term 3 pos
1/511
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
512 Terms
what is PGE characterised by
diarrhoea/ weight loss
poor weight gain
hypoalbuminaemia
examples of parasitic nematode worms casusing bovine pge
ostertagia (abomasum)
cooperia and neatodrus (small intestine)
life cycle of ostertagia
adult ostertaga in abomasum
egg containing L1 larva passed in faeces
eggs hatch on pasture
develops to L3 larva, migrates from faeces to grass
L3 larva ingested by cow
this L1 to L3 development is temperature dependent. it takes up to 2 weeks or can be even slower
the prepatent period is 3 weeks, or up to 6 months if the development is arrested
typical strongyle eggs in faeces: oval, thin clear wall, bundle of cells. 80um
3rd stage larva is 750 um.
adult around 1cm long, brown. they emerge from the gastric glands and live/mate on abomasal mucosal surface
pathogenesis
where do larvae migrate to on ingestion
when do adult worms emerge
what happens if a large number of worms emerge at the same time
on ingestion larvae migrate to gastric glands of abomasum to continue development
adult worms emerge from glands around 18 days later
if a large number of worms emerge at the same time
pH increases from 2-7 as less acid produced as gastric glands are affected
pepsinogen cannot be activated to pepsin
abomasal epithelium becomes leaky
plasma proteins lost into gut lumen causing hypoalbuminaemia, weight loss and diarrhoea
what can happen to gastric mucosa
thickened, hyperpastic
raised nodules
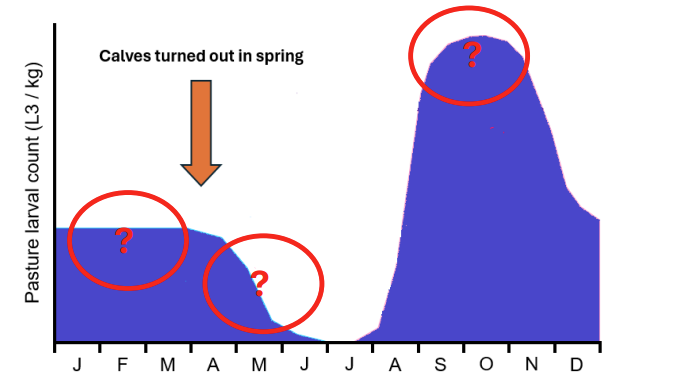
some of the L3 larvae survive on pasture overwinter
the new eggs deposited in early spring develop slowly to L3 as it is too cold
as the weather warms some existing L3 die as drier conditions and trapped in cow pats. but rate of L1 to L3 dev increases.
Then L3 increase furthe as more calves are infected and shed and eggs in faeces
what does rate of infection depend on?
host appetite
number of infective larvae (L3) on pasture
so disease is most common in calves where they are grazing permanent pasture and kept at a high stocking density
what happens to L3 is ingested in late autumn or early winter?
L4 arrest in gastric glands
then L4 resume development and emerge from glands in waves (type 2 disease)
immunity to ostertagia
slow to develop - takes the whole grazig season
may dip over winter ad re established upon turnot (2nd grazing season)
adult cattle solidly immune
epidemiology in beef herds- spring calving
calves at foot with cows
spring mortality of L3 occurs before calves eat much grass
so immun cows eat most of grass and pass few eggs
so very low disease risk
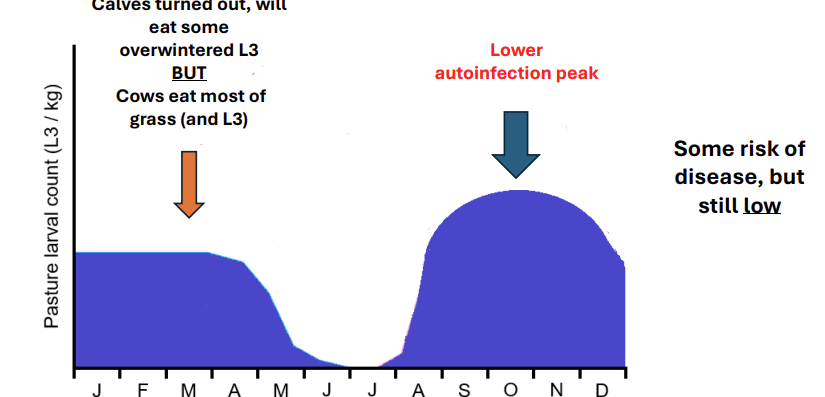
epidemiology in autumn calving
calves turned out at start of year and will eat some outwintered L3 BUT cows eat most
then lower autoinfection peak
some risk but still low
type i disease in cows
typically calves in first grazing season
mid july onwards
morbidity high, mortality low
diarhoea common (larval damage to gastric glands)
weight loss
type ii disease
typically yearlings
late winter/ spring following first grazing seasn
prevalence low, only some affected
mortality more likey
± diarrhoea with anorexia and thirst
hypoalbuminea more marked, weight loss
control of type i disease
use clean pasture
