Voice Exam 1
1/79
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
80 Terms
Voice Evaluation- perception
1) GRBAS (G = Grade or overall severity of dysphonia, R = Roughness, B = Breathiness, A = Aesthenia, and S = Strain voice quality)
2) CAPE-V (couple lines 1 out 100, listener rates)
Voice Evaluation
-Acoustics (objective but limited) (PRAAT)
-Aerodynamics
-Imaging (stroboscopic or endoscopic)
-Patient self-report
Objective Acoustic Measures
-Pitch
-Loudness
-Quality-related measures (jitter, shimmer, HNR, CPP)
Acoustic Pitch Measures
• Frequency range- lowest to highest note
•Task: Pitch glide, lowest and highest frequency excluding fry
•Mean Frequency in conversation- able to put in note if it’s abnormal
Acoustic Loudness Measures
dB range
dB in conversation
Acoustic quality-related measures
•Sustained phonation (ahhhhh) tasks: jitter and shimmer (perturbation), Harmonics to Noise ratio
•Sustained phonation AND connected speech: Cepstral Peak Prominence
Fundamental Frequency
How many flaps/cycle per second
Ex: 100 flaps/sec. = Pitch Period is .1
•F0= fundamental frequency – lowest frequency- perceived pitch
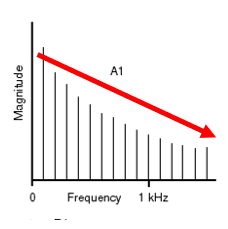
•Higher Fo has wider-spaced harmonics
•Higher harmonics have less energy:
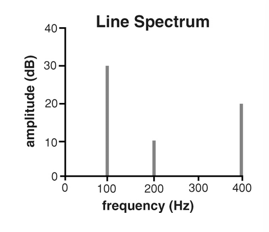
Harmonics
•multiples of fundamental frequency
•So: 100 Hz wave also has 200 Hz, 300 Hz, 400 Hz, etc.
•We perceive the 100 Hz distance between them as F0
Spectral Slope
Graph sloping downward
Amplitude or dB
How wide the flap is or the displacement of vocal folds
•Determined by Psub
•Height of waveform
Pitch Period
duration of 1 cycle/flap
•If Fo = 100 Hz, then t = 1/ 100 = .01 sec
•The higher the frequency, the shorter the period.
•The lower the frequency, the longer the period.
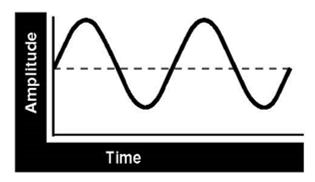
Acoustic Waveform
• a plot of the change in amplitude of the pressure wave over time.
Power Spectrum
a “snapshot” of the energy of each frequency component of the pressure wave (Pure tone has no harmonics)
•Is each flap IDENTICAL in pitch period and amplitude?
•There is variability in a person so not each flap is identical in pitch period or amplitude- we aren’t robots
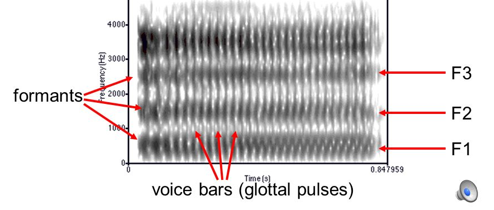
Formant Frequencies
Frequencies that are boosted by the filter (Vocal tract)
Vocal tract filter amplifies certain harmonics and dampens others in source spectrum
High Pitch
More stretch/tension/thinner in vocal folds=faster vibrations, higher pitch
Low Pitch
vocal folds shorter, thicker, less stiff -- vibrate more slowly
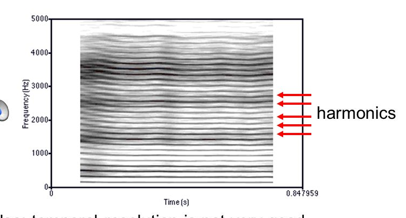
Narrow-Band Spectrogram
Time on x axis, frequency on y
-Shows harmonics but formants are less distinct
-Darkness/Thickness implies how loud it is
Wide Band Spectrogram
Shows formants better than harmonics
Fourier Theorem
•every complex periodic wave can be decomposed into its harmonic series.
