OCD Master Set
1/34
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
What is OCD?
A condition characterised by obsessions and/or compulsions.
Obsessions= cognitive
Compulsions= behavioural
Symptoms of OCD
Repetitive intrusive thoughts, anxiety reducing behaviours.
How common is OCD?
2% of population
DSM-V OCD
The DSM-V recognises OCD and a range of related disorders. What the disorders all have in common is repetitive behaviour accompanied by obsessive thinking:
Related disorders:
Trichotillomania
Hoarding Disorder
Excoriation disorder
What is Trichotillomania
When someone can't resist the urge to pull out their hair.
Hoarding Disorder
A persistent difficulty discarding or parting with possessions because of a perceived need to save them. A person with hoarding disorder experiences distress at the thought of getting rid of the items. Excessive accumulation of items, regardless of actual value, occurs.
What is Excoriation disorder
A mental illness related to obsessive-compulsive disorder. It is characterized by repeated picking at one's own skin which results in skin lesions and causes significant disruption in one's life (also referred to as chronic skin-picking or dermatillomania)
OCD Cycle
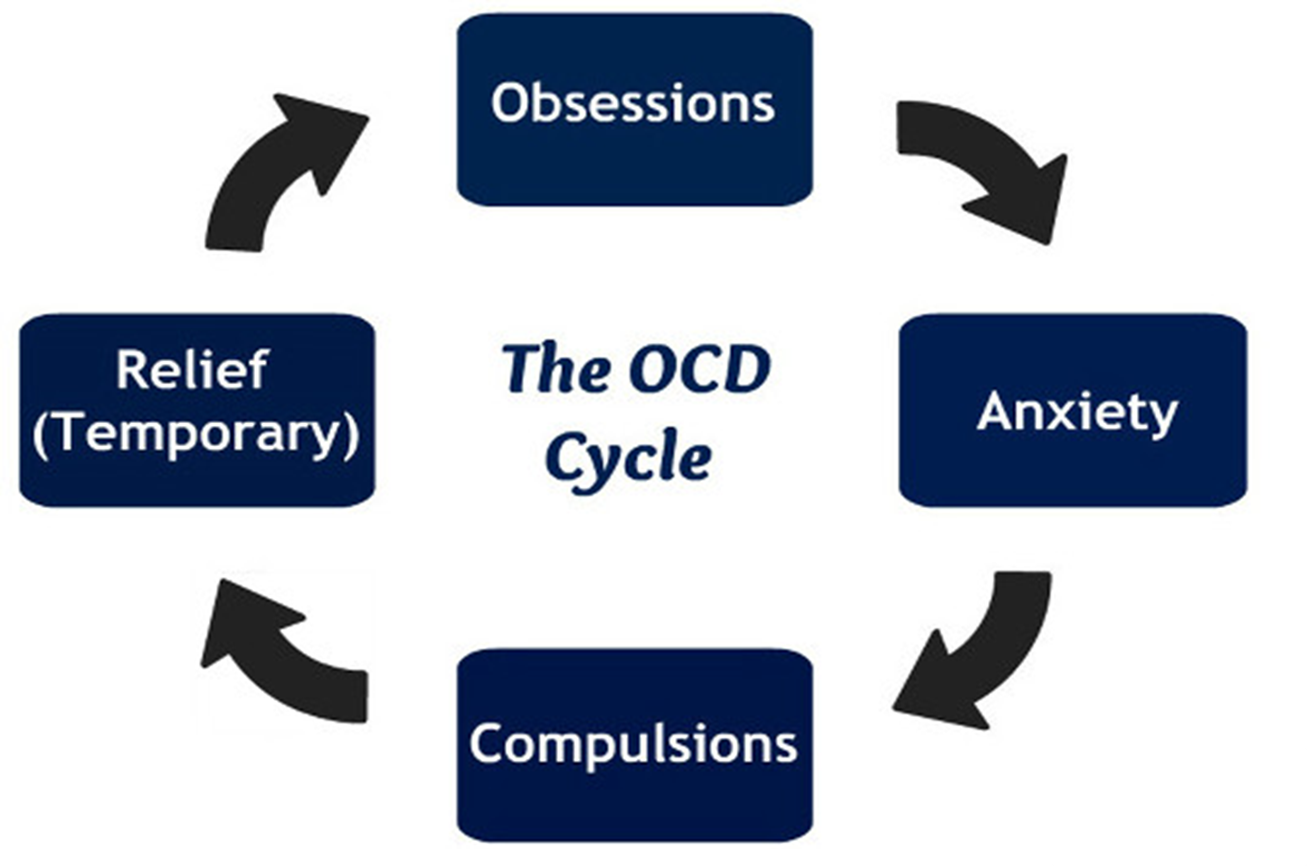
What are compulsions?