delay turnout untul after spring mortality in L3
strategic anthelmintic use
anthelmintic use
macrocyclic lactone wormers last 5 weeks eg doramectin
prepatent period for ostetagia s 3 weeks
so dosing needed every 8 weeks
options
dose and move to fresh pasture in july before autoinfection peak
but can still get disease if L3 high, increased risk of spreading resstant worms to fresh pastur
dose every 8 weeks from july and keep on same pasture
dose at spring turnout and 8 weeks later reducing autoinfection peak
give an intraruminal device before turnout which reduces autoinfection peak
control of type ii
cattle exposed to low challenge at pasture in late autumn
unlikely to require worming treatment at housing
cattle exposed to medium/ high challenge at pasture in late autumn or cattle of unknown origin
likely to require worming treatment at housing
skin and problems
thick layer of cells and sebaceous gland secretions
wounds
vector borne pathogens
mucous membraness
mucociliary escalator, peristalsis
coughing and sneezing, vomiting and diarrhoea
secretions- physical and anti microbial properties
commensal microflora
what does the innate immune sstem use for detection
uses pattern recognition receptors to detect microbial components that are itrinsically foregin
protein associated molecular patterns eg
lipopolysaccharide in gram negative
peptidoglycan in gram positive
mannose sugar in prokaryotic carbohydrate molecules
bacterial PAMPs
pathogen associated molecular patterns
pattern recognition receptor
where can they be found
what type in each
can be found in the cytoplasm, cell membrane, inside vessicles or as soluble molecules int he tissue fluid/plasma to detect PAMPS
cytoplasm: NOD receptors
membrane bound: TLRs
soluble: complement c3 protein, mannose binding lectin, c reactive protein
toll like receptors- what do these recognise
2
4
3 and 7
what are they predominantly expressed by
tlr2 recognises peptidoglycan- gram positive
tlr 4 recognises LPS - gram negative
tlr3 and 7 recognise viral nucleic acid
predominantly expressed by neutrophils and macrophages
how does innate to viral work
how are they detected
how do cells respond and what effect does this have
do not have strutural pamps
are detected by presence of double stranded rna produced during replication (not present in mammalian cells) or DNA in the cytoplasm
cells respond by producing type 1 interferon
this includes interferon alpha, beta, omega
interferons have a paracrine effect
function of type 1 interferon
resistance to viral replication
act on neighbouring
increased deradeation of viral mrna
inhibition of viral protein sythesis
increased antigen presentation of viral antigens
what is the paracrine effect
innate immunity to viruse
viruses can infect any nucleated cells
all nucleated cells can respond to viral infection by producing type 1 interferon
interferon omega can be used to treat persistent viral ifnection of cat eg FeLV/FIV
natural killer cell- large granular lymphocyte
what does it recognise
what does it release
recognise decreased levels of MHC molecules on host cells
there is decreased production during viral protein synthesis
some virus block transport to cell surface to prevent expression
this decrease is a symptom of viral infection.