Digital Measurement considerations
•Use mic with flat frequency response
•Keep set-up constant (mouth to mic distance)
•Mic at 45 degree angle
•Don’t breathe on mic!
Acoustic Measures pros and cons
•Useful: Compare to norms, Compare pre and post therapy or surgery
•Objective, but limited: No 1:1 correlation between quality and specific measures breathy, strained, etc
Fundamental Frequency Norms
•100-150 Hz males
•180-250 Hz women
•Above 300 in pre-pubescent children
Pitch Range Norms
•Adult male range around 100-500 Hz range
•Adult female range 170-750 Hz range, higher for sopranos
-Glide
Type 1, 2, 3 and Fo
Must be “regular” (type 1) to have accurate fundamental frequency value
Can’t measure Fo when type 2 because it splits into two bands on spectrogram
Can’t measure Fo when type 3 because there is no Fo on spectrogram (chaos)
When pt is very dysphonic they are type:
usually type 2 and 3
fry is often type 2
Jitter
Measured only in sustained phonation
cycle to cycle irregularity of pitch period
Normal if less than 1% (but not 0)
*Do not used for type 2 or 3
Amplitude norms
•Conversation Norm: about 70 dB
•Dynamic range: Quietest “ah” or speaking about 55 dB, Loudest/shout “Taxi!!!” or “Hey!!” about 100 dB
Shimmer
Measured in sustained phonation only
Cycle to cycle variation in amplitude
Norms: PRAAT = less than 3.8%
Only valid in Type 1 (not type 2 or 3)
Harmonics to Noise Ratio
Harmonic energy (dB compared to noise
not cycle to cycle
does not require stable Fo
Norms= greater than 20 dB (harmonics need to be louder than breathy/roughness)
In NHR, noise results from
•incomplete glottal closure= air that is not valved
•irregularity of vibration= aperiodic vibration: not a multiple of the fundamental
Cepstral Peak Prominence
Spectrum of the spectrum
Higher values = clearer or louder
Lower values= rougher or breathier
Correlates with G of GRBAS at r=.8
Can be used in connected speech
•Speech spectrum versus spectrogram
Speech spectrum X-frequency Y- amplitude
spectrogram- X- time Y- frequency
Why use My Oh My
good sentence for measures since all are voiced
Two muscles in vocal folds
•Thyro-muscularis
•Thyro-vocalis
Thyro-muscularis contraction
•always lowers pitch by ”putting slack on the string”
•Never vibrates
Thyro-vocalis contraction
•lowers pitch ONLY IN HIGH RANGE when only mucosa are vibrating.
•Raises pitch in low range, slightly, when part of vibrating mass
•Can vibrate or not vibrate- doesn't vibrate in high or breathy voice
CAPE-V
•Consensus Auditory-Perceptual Evaluation of Voice
•Standardized tasks: 3x /a/ and /i/ 3-5 seconds, 6 sentences, Running speech
•Rate qualities GRBS, pitch, loudness on 100 mm scale
Endoscopy
•Viewing vocal folds with an endoscope of any kind
•Fiberoptic endoscopic evaluation = transnasal
•Talk, eat, sing- can’t see VF very well
•Ab and adduction tasks: Cough, Coup, whistle, /ihi/ - see adduction and abduction, sniff /i/
•Stroboscopy
•Using strobe light to create illusion of glottal cycles of vibration.
