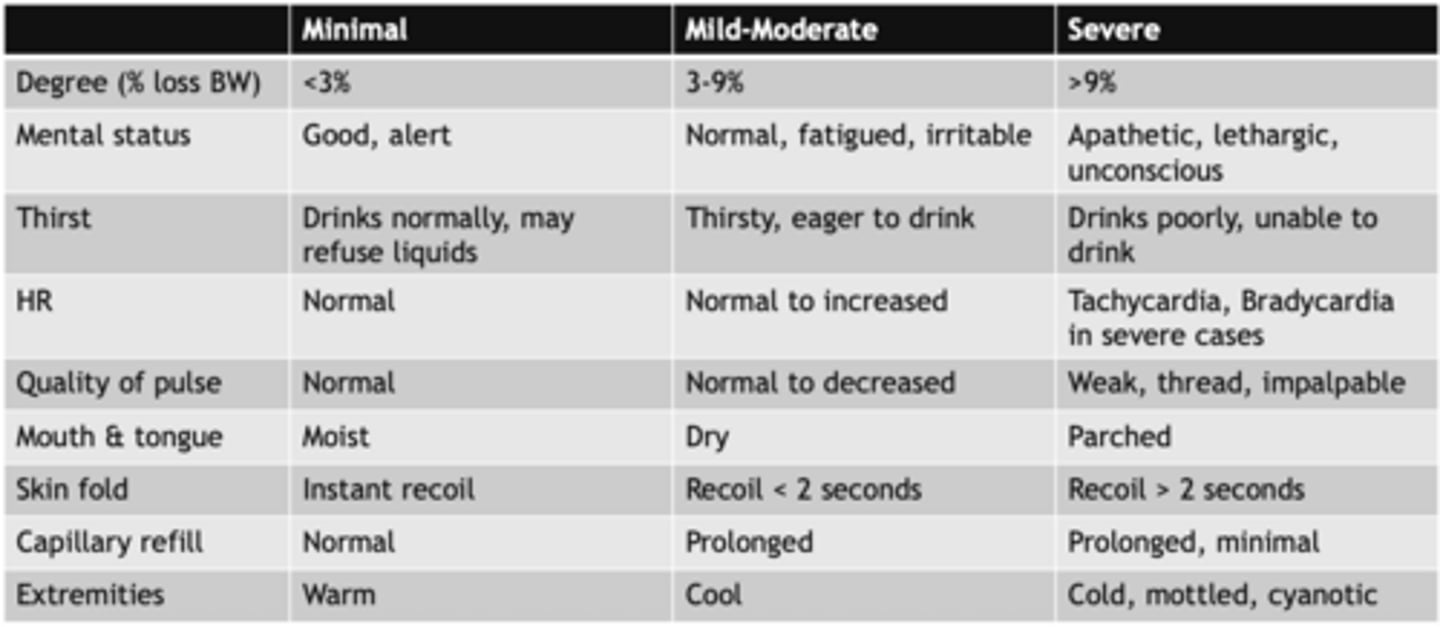
Severity of acute diarrhea is assessed by...
degree of dehydration
What are some signs that a patient would need a referral or urgent treatment for diarrhea?
- Blood/mucus in stool
- High fever
- Severe abdominal pain
- Immunocompromised
- Recent antibiotics/hospitalization
- Signs of moderate-severe dehydration
If there are no red flags and the patient has mild diarrhea, what can be used for treatment?
Self-care, continue diet as tolerated and use a oral rehydration solution
What is used for symptom relief in acute diarrhea?
Loperamide for non-bloody, afebrile diarrhea
Bismuth for mild traveler's/food-borne symptoms
What are some safety pearls for acute diarrhea?
- Avoid antimotility agents if suspected invasive diarrhea (blood/fever) or C.diff concern
- Escalate if symptoms persist >48 hr of worsening dehydration
What are some common drugs that cause constipation?
- Opioids
- Verapamil
- Diuretics
- GLP-1s
What information is important to collect when assessing constipation?
- Frequency of bowel movements
- Duration of symptoms
- Usual diet
- Laxative regimens
- Current medications
- Psychiatric history
- Physical exam (rectal)
What are some non-pharm management options for constipation?
- Dietary modification (increase fiber to 20-25 g/day)
- Surgery (only if malignancy or obstruction)
- Biofeedback (idiopathic constipation due to pelvic flood dysfunction)
What are the 6 steps to constipation pharmacotherapy?
1. Rule out red flags
2. Address contributing factors (med induced, low fiber/fluids, low activity)
3. First-line meds = osmotic laxative +/- short trial of bulk-forming
4. Add ons = stimulant for inadequate response
5. Rescue = rectal therapy (supp/emena) or referral if refractory/complicated
6. Monitoring/counseling: stool frequency/consistency goals, cramping/diarrhea, electrolyte concerns in high-risk patients, when to reassess
What are some constipation red flags that might be cause for referral?
- Severe pain
- Vomiting
- Obstruction symptoms
- Weight loss
- GI bleeding
Why do butyrophenones (haloperidol/droperidol) have limited use despite being very effective?
Propensity to cause extra-pyramidal symptoms and risk of QTc prolongation
What is the standard of care for CINV, PONV, and radiation induced N/V?
5-HT3 antagonists
What is useful in diabetic gastroparesis associated with N/V?
metoclopramide