the NK cell releases toxic granules killing the cell before the viral replication is complete
innate- cellular mechanisms
what is the response
how is the micro organism killed
what helps and enhances
recognition of pathogen (membrane, vesicular and cytoplasmic PRR)
response is phagocytosis and inflammation
phagocytic organisms attach to the organism and use pseudopodia to capture it forming a phagosome
then it stimulates a respiratory burst and toxic metabolites (eg oxygen free radials, hydrogen peroxide) are pumped into the vesicles to kill the micro organism
subsequent fusion of the lysosomes with the phagosome (phagolysosome) releases proteolytic enzymes and anti microbial mediators (defensins and lactoferrin)
increasingly acidic pH results in digestion of the microorganism
enhanced phagocytosis (opsonisation) can be achieved with the help of the antibody IgG and or complement CC3b
destruction of endocytosed organisms can be enhanced by stimulation of cytokines released by T helper cells
innate- humoral mechanisms
recognition of pathogen- soluble PRR
response: killing of foreign organism, enhacned phagocytosis and inflammation
tlr

what could NOD2 receptor defect cause
crohns in man
ibd or anal furunculosis in german shepherd
what does recogn tiion of bacteria by macrophage tlr lead to
phagocytosis and inflammatory resposne
respiratory burst
what is it
what is formed
enhanced cellular aeorbic metabolism
reactive oxygen intermediates are formed
superoxide anion
hydroxyl radicals
hydrogen peroxide
this isthe oxygen dependednt mechanism of bacteiral killing
lysosomes
3 types
defensins
cationic anti microial peptides that damage bacterial cell wall
lactoferrin
binds and chelates free iron, which is required for bacteiral growth
acid proteases
digestive enzymes active at low pH
inflammatory mediators-histamine
what is it released by
produced by mast cell degranulation in tissues
anti histamine
pro inflammatory cytokines
examples
what are they synthesised by
tumour necrosis factor a
synthesised predominantly by wbc and macrophages
corticosteroids
lipid mediators of inflammation
prostaglandin and leukotrienes
derived from arachidonic acid by action of cycloocygenase and lypoxygenase enzyme
nsaid
localised effect
inflammation
systemic
hypothalamus
fever
liver
acute phase response
bone marrow
neutrophil and monocyte mobilisation
speed up production
acute phase response
where are the proteins produced by in response to what
examples
what do they do
are they specific or non
acute phase proteins are produced by the liver in response to pro inflammatory cytokines
serum amyloid protein, C reactive protein and mannose binding lectin stick to bacterial cell walls
act as opsonins to enhance phagocytosis and stimulating complement activation
but are non specific
complement
where are complement proteins found
what steps do they form
what is the end product
complement prtoens are found in the blood
series of enzyme activation steps forming an aomplification cascade
small amount of activation is amplified to generate a large response
similar in nature to clotting cascade but with a diff trigger and outcom
the end product of the cascade is the polymerisation of C9 monomers to form a C9 polymer forming a membrane attack complex
a tube like structure that create holes in the cell walls of bacteria causing them to lyse
inactive C3 in the blood dissociates into C3a and b in the presence of bactiera- it is a pro enzyme
C3b is deposited onto the surface of the microbe and acts as an enyzyme to catalyse the formation of the MAC and also act as an opsonin (phagocytic cells express c3b receptor)
C3a binds to receptors on local tissue mast cells triggering degranulation and stimuating a inflammatory response
what are 3 examples of physical barriers
thick stratified squamous epithelium (skin and lower urinary tract)
mucociliary escalator (resp tract)
peristalsis, vomiting and diarrhoea when necessary (alimentary)
example of biochemical barriers
lactic and fatty acis in sebum from sebaceous glands of skin
enzyes
acid in stomach
antibacterial peptides eg defensin
how do commensal organisms provide protection
compete with organisms for space