•Rigid scope
•Great images of VF
•Only can say “eee” cuz that’s what flips the epiglottis back
Talbot’s Law
•Images >5/sec appear continuous to the eye
High speech digital imaging
Records at 3000 views/second
•Drawbacks: Expense, Can only store a few secs (large files), Up to recently only black and white
•Advantages: See aperiodic voices (stable Fo not needed), Higher time resolution, Can measure exact onset of phonation, More accurate diagnosis, Observe details such as discreet spasmodic events in SD
Visual Assessment for Larynx
•Describe at rest (abducted): Color, Secretions, Vocal fold edges, Lesions
•Ab and adduction: Symmetry, Complete or Partial
•Strobe: Oscillation parameters (use VALI sheet), Amplitude of vibration, glottal closure (closed configuration), mucosal wave, adynamic segments, phase closure (does closing or opening phase predominate), phase symmetry (do the folds both come together at the same time)
Ab and adduction assessment
•Fully vs partially abducted
•Tasks: phonation, sniff/i/ reps or /hihihi/, glottal coup
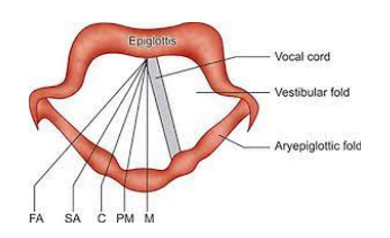
Vocal Fold positioning
•Median= midline
•paramedian” (paralysis/paresis)= 1.5mm from center paralysis
•Intermediate/cadaveric= 3.5 mm from midline
•Partial/slight abduction= 7 mm from midline
•Full abduction= 9.5 mm from midline
Glottic Closure: complete
•Touching along entire edge of vocal folds

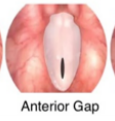
Glottic Closure: Anterior Gap
Apart anteriorly only (near anterior commissure)
Glottic Closure: Posterior Gap
apart near arytenoids

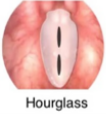
Glottic Closure: Hourglass
Lesions touch in the mid 1/3 portion of the membranous glottic
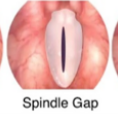
Glottic Closure: Medial Gap/Spindle
•Gap in the mid 1/3 portion of membranous glottis
Glottic Closure: Irregular
lesions different on both sides at different points

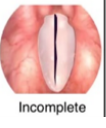
Glottic Closure: Incomplete
not touching along entire length including vocal processes
Vertical Phase symmetry
coming to center at same time
Phase closure
•% of time vocal folds are open vs closed
•Consider counting frames. Normal 40-60% open
Things to view with Stroboscopy
•Edges and color on full abduction (“V”)
•Symmetry of ab and adduction: /hi hi hi/ (rigid scope) or sniff-/i/ (flexible scope)
•Regular or irregular vibration
•Amplitude of vibration and mucosal wave (most open portion of open phase)
•Closed configuration in most closed phase frame
•Lesions: describe it, don’t diagnose a name
Aerodynamic evaluation
•How does larynx use aerodynamics (air) in phonation: Air pressure, Airflow, Relationship between these
•S, Z and MPT are actually aerodynamic tasks
•Quick and dirty measures/approximations
•Expensive equipment
S:Z Ratio
•Sustained /s/ gives idea of lung capacity
•Helps determine if it’s a vocal fold issue or lung capacity issue (they can’t get a good breath)
ratio should be about 1
s:z > 1= breathy, high flow, > 1.3 suggests disorder
S:z <1= suggests strain (longer z)
Maximum Phonation time (MPT)
•How long someone can sustain phonation on a given pitch
•Gives an idea of vital capacity, glottal valving efficiency
•“Hold out an /a/ as long as you can on a comfortable speaking pitch.”
1) “one two three for fiiiiive”
2) coach duration.