Unwelcome thoughts, images, urges, worries or doubts that repeatedly appear in your mind. They can make sufferers feel very anxious or uncomfortable.
Behavioural Characteristics of OCD
Compulsions are repetitive: Suffers feel compelled to repeat behaviours e.g. handwashing, praying, tidying, ordering items.
Compulsions reduce anxiety: Compulsive handwashing is carried out as a response to an obsessive fear of germs. Therefore compulsions are seen to manage to sufferers’ anxiety.
Emotional Characteristics of OCD
Anxiety and Distress: The urge to repeat a behaviour creates overwhelming anxiety. Obsessive thoughts are unpleasant and frightening.
Accompanying Depression: OCD is often comorbid with depression so there is also likely to be low mood and anhedonia.
Guilt and Disgust: Sometimes OCD involves emotions such as irrational guilt e.g. for example over minor moral issues, or disgust which may be directed against something external like dirt or at the self.
Cognitive Characteristics
Obsessive thoughts: Thoughts that recur over and over again. They vary from the person to person but are always unpleasant and maladaptive. e.g. the door was left unlocked.
Cognitive strategies to deal with obsessions: For example, a religious person tormented by guilty may respond to praying or meditating. This may help the person but will look abnormal to others.
Insight into excessive anxiety: OCD sufferers are aware their obsessions and compulsions are irrational. OCD sufferers experience catastrophic thoughts about the worse case scenarios that might occur if their anxieties were justified.
Family Studies
Lewis (1936) found that 37% of OCD patients had parents with OCD and 21% had Siblings with OCD.
This suggests OCD is passed on in genetic vulnerability, not certainly
According to the diathesis-stress model, Certain gever leave Some people more villnerable to Supper a mental disorder, but it's not certain - some environmental stressor is recassary. to trigger it.
Candidate genes (Lewis 1936)
Researchers have identified genes, which reale vulnerability for OCD, called candidate genes.
Some of these genes are involved in regulating the development of the seratonin systemic.
OCD is Polygenic
This means that OCD is not caused by one sole gene, but several genes are involved
Taylor (2013) analysed the findings of previous studies and found evidence that of may up to 230 genes involved. These genes related to the the action of dopamine and serotonin- both have roles in regulating mood
Different types of OCD Explanation
OCD is aetiologically heterogenous, meaning the origin (aetiology) of OCD has different causes (heterogenous)
There is also some evidence to suggest that different types of OCD variations may be the result of particular genetic variations
The role of Serotonin
Low levels of serotonin impact the normal transmission of mood-relevant information, leading to difficulties in emotional regulation and cognitive processes such as memory and decision-making.
Decision-making systems
Some cases of OCD seem to be associated with impaired decision making.
This may be associated with the with abnormal functioning on the lateral of samtal lobe in the brain.
There is also evidence that an area called the left parahippocampal gyrus functions abnormally in OCD.
Twin Studies
Nestadt et al. (2010) reviewed previous studies. and found that 68% of Identical twins shared OCD as opposed to 31% of non-identical twins
Limitation of candidate genes
For many candidate genes Carnot fin down all genes involved (atm) Only increase OCD risk fractionally
Environmental risk factors.
Cromer et al. 2007 found that over half the OCD patients in their sample had a traumatic event in their past, and that OCD was more severe in these with multiple traumas.
Limitations of environmental risk factors
Not a full explanation, not entirely genetic in nature
Supporting evidence of the biological explanation
Some anti-depressants are effective in reducing OCD symptoms, suggesting Serotonin is involved:
Also, OCD symptoms form a part of a number of other conditions are biological in nature e.g Parkinson’s (Nestadt et al 2010)
Limitations of the biological explanation
Not clear exactly what neural mechanisms are involved. (Should not assume neural conditions cause OCD)
The serotonin OCD link may simply be Co- morbidity with depression.