provide natural antibiotic
what do gamma delta t cells do
react to stress proteins that are upregulated on the surface of infected mucosal epithelial cells
overall oucome of complement activation
lysis of the bacteria by the MAC
enhacend phagoytosis of bacteria coated in complement proteins C3b
inflammation at the site of complement activation C3a
where are these prrs located
TLR 2
TLR 4
TLR 5
TLR 9
NOD2
peptidoglycan
lipolysaccharide
flagellin
prokaryotic DNA
muramyl dipeptide
localised efects of inflammatory cytokines
vasodilation
increased capillary permeability
recruitment and influx of white blood cells
immunohistochemistry
prepare cells in tissue
apply a specific antibody against a target eg virus antigen
anibody chemically modified to have enzyme to form antibody-enzyme conjugate
wash the slide to get rid of unbound antibody
add DAB substrate- colourless which changes to brown ppt with presence of enzyme
look under microscope to find positive
Fluoresecent antibody test
antibody is labelled with a fluorophore
can see antibody binding to the target under a fluorescence microscope
enzyme linked immuoabsorbent assay
can be used to detect either antigen or antibody
if testing early test for antigen at site of infection, will still be in lag phase
if testin more than 5 days post exposure test for antibody in serum (LOG phase) and retest 2-3 weeks later (plateau phase)
sandwich elisa method
elisa plate
add a specifc capture antibdy at the bottom which binds
add in antigen in sample whch bins to antibody
add another antibody which is also specific. this has een chemically modified with enyme
add substrate—>colour change
elisa method for detection of antibody in serum
add antigen at bottom
add take blood sample and serum
if anitbody present it will bind to antigen
add a secondary antiboy (conjugate)
colourchange
haemolytic bacteria
produces a toxin that damages cells
does NOT cause haemolysis ad anaemia
can test for this by culturing samples on sheep blood agar where haemolysis can be observed in the petri dish
these pathogens will produce the same toxin at the site of infection causing damage to the local cells
titre definition in serology
the greatest dilution of serum that still gives a positive result for the presence of antibodies in the test
bacteria vs virus culture
bacteria need nutrient agar at 37
viruses require cells
need to culture cells in the lab that the virus is able to infect and replicate within
species specificity and tissue tropism will dictate the cll type rquired for virus isolation
opportunistic pathogen
a pathogen which does not normally cause disease but does when the hosts immune system is compromised
fluorescent antibody test
where can the pathogen be
epithelial tissue
cytoplasm
tissue fluid
vesicle- endosome
innate
what receptors are involved
specificity
oldest
tries to keep foregin out
if organism breach external barriers recognise that infection is present and respond quick
pattern recognition receptors
neutrophils and tissue macrophages target bacteria
eosinophils and tissue mast cells target parsites
recognition of commonmicrobial molecules that are intrinsically foregineg peptidocycan of bacteria cell wall
receptors for these are broadly reactive but not very specific
pathogen associated molecularpttens
lipopolysaccharide= gram -ve
peptidoglycan= gram positive
viruses do not have obvious pamps
some bacteria produce capsules to hide them
innate immunity is no longer sufficient to protect thehost from all infections
we need another strategy- adaptive immunity
adaptive
immune resposne of higher species
much more efficient but slower to react
helps innate immune mechanism to work better
anitgen receptors are expressed by lymphocytes- recognition of foregin antigens and have a highly specifc detection systems
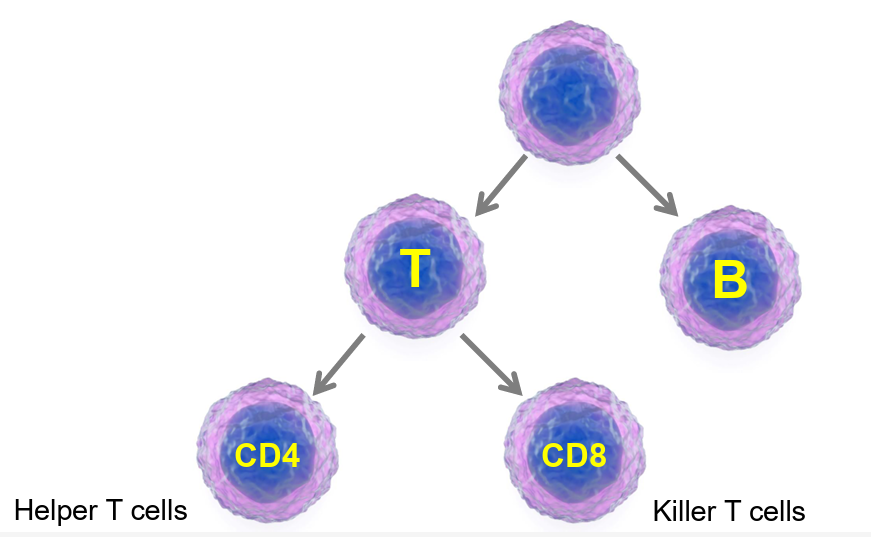
lymphocytes- t and b cells
primary role in dealing with viruses
also hep the cells of innate immunity to fight bacterial and parasite infections
what is an antigen
usually a structural protein of a pathogen eg a spike protein
lymphocyte receptors recognise the shape of a small region of the antigen
this is the epitope
lymphocyte family tree