3) 3 trials
MPT norms
•Women: >17 sec
•Men: >20 sec
•Pre-pubescent children: 4-6 years: about 6 sec; 7-9 years: about 8 sec; 9-12=about 9 sec
Cycle of vocal fold vibration
folds do not open all at once, but rather the lower part first begins to open and at a later point in time the upper portion of the folds separate
bottom closes before top
Vital Capacity
Get from pt’s Pulmonary Function Testing
Normal 3-5 liters or 3000-5000 CC
Phonatory Airflow System (PAS)
•Measures Average airflow (mean flow rate= cc/sec) (how much going through vf)
•During phonation e.g. “aaaa”
•captured with flow mask
PAS norms
–Men: Average 119 cc/sec Men, range 40-320 cc/sec
–Women: mean 115 cc/sec, range 50-220 cc/sec in women
–Large range so pt needs to be severe to be outside range
–Can use for pre and post tests (surgery, treatment)
Subglottal pressure (Psub)
•Air pressure needed for phonation
Psub norms
•3 cmH20,
•conversation 6-10 cmH20,
• shouting >10
Intra-oral pressure estimates
•On “p” of “pa” or “pi”
•/p/ intra oral pressure= subglottal= lung (alveolar)
•P = voiceless (building up pressure), pressure behind lips are estimate of pressure under vocal folds, with p your vf are abducted which creates a long tube from lubes to mouth
Intra-or al pressure tools
•U-tube manometer
•Glottal enterprises electronic manometer
•Part of phonatory airflow system ($$$) (really expensive)
Laryngeal Airway Resistance
•Rlaw =Psub/flow rate
•Larger number is more strain!
-high number is not good
Rlaw values
•Paralysis=
*If Psub = 5cmH20 and Mean flow rate 500cc/sec,
*Rlaw psub/flow = 5/500=.01
•Strain- not letting a lot of air through=
*Pressure 15 cmH20, mean flow rate 150 cc/sec
*Rlaw =pressure/flowrate= 15/150=.1
Voice Handicap Scales (VHI)
measures how a voice problem influences a patient's quality of life and includes a:
–Physical subscale
–Functional subscale
–Social/emotional subscale
•Normal= around 8-12 (Behrman)
*5 point scale (0-4)
* provides mild, mod, severe score
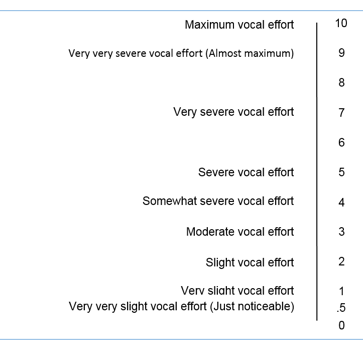
Borg CR10 Scale
•rate their level of exertion during exercise
•Categorical verbal descriptors
•Numeric ratio: Standard intervals, Absolute zero
Vocal Fatigue Index
client questionnaire
symptoms of voice fatigue that are associated with voice problems
Voice Disorders
Abnormal change in the loudness, pitch or quality of voice, the effort needed to produce voice, or the resilience of voice production
Change: not normal for the person
Effort: patient perceived
Resilience: It doesn’t last
Voice does not meet the demands of the user
Voice that draws attention to itself
Dysphonia that continues more that 3 weeks
Larynx Cartilages
Cricoid, thyroid, arytenoids, corniculate
Interarytenoid muscles (oblique and transverse)
adduct the base of arytenoids
Lateral cricoarytenoids
brings apex/vocal process together for full closure of vocal folds
Posterior cricoarytenoids
abduct vocal folds
Cricothyroids
stretches vocal folds by moving thyroid down to cricoid which changes the pitch, more stretch=higher pitch= frequency faster
aerodynamic and myoelastic forces
vocal folds are pushed apart due to subglottic pressure, vocal folds are displaced and depending on how far they are displaced determines amplitude, vocal folds are snapped back together due to them being elastic and the negative pressure created when air flows through a smaller space than it came from
Vocal Fold layers
3) Most inner (body): thryovocalis- muscle
2) Transition layer/ligament: intermediate and deep layer of lamina propria
Intermediate: Elastin fibers (rubber bands)
Deep layer: collagen fibers (string)
1) Outermost: Mucosa (cover)- 2 layers epithelum and beneath is the superficial layer of lamina propria (connective tissue), basement membrane connects the epithelum and superficial layer
Hyaluronic acid (gelatinous goo)- lots in the superficial layer of lamina propria, adds flop to the vocal folds