Strengths of the biological explanations
One of the best sources of evidence for the importance of genes is twin studies. Nestadt et al. (2010) reviewed previous studies and found that 68% of identical twins shared OCD as opposed to 31% of non-identical twins.
Limitations of the biological explanation
Although twin studies strongly suggest that OCD is largely under genetic control, psychologists have been much less successful at pining down all the genes involved. One reason for this is because it appears that several genes are involved and that each genetic variation only increases the risk of OCD by a fraction.
It seems that environmental factors can also trigger or increase the risk of developing OCD (the diathesis-stress model). For example, Cromer et al. (2007) found that over half the OCD patients in their sample had a traumatic event in their past, and that OCD was more sever in those with more than one trauma.
Strengths of the neural explanations
There is evidence to support the role of some neural mechanisms in OCD. For example, some antidepressants work purely on the serotonin system, increasing levels of this neurotransmitter. Such drugs are effective in reducing OCD symptoms and this suggests that the serotonin system is involved in OCD. Also, OCD symptoms form part of a number of others conditions are biological in nature Parkinson's Disease (Nestasdt et al., 2010).
Limitations of the neural explanation
Studies of decision making have shown that these neural systems are the same systems that function abnormally in OCD (Cavedini et al. 2002). However, research has also identified other brain systems that may be involved sometimes but no system has been found that always plays a part in OCD.
There is evidence to suggest that various neurotransmitters and structures of the brain do not function normally in patients with OCD. However, this is not the same as saying that this abnormal functioning causes the OCD.
Drug Therapy
Drug therapy aims to increase or decrease, levels of neurotransmitters, which increase or decrease certain behaviours. Low levels of serotonin are associated with OCD.
Drug treatments work to increase serotonin levels
What does SSRI stand for?
Selective Serotonin Reuptake Inhibitor
SSRIs
Most commonly used antidepressants to treat OCD
SSRI's work by Mocking (or inhibiting) reuptake.. meaning more serotonin is available to pass wee angers between nearby neurons.
Prevents it from being reabsorbed into the sending cell
Can take 3-4 months to have any real impact on symptoms
Fluoxetine is a key SSRI
Combining SSRIS & other treatments
Often used alongside CBT
Drugs help reduce symptoms, increasing engagement with CBT
Some patients respond best to CBT alone, whilst others benefit more from drug like Fluoxetine
Ocaissonally, other dogs are prescribed alongside SSRIS
Alternatives to SSRIS
If SSRIs aren't working, it can be combined with Tricyclics & & Clomipramine. e.g. Clomipramine
These have more severe side effects
SNRIs aka Serotonin-noradrenaline reuptake Inhibitors
New, Same effects as SSRI
Strengths
Soomro et al. (2009) reviewed studies which compared SSRIs to placebos when treating OCD. All 17 studies showed better results for the SSRIs than the placebos. Effects are even greater when the SSRIS are combined with other forms of treatment like CBT. Typically symptoms decline for 70% of those taking SSRIS. Of remaining 30%, alt drugs and psych. treatments are likely to be effective.
Drug treatments are cheaper than other psychological treatments. Using drugs to treat OCD is therefore good value for a public health system. + when compared to other drugs, SSRIs are also non-disruptive to patients' lives. For some patients, they can take drugs until they feel better without the need to engage with the hard work needed for other forms of therapy like CBT.
Limitations
Although drugs can be helpful, a significant minority will get no benefit. Some also suffer side-effects. For example, those taking Clomipramine, side-effects are more common and can be more serious. More than 1- in-10 patients suffer erection problems, tremors and weight gain. More than 1-in- 100 become aggressive and suffer disruption to blood pressure and heart rhythm.
OCD is widely believed to be biological in origin therefore it makes sense that treatments are biological. However, some forms of OCD can have a range of other causes i.e. whereby OCD is a response to a traumatic life event.
Although, SSRIs are fairly effective and any side-effects will probably be short term, like all drug treatments they have some controversy attached. For example, some psychologists believe the evidence favouring drug treatments is biased because the research is sponsored by drug companies who do not report all the evidence (Goldacre, 2012).