b cell receptor
bind to whole antigen on the surface of a pathogen in the ecf
t cell
recognises digestedantigen displayed ont he surface of other cell
proten is degraed to peptides
peptides are displayed on surface of cell hich cna be recognised by tcr
immunological synapse
when an immune cell creates contact with an antigen
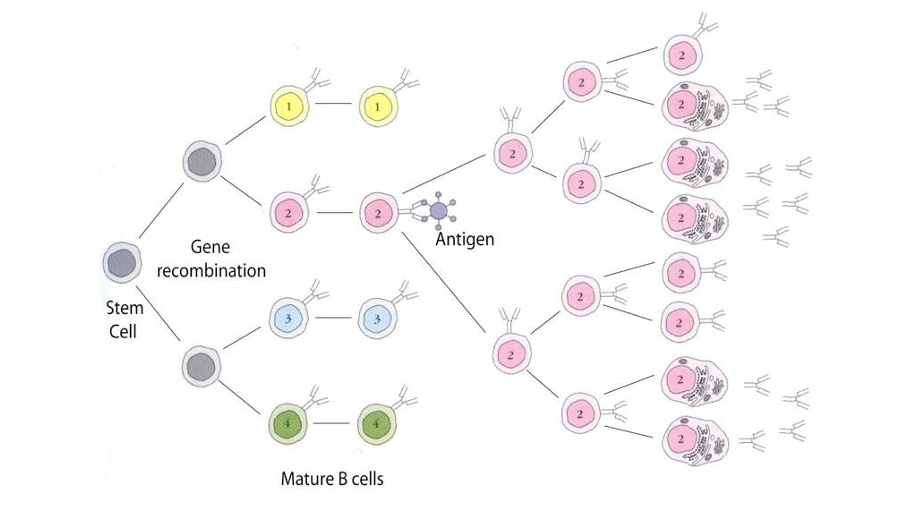
lymphocyte development
when a lymphocyte develops in the bone marrow it has to design its own unique antogen receptor
they juggle their genes to generate a large amoutn of diversity
constant and variable with antigenic epitope
clonal selection
what do b cells do
produce antibody eg immunoglobulin, gamma globulin which stick to pathogens
what do cd4 helper cells do
produce cytokines which activate other cells
cd8 killer cells
seek and destroy virus infected cells
b cells resposne to infection
rcognition of antigen on surface of pathogen
clonal epansion
differentiation to plasma
produciton to anitbody
antibody
what are they
what do they do once bound
what are they secreted by
where are they secreted and why
antigen binding protiens
soluble versions of the b cell surface antigen receptor
targets the external surface of the pthogen
once bound
inactivate/neutralise
attract phagocytic cells
triggers innate killing response
secreted by plasma cells (drived from B)
secreted into the lymph node where they can bind to their specific antigen in the ECF- cannot cross cell membrane
CD4+T lymphocyte
are helper t cells
some make cytokines to activat emacrophaces
some make cytokines to assist b cells in making antibodies- B cell growth fators
CD8+T lymphocyte
killer t cells
kills infected
immunological memory
after recovery we are left with an expanded population of lymphocyte clones
these memory lymphocytes have a long lifespan
immune syste respond much mor quixkly and efficiently
instead of becoming effector cells they become quiescent
detection of infection
some structures are intrinsically foreign eg lipopolysaccharide and peptidoglycan and pattern recognition receptors have evolved for their detection
typically found on the surface of wbc for detection of infection in the extraceluular fluid or in the cytoplasm for detection of infection i the intracllular fluid
adaptive detects protein structure and shape to differentiate between self and foreign
lymphocytes express receptors on their surface that are designed to recogn ise foreign proteins bvy shape (antigens)
lymphocyte development
a large number of diversity is generated by random juggling of receptor variable genes ton produce a receptor nprotein
so each lymphocyte expresses uniquely shaped antigen receptor
once designed, each lymphocyte will express many copies of its antigen receptor
B vs t
the B cell antigen receptor is designed to detect epitopes of the whole antogen on the surface of pathogens located in the extracellular fluid
the t cell receptor is designed to recognise fragments of digested antigen eg peptides that are displayed on the surface of other cells in association wiht specialist antigen presenting molecules -MHC
what is clonal selection
during an infection, when a host is exposed to foreign antigen, only a small number of specific lymphocytes will react
must proliferate to generate many copies
usually occurs in the lymph nodes
what are parasites killed by
toxic mediators released by eosnopils and mast cells when they degranulate
how are viruses killed
a coordinated attack by lymphocytes by the acion of antibody and killer T cell
antibodies
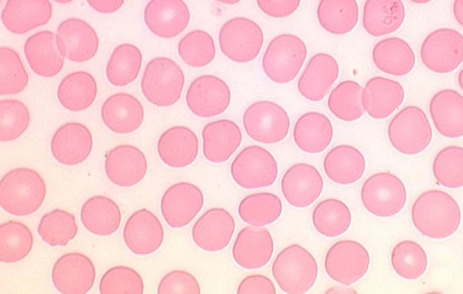
erythrocytes
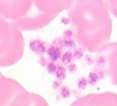
platelet
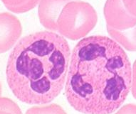
neutrophil
eosinophil

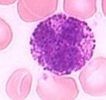
lymphocyte
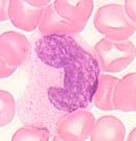
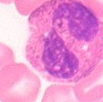
monocyte
basophil
erythryocyte and leukocyte staining
cytoplasm of erythryoctres stains pink
that of leukocytes is blue grey with cytoplasmic granules staining grey/pink, red/pink or blue/purple
what do neutrophils, eosinophils and basophils contain in their cytoplasm
granules
in which cells are the nuclei lobed
neutrophils, eosinophils and